

-
肺癌在我国的发病率逐年上升,美国国家肺癌筛查试验(NLST)结果显示,低计量肺部CT筛查能有效降低肺癌的病死率达20%[1]。孤立性肺结节(solitary pulmonary nodule,SPN)是早期肺癌的常见影像学表现,对于偶发性肺部结节进行恶性风险性评估具有重要的临床意义,既可以实现恶性结节的早发现、早治疗,又可以避免对良性结节进行不必要的手术,确定SPN的恶性风险度是制定肺结节下一步治疗策略的关键[2]。本文通过分析43例SPN病人的一般临床资料及结节的CT征象,比较良、恶性结节的组间差异,筛选出独立影响因素,旨在提高SPN的鉴别诊断能力,更加合理地提出临床下一步处理意见。
-
回顾性分析我院2016年5月至2018年6月收治的43例SPN病人,其中男27例,女16例;发病年龄17~84岁;结节最大径0.7~3.0 cm;随访时间最长者约1年。病例纳入标准:肺内SPN最大径≤3.0 cm,临床手术、病理资料或影像随访资料完整,能够明确诊断肺部结节的良恶性。排除标准:肺内结节>3.0 cm,肺内完全钙化结节,初次就诊时已有肺内或远处转移的恶性SPN病例。
-
采用Philips Brilliance 16排螺旋CT机行胸部薄层平扫或增强扫描。扫描前行呼吸深度及频率训练,病人仰卧位,在深吸气末屏气扫描,扫描范围自胸廓入口至肋膈角水平。增强扫描使用高压注射器经肘静脉注入碘普罗胺(62.34 g/100 mL),用量为80~100 mL,注射流率为3.0~4.0 mL/s。描参数为120 kV,180 mAs,旋转速度0.5 s,准直器16×0.75 mm,螺距0.938,矩阵512×512,扫描层厚2~5 mm,重建层厚0.8 mm。扫描数据传入EBW V4.5工作站进行容积重建(volume reproduction,VR)、多平面重组(multiplanar recombination,MPR)、最大密度投影(maximum intensity projection,MIP),并在浙江格林蓝德信息技术有限公司的PACS工作站进行重建分析阅片。主要观察肺结节的形态特征(如分叶征、毛刺征、边缘是否有平直边)、密度特征(成分、空泡征、强化方式)及与周围组织的关系(血管集束征、支气管征、胸膜凹陷征)。
-
归纳上述43例SPN的各CT征象,由2名有多年肺部疾病诊断经验的主治医师独立分析各结节的影像特征、测量结节大小,分析结果或测量数据存在争议时由2名医师共同商讨后得到统一结果。
-
采用t检验、χ2检验和logistic回归分析。
-
本组43例病人共43枚SPN,经临床和病理证实良性结节18例(41.9%),恶性结节25例(58.1%)。其中良性结节经病理证实6例(结核及炎性假瘤各2例,错构瘤及曲霉菌感染各1例);经随访病灶吸收11例(考虑感染性病变);另1例白血病病人治疗过程中结节不断变化,临床证实为霉菌感染。恶性结节中经手术病理证实24例(腺癌11例,微浸润腺癌2例,原位腺癌1例,鳞癌5例,小细胞肺癌4例,转移性腺癌1例);1例肺部结节1年后复查结节显著增大伴厚壁空洞,两肺多发转移灶,考虑肺癌。
-
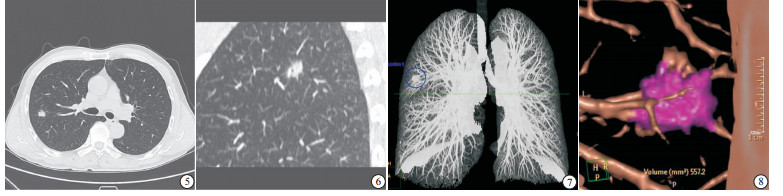
43例SPN中32例行平扫+增强扫描,11例为平扫。其中纯磨玻璃结节4例、部分磨玻璃结节11例、实性结节28例。典型病例:病例1,女,68岁;2017年5月30日行CT扫描,示右肺上叶前段纯磨玻璃结节,边界模糊;2017年9月2日CT扫描图像及MPR、VR图像显示,磨玻璃结节大小无变化,结节边缘肺血管走形不自然,结节内肺血管增多、增粗,表现“血管集束征”; 术后病理为原位腺癌(见图 1~4)。病例2,男,55岁;CT扫描示右肺上叶后段结节灶,结节后缘为平直边;MPR矢状位图像示结节边缘见短毛刺,内有空泡征;MIP及VR图像示结节与肺纹理的关系;术后病理证实为结核性肉芽肿(见图 5~8)。
图 1 病例1影像学检查图像

图 5 病例2影像学检查图像
-
单因素分析结果显示,病人为女性、结节有分叶、毛刺、胸膜凹陷,支气管征及血管集束征的结节恶性率较高(P < 0.05~P < 0.01),而结节出现平直边的病人结节良性率较高(P < 0.05);病人发病年龄、结节最大径、长短径比值、空泡征、结节成分对结节的良恶性影响无统计学意义(P>0.05)(见表 1)。以单因素分析中有统计学意义的性别、分叶征、平直边、毛刺征、胸膜凹陷征、支气管征、血管集束征为自变量进行多因素logistic回归分析,结果显示,毛刺征为恶性SPN的独立危险性因素(P < 0.05),有平直边为良性SPN的独立保护性因素(P < 0.05)(见表 2)。
因素 SPN χ2 P 良性 恶性 性别 男 15(55.56) 12(44.44) 5.59 < 0.05 女 3(18.75) 13(81.25) 分叶征 有 4(21.05) 15(78.95) 6.06 < 0.05 无 14(58.33) 10(41.67) 毛刺征 有 4(19.39) 19(82.61) 12.16 < 0.01 无 14(70.00) 6(30.00) 平直边 有 8(72.73) 3(27.27) 4.21 < 0.05 无 10(31.25) 22(68.75) 血管集束征 有 3(17.65) 14(82.35) 6.77 < 0.01 无 15(57.69) 11(42.31) 支气管征 有 2(15.38) 11(84.62) 5.37 < 0.05 无 16(53.33) 14(46.67) 空泡征 有 2(22.22) 7(77.78) 0.93 >0.05 无 16(47.06) 18(52.94) 胸膜凹陷 有 5(25.00) 15(75.00) 4.37 < 0.05 无 13(56.52) 10(43.48) 结节成分 磨玻璃 2(50.00) 2(50.00) 部分磨玻璃 2(18.18) 9(81.82) 3.67 >0.05 实性 14(50.00) 14(50.00) 年龄(x±s)/岁 57.83±14.80 64.12±10.18 1.65* >0.05 最大径(x±s)/cm 1.67±0.52 1.99±0.78 1.52* >0.05 长短径比值(x±s) 1.33±0.24 1.24±0.27 1.13* >0.05 *示t值;()中为百分率/% 表 1 影响SPN良恶性的单因素分析
自变量 β Waldχ2 P 0R OR 95% CI 性别 -1.500 1.712 >0.05 4.481 0.474~42.373 分叶 0.287 0.052 >0.05 0.751 0.064~8.868 毛刺 2.242 4.022 < 0.05 0.106 0.012~0.950 胸膜凹陷 1.271 1.562 >0.05 0.281 0.038~2.060 气管征 1.887 2.318 >0.05 0.152 0.013~1.720 血管集束征 0.407 0.106 >0.05 0.665 0.057~7.768 平直边 -2.425 3.943 < 0.05 11.307 1.032~123.888 表 2 SPN良恶性的多因素logistic回归分析
-
2017年Fleischner学会基于国际多学科的研究进展,针对肺部偶发结节提出了最新的处理指南白皮书,中国肺癌早诊早治专家组曾结合国内外肺部结节处理指南及在我国人群及临床筛查中的应用提出了《中国肺部结节分类、诊断与治疗指南(2016年版)》。目前肺部偶发结节主要依赖定期随访,由多学科医师会诊,决定是否需要进行进一步检查(包括CT增强扫描、PET-CT扫描、纤维支气管镜、经皮肺穿刺活检)明确诊断,以及采取什么方法进行治疗。但良性及恶性SPN的影像特征存在部分重叠,往往鉴别困难,不利于恶性结节的早发现、早治疗[3]。
OST等[4]曾对肺部SPN的各项检查进行过全面系统的成本效益分析,认为诊断SPN成本效益最高的检查手段为CT,其对恶性SPN总的诊断敏感性为96.5%,特异性为55.8%。根据GOULD等[5]的报道显示,恶性SPN的独立危险因素为发病年龄、病人有吸烟及戒烟史、结节直径是恶性SPN的危险因子。NELSO筛查的7 155例受试者发现非钙化结节9 681例,容积 < 100 mm3的结节恶性比例为0.6%,100~300 mm3的比例为2.4%,而>300 mm3为16.9%,随着结节体检增大,恶变率增加[6]。陈康等[7]研究189例肺部SPN后认为结节大小、毛刺、胸膜凹陷征等在良恶性结节中差异有统计学意义。王越等[8]通过相关研究发现,病人年龄、分叶征、胸膜凹陷征与孤立性肺结节良恶性有关,其中年龄、分叶征是判断SPN良恶性的独立影响因素。本研究显示,病人性别、结节分叶征、有无平直边、毛刺征、胸膜凹陷征、支气管征及血管集束征在SPN良恶性之间差异有统计学意义,毛刺征为恶性SPN的独立风险因素,有平直边为良性SPN的独立保护性因素;与国内外各研究报道大体符合,略有差异。本组SPN中女性病人恶变率更高(P < 0.05),考虑纳入研究的恶性SPN中肺腺癌占比高(14/25),张著学等[9]通过119例肺腺癌表皮生长因子受体(EGFR)基因突变的研究得出肺腺癌中EGFR基因突变率高,可能是肺腺癌发生的早期事件,而EGFR基因突变以女性多见。目前尚不能证明结节大小、成分及病人年龄在良恶性SPN中存在差异,研究存在局限性,主要是由于收集病例数不足,另外纳入研究的病例多数为经过各科室层层筛选的手术病例,良性征象的病例存在随诊时间跨度不足、随诊过程中病例丢失而未被纳入研究,良恶性征象偏重不明确者进入上级医院继续治疗,导致收集的病例存在偏倚。
本研究在良恶性SPN中差异有统计学意义的CT征象:分叶、毛刺、胸膜凹陷、血管集束征等间接反映了病灶的病理学特征。恶性结节的分叶征是因肿瘤各部位瘤细胞分化程度不同,生长速度不一致所致,较大的结核球可由多个小病灶融合而形成分叶征表现,肺癌的分叶征较良性结节更多见,本组SPN中恶性结节分叶征15例(60.00%),比例明显高过良性结节4例(22.22%),差异有统计学意义。周围型肺癌侵袭性强、收缩性强,癌细胞侵犯肺间质,引起出血、渗出及瘤内瘢痕收缩使小叶间隔重排而形成短毛刺,并可使邻近胸膜牵拉凹陷,少数良性结节也可见上述征象,但肺癌可使凹陷的胸膜延伸进入肿瘤内,肿瘤表面形成“胸膜凹陷切迹”[10]。血管集束征由于恶性结节的侵袭性及富血供特征所致,肿瘤组织向血管支气管鞘生长,牵拉邻近血管向瘤体集中,富血供肿瘤诱发形成新生血管或供血动脉代偿增粗。
本组43例病人32例行增强CT检查,给SPN的定性诊断带来帮助;虽然有研究[11-12]指出非增强CT同样可以显示重要的异质性特征,笔者认为增强图像显示结节的血管集束征更优,特别是实性结节内部的血管改变单纯CT平扫不能显示,结合结节的强化方式,增强CT在SPN的鉴别诊断中仍然是必要的。本研究结果显示SPN存在平直边为良性结节的保护性因素,可能是由于结节的生长特性及侵袭性决定,良性结节一般收缩力弱,无各部生长速度不一的特征,致病因子损伤肺组织同时有修复的过程,病灶边缘有纤维增殖灶形成;另外良性结节侵袭性弱,肺结缔组织(如肺泡间隔、小叶间隔)阻挡病灶进展,具体病理特性有待进一步证实。
良、恶性SPN各影像征象存在一定重叠,如肺炎吸收不完全病灶机化后纤维组织增生产生的“假性”肿瘤征象等,国内外相关研究报道也存在一定的差异,且目前尚未建立标准的SPN各征象诊断模型[13-14]。影像及临床医师对病人的影像征象、临床资料及动态随访结果综合客观的评价是制定SPN下一步处理方案的重要前提,有恶性倾向者应积极尽早的行手术治疗。
孤立性肺结节影像学特征的logistic回归分析
Logistic regression analysis of imaging features of solitary pulmonary nodule
-
摘要:
目的采用logistic回归分析对良、恶性孤立性肺结节(SPN)的临床及影像征象进行恶性风险因素分析,以提高早期肺癌的检出率。 方法回顾分析43例SPN病人的临床及影像资料,先进行单因素分析,筛选出良、恶性组差异有统计学意义的因素,代入二元logistic回归分析进行多因素分析,得出良、恶性SPN的独立影响因素。 结果43例病人共43个SPN,良性组18例(41.9%),恶性组25例(58.1%)。孤立性肺结节良恶性的单因素分析显示,病人为女性、CT影像中结节有分叶、毛刺征、血管集束征、支气管征、胸膜凹陷征和无平直边的结节恶性率较高(P < 0.05~P < 0.01);多因素logistic回归分析结果显示,毛刺征为恶性SPN的独立危险性因素(P < 0.05),有平直边为良性SPN的独立保护性因素(P < 0.05)。 结论良、恶性SPN的各影像征象存在重叠,毛刺征为恶性SPN的独立危险因素,而有平直边为良性结节的独立保护性因素。 -
关键词:
- 孤立性肺结节 /
- 影像学 /
- logistic回归分析
Abstract:ObjectiveTo investigate the clinical characteristics and imaging signs of malignant solitary pulmonary nodule(SPN) to analyze the malignant risk factors, in order to improve the early detection rate of lung cancer. MethodsThe clinical and imaging data of 43 patients with SPN were analyzed using single factor analysis, and the statistical significance factor between benign and malignant groups was screened.These factors were multiplely analyzed using binary logistic regression analysis, and the independent influencing factors in benign and malignant SPN were screened. ResultsAmong 43 patients with SPN, 18 benign cases(41.9%) and 25 malignant cases(58.1%) were identified.The single factor analysis of benign and malignant solitary pulmonary nodules showed that the malignant rates of nodules with lobulation, burr sign, vascular cluster sign, bronchial sign, pleural indentation sign and no straight edge in CT images in female patients were higher(P < 0.05 to P < 0.01).Multiple-factor logistic regression analysis showed that blur sign was the independent risk factor of malignant SPN(P < 0.01), and the straight edge was the independent protective factor of benign SPN(P < 0.05). ConclusionsThe imaging features of benign and malignant SPN overlap.The blur sign is the independent risk factor of malignant SPN, and the straight edge is the independent protective factor of benign nodules. -
Key words:
- solitary pulmonary nodule /
- medical imaging /
- logistic regression analysis
-
表 1 影响SPN良恶性的单因素分析
因素 SPN χ2 P 良性 恶性 性别 男 15(55.56) 12(44.44) 5.59 < 0.05 女 3(18.75) 13(81.25) 分叶征 有 4(21.05) 15(78.95) 6.06 < 0.05 无 14(58.33) 10(41.67) 毛刺征 有 4(19.39) 19(82.61) 12.16 < 0.01 无 14(70.00) 6(30.00) 平直边 有 8(72.73) 3(27.27) 4.21 < 0.05 无 10(31.25) 22(68.75) 血管集束征 有 3(17.65) 14(82.35) 6.77 < 0.01 无 15(57.69) 11(42.31) 支气管征 有 2(15.38) 11(84.62) 5.37 < 0.05 无 16(53.33) 14(46.67) 空泡征 有 2(22.22) 7(77.78) 0.93 >0.05 无 16(47.06) 18(52.94) 胸膜凹陷 有 5(25.00) 15(75.00) 4.37 < 0.05 无 13(56.52) 10(43.48) 结节成分 磨玻璃 2(50.00) 2(50.00) 部分磨玻璃 2(18.18) 9(81.82) 3.67 >0.05 实性 14(50.00) 14(50.00) 年龄(x±s)/岁 57.83±14.80 64.12±10.18 1.65* >0.05 最大径(x±s)/cm 1.67±0.52 1.99±0.78 1.52* >0.05 长短径比值(x±s) 1.33±0.24 1.24±0.27 1.13* >0.05 *示t值;()中为百分率/%  下载: 导出CSV
下载: 导出CSV
表 2 SPN良恶性的多因素logistic回归分析
自变量 β Waldχ2 P 0R OR 95% CI 性别 -1.500 1.712 >0.05 4.481 0.474~42.373 分叶 0.287 0.052 >0.05 0.751 0.064~8.868 毛刺 2.242 4.022 < 0.05 0.106 0.012~0.950 胸膜凹陷 1.271 1.562 >0.05 0.281 0.038~2.060 气管征 1.887 2.318 >0.05 0.152 0.013~1.720 血管集束征 0.407 0.106 >0.05 0.665 0.057~7.768 平直边 -2.425 3.943 < 0.05 11.307 1.032~123.888
下载: 导出CSV
-
[1] SULLIVAN DR, GOLDEN SE, GANZINI L, et al.'I still don't know diddly':a longitudinal qualitative study of patients knowledge and distress while undergoing evaluation of incidental pulmonary nodules[J]. NPL Prim Care Respir Med, 2015, 25:15028. doi: 10.1038/npjpcrm.2015.28 [2] 李梦琦, 韩融城, 宋文静, 等.CT三维容积分析在实性肺结节恶性风险度评估中的价值[J].中国肺癌杂志, 2016, 19(5):279. [3] 迟淑萍.CT图像纹理分析在鉴别良恶性肺结节中的价值[J].实用放射学杂志, 2016, 32(11):1789. doi: 10.3969/j.issn.1002-1671.2016.11.036 [4] OST D, FEIN A.Management strategies for the solitary pulmonary nodule[J]. Curr Opin Pulm Med, 2004, 10:272. doi: 10.1097/01.mcp.0000130322.11513.c8 [5] GOULD MK, ANANTH L, BARNETT PG, et al.A clinical model to estimate the pretest probability of lung cancer in patients with solitary pulmonary nodules[J]. Chest, 2007, 131:383. doi: 10.1378/chest.06-1261 [6] HOREWEG N, VAN ROSMALEN J, HEUVELMANS MA, et al.Lung cancer probability in patients with CT-detected pulmonary nodules:a prespecified analysis of data from the NELSON trial of low-dose CT screening[J]. Lancet Oncol, 2014, 15(12):1332. doi: 10.1016/S1470-2045(14)70389-4 [7] 陈康, 努尔兰·阿汗, 马金山.孤立性肺结节的危险因素分析[J/CD].中华临床医师杂志(电子版), 2014, (14): 2602. [8] 王越, 宋龙霞, 黄艳, 等.孤立性肺结节55例的影像学特征分析[J].中国基层医药, 2018, 25(3):352. doi: 10.3760/cma.j.issn.1008-6706.2018.03.022 [9] 张著学, 彭学勤, 薛英波, 等.肺腺癌中表皮生长因子受体基因突变与临床病理因素的关系[J].实用医学杂志, 2015, (13):2155. doi: 10.3969/j.issn.1006-5725.2015.13.027 [10] 齐晨晖, 慕建成, 胡瑞霞.孤立性肺结节64排螺旋CT征象良恶性鉴别诊断的Logistic回归分析[J].影像诊断与介入放射学, 2013(1):18. [11] BAYANATI H, E THORNHILL R, SOUZA C A, et al.Quantitative CT texture and shape analysis:can it differentiate benign and malignant mediastinal lymph nodes in patients with primary lung cancer[J]. Eur Radiol, 2015, 25(2):480. doi: 10.1007/s00330-014-3420-6 [12] NG F, GANESHAN B, KOZARSKI R, et al. Assessment of primary colorectal cancer heterogeneity by using whole-tumor texture analysis:contrast-enhanced CT texture as a biomarker of 5 year survival[J]. Radiology, 2013, 266(1):177. doi: 10.1148/radiol.12120254 [13] 叶峰, 陈城, 张永奎.直径≤ 1 cm肺结节CT定性诊断的可行性分析[J].实用放射学杂志, 2016, 32(5):699. doi: 10.3969/j.issn.1002-1671.2016.05.010 [14] 丁玲, 张伟华, 马靖, 等.PET/CT对981例肺结节的良恶性诊断价值[J].癌症进展, 2017, 15(3):277. -

 点击查看大图
点击查看大图

图(2)表(2)
计量
- 文章访问数: 4096
- HTML全文浏览量: 2091
- PDF下载量: 12
- 被引次数: 0
