

-
化学治疗(化疗)是中晚期肺癌病人较为常见的治疗方法,但化疗药物刺激性强,不良反应多,对机体血管损伤性大,近10年来,护理同仁已经实行了化疗药物钢针零容忍,但静脉留置针在化疗药物输注时仍无法满足病人需求[1],PICC虽应用广泛,但PICC留置期间导管相关感染、堵管及血栓等并发症也不容忽视。植入式静脉输液港是完全植入皮下的静脉输液装置,具有舒适美观、保留时间长等优点,但在输液港维护期间仍可能发生静脉血栓栓塞症(venous thromboembolism, VTE), 对病人治疗、预后及生命产生不利影响,严重者需拔除输液港,容易继发多种静脉并发症。国内外对输液港导致的静脉血栓的发生及其危险因素报道较少[2]。本研究对158例使用输液港的肺癌化疗病人血栓发生原因进行调研,对其影响因素进行分析并提出护理对策,以期降低输液港致静脉血栓发生率。现作报道。
-
选择2016年7月至2019年3月我院收治的肺癌化疗使用输液港病人158例。纳入标准:(1)经病理学诊断确诊为肺癌,年龄≥18岁;(2)接受同期化疗;(3)病人对本研究知情同意,自愿参与此次研究。排除标准:(1)存在严重精神障碍;(2)上腔静脉压迫或阻塞综合征;(3)存在血液系统疾病史;(4)血小板计数≤20×109/L或≥300×109/L;(5)严重心、肺、肾功能不全。本研究所选肺癌标准化疗方案为TP(多西他赛联用顺铂),PP(培美曲塞联用顺铂),GP(吉西他滨联用顺铂),EP(依托泊苷联用顺铂)四种,化疗21天为1个周期。158例病人中,男96例,女62例;年龄45~75岁;肿瘤分类:非小细胞肺癌91例,小细胞肺癌67例;输液港植入部位:58例经锁骨下静脉植入,74例经颈内静脉植入,26例经贵要静脉植入(手臂港)。置管时间7~224 d。本研究已得到蚌埠医学院第一附属医院伦理审查委员会批准(年度审查编号为2020KY029)。
-
手臂港采用4.5F、胸壁港采用7F舒贝康植入式静脉输液港进行穿刺。超声引导下穿刺成功,送入导管,建皮下隧道,置入港体的皮下组织厚度以1 cm左右为宜[3]。术后拍胸片定位,导管尖端的最佳位置是上腔静脉和右心房交界处。
-
依据深静脉血栓诊断标准进行观察。(1)症状血栓:参照2017深静脉血栓形成的诊断和治疗指南(第3版)[4],观察病人穿刺侧部位出现疼痛、肿胀、伴上臂肩部锁骨上等部位的浅静脉扩张,静脉彩超可见实质性低回声团块血管管径扩张,确定血栓部位和范围。(2)无症状血栓:置管侧肢体或胸壁无明显不适主诉,静脉彩超显示:管腔内血流信号减少或消失;乏性反应消失或减弱;挤压远端肢体血流增强消失或减弱[5]。
-
自输液港植入后当天直至出院,护士全程进行血栓观察,如病人出现不适,例如呼吸费力、穿刺部位疼痛、红肿等症状,推注液体有阻力感,立即给予彩超检查,以精准判断病人是否发生输液港相关血栓。再次住院病人依旧按照输液港相关血栓观察标准进行,每次入院时给予上肢静脉彩超检查,符合上述标准即为输液港相关血栓,观察直至病人化疗周期结束。
-
采用χ2检验、秩和检验和非条件logistic回归。
-
158例肺癌化疗病人中发生输液港相关血栓31例(发生率19.6%),包括导管外壁血栓24例,导管内壁2例,复合血栓5例。其中,症状性血栓6例,主要表现为穿刺侧肢体疼痛,无症状血栓25例,排除出血倾向,予以低分子肝素钙5 000 U皮下注射,每天2次,尿激酶5 000 U/mL溶栓后,病人输液港继续使用;1例症状性血栓病人因治疗后症状无缓解而取出输液港。
-
根据是否发生输液港相关血栓将158例肺癌化疗病人分为无血栓组(n=127例)和血栓组(n=31例),2组病人单因素比较显示,留置时间、血液高凝状态、肿瘤分类和化疗方案对输液港血栓形成的影响具有统计学意义(P < 0.05~P < 0.01)(见表 1)。
分组 n 男 女 年龄/岁 导管留置时间 植港部位 45~ 55~ 65~75 ≤6个月 >6个月 锁骨下静脉 颈内静脉 贵要静脉 无血栓组 127 80(63.0) 47(37.0) 17(13.4) 64(50.4) 46(36.2) 92(72.4) 35(27.6) 49(38.6) 58(45.7) 20(15.7) 血栓组 31 16(51.6) 15(48.4) 6(19.4) 14(45.2) 11(35.4) 21(67.7) 10(32.3) 9(29.0) 16(51.6) 6(19.4) χ2 — 1.35 0.75 6.75 1.00 P — >0.05 >0.05 < 0.05 >0.05 分组 n 高凝状态* 肿瘤分类 输液座材质 化疗方案 否 是 非小细胞肺癌 小细胞肺癌 钛金属 树脂 TP PP GP EP 无血栓组 127 75(59.1) 52(40.9) 67(52.8) 60(47.2) 80(63.0) 47(37.0) 42(33.1) 30(23.6) 39(30.7) 16(12.6) 血栓组 31 8(25.8) 23(74.2) 24(77.4) 7(22.6) 21(67.7) 10(32.3) 13(41.9) 8(25.8) 7(22.6) 3(9.7) χ2 — 11.05 4.35 0.24 5.50 P — < 0.01 < 0.05 >0.05 < 0.05 注:*凝血四项有1项超出正常范围即为高凝状态 表 1 输液港相关血栓形成的单因素分析结果[n;构成比(%)]
-
以肺癌化疗输液港相关血栓形成为因变量(否=0;是=1),以留置时间、血液高凝状态、肿瘤分类、化疗方案为自变量(赋值见表 2),进行非条件logistic回归分析,设置α入=0.05, α出=0.10,结果显示,导管留置时间、血液高擬状态、肿瘤分类和化疗方案均与血栓形成的有关(P < 0.05~P < 0.01)(见表 3)。
自变量 赋值 导管留置时间 < 6个月=0;≥6个月=1 血液高凝状态 否=0;是=1 肿瘤分类 设置哑变量:小细胞肺癌为参考;非小细胞肺癌=肿瘤分类(1) 化疗方案 设置哑变量:EP为参考;PP=化疗方案(1);TP=化疗方案(2);GP=化疗方案(3) 表 2 自变量赋值
自变量 B SE Waldχ2 P OR(95%CI) 常量 1.243 1.192 0.75 >0.05 导管留置时间 -0.356 0.204 4.41 < 0.05 0.324(0.215~0.516) 血液高凝状态 -0.663 0.363 4.94 < 0.05 0.491(0.231~0.972) 肿瘤分类 非小细胞肺癌 1.690 0.534 8.63 < 0.05 23.954(15.423~39.800) 小细胞肺癌 1.691 0.523 12.32 < 0.01 0.147(0.019~1.001) 化疗方案 TP -3.925 0.747 18.66 < 0.01 0.025(0.003~0.106) PP 2.365 1.135 5.34 < 0.05 11.537(1.195~23.437) GP -2.544 0.632 7.59 < 0.05 0.079(0.029~0.224) 表 3 输液港相关血栓形成影响因素logistic回归分析(n=158)
-
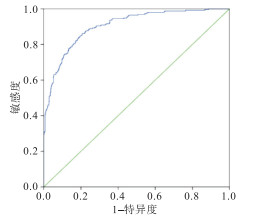
经Hosmer-Lemeshow检验可得,logistic回归模型拟合度良好(P>0.05,决定系数R2=0.584),对多因素logistic回归模型预测概率P进行ROC曲线验证,可得AUC为0.905(95%CI 0.884~0.927),敏感度为0.861,特异性为0.793,约登指数为0.654(见图 1)。

图 1 肺癌化疗病人输液港相关血栓形成影响因素logistic回归模型的ROC曲线
-
本研究输液港相关血栓发生率为19.6%,其中无症状血栓发生率为15.8%,症状性血栓发生率为3.8%,低于毛美芬等[6]报道的输液港血栓发生率。其他研究表明,输液港所致症状性血栓发生率为1.06%~11.4%[7-8],本研究所得结论基本吻合,说明本研究结果较为可靠。
-
本研究单因素分析结果显示,导管留置时间越长,血栓发生率越高,多因素分析结果显示,导管留置时间是血栓形成的促进因素。病人置管维护时间与住院时间重叠,故≤6个月病人每月能按时来院维护,所以血栓发生率较低。时间超过半年的病人化疗周期结束,病人依从性下降,部分病人未按时每月来医院冲管维护,或回当地医院肝素钠的封管液浓度达不到100 U/mL,导致留置时间超过半年的病人血栓发生率上升。
-
肿瘤细胞可通过生成癌促凝因子和诱导血小板改变来激活凝血过程[9],促使血液处于高凝状态。本研究单因素分析结果显示,非小细胞肺癌输液港血栓发生率为23.1%,高于小细胞肺癌输液港血栓发生率10.4%。凝血因子表达水平在非小细胞肺癌中的表达显著高于小细胞肺癌,因为此类病人血液黏稠度的增高、血流缓慢将减少因微血管挤压,而引起的肿瘤细胞机械性损伤,更加有利于癌栓的形成,更易造成血栓[10]。多因素分析结果显示,小细胞肺癌输液港血栓风险更低(OR=0.147),但P值为临界值,分析原因与样本量较小有关,可通过增加样本量做更深层次的观察。
-
本研究显示,TP及PP方案输液港血栓发生率高于GP方案者。其原因可能为,TP方案和PP方案化疗后纤维蛋白原含量升高更为显著,影响病人凝血状态,增加血栓发生概率。同时联用顺铂后血小板能够被其激活,血管性血友病因子水平也随之升高[11],继而导致血管内皮受损,抑制血管内皮生长因子的活性,损伤血管壁,从而导致血栓形成。
-
护士更应做好肺癌化疗病人VTE高危人群的筛查,及时采取预防措施。置管前监测病人凝血功能5项指标,排除高危病人出血倾向,预防性使用低分子肝素抗凝治疗。同时做好基本预防,如告知病人戒烟戒酒,控制血压血糖,做好踝泵运动、深呼吸、有效咳嗽的宣教。指导病人多吃蔬菜水果,饮水量化。手臂输液港病人应尽早做握拳、松拳练习,促进血液循环,预防VTE的发生。
置管后建立输液港出院随访登记制度,做好宣教工作,特别是留置时间>6个月的病人,可通过随访、建立微信群等方式督促病人按时维护,维护遇到的难题给予解答。提高病人依从性,预防长时间不维护导致血栓和堵管等并发症的发生。加强基层医院护理人员的标准化培训,由于输液港临床使用安全性受到护士的理论、技能、经验等因素的影响[12-13],大多数基层护理人员不了解输液港维护的标准化流程[14]。因此,要加强护士专业培训,掌握标准化维护流程,尤其是肝素封管液浓度的选择和无损伤针的使用,让护士能全面了解输液港的相关知识,以便正确处理。可通过专科基地培训、线上指导[15]等方式将输液港的相关知识普及到基层医院,以保证病人出院后在基层医院享受到输液港的正规维护。
肺癌化疗病人输液港相关血栓形成的影响因素分析及护理对策
Analysis of influencing factors and nursing strategies of infusion port-related thrombosis in chemotherapy patients with lung cancer
-
摘要:
目的对肺癌化疗病人输液港相关血栓形成的影响因素进行分析,并提出护理对策。 方法选择2016年7月至2019年3月收治的158例肺癌使用输液港病人为研究对象,回顾其临床资料,对输液港相关血栓形成的影响因素进行单因素和非条件多因素logistic回归分析,探讨输液港相关血栓形成的风险因素,并应用ROC曲线验证logistic回归的预测效果。 结果肺癌化疗病人输液港相关血栓发生31例(19.6%),单因素和多因素logistic回归分析显示,留置时间、血液高凝状态、肿瘤分类、化疗方案是输液港相关血栓形成的主要影响因素(P < 0.05~P < 0.01)。多因素logistic回归模型预测概率P进行ROC曲线验证,可得AUC为0.905(95%CI为0.884~0.927),敏感度为0.861,特异性为0.793,约登指数为0.654。 结论肺癌化疗病人输液港相关血栓与导管留置时间、血液高凝状态、肿瘤分类、化疗方案有关,护士应做好静脉血栓栓塞症高危人群的筛查和宣教,建立输液港出院随访登记制度,加强基层医院及社区护理人员的标准化培训,以降低输液港血栓发生率。 Abstract:ObjectiveTo analyze the influencing factors of infusion port-related thrombosis in chemotherapy patients with lung cancer, and to propose nursing strategies. MethodsA total of 158 patients with lung cancer from July 2016 to March 2019 were taken as the research objects.The influencing factors of the infusion port-related thrombosis were analyzed by univariate and unconditional multivariate logistic regression analysis.The risk factors of thrombosis related to infusion port were explored, and the predictive effect of logistic regression was verified using ROC curve. ResultsThirty-one cases(19.6%) of infusion port-related thrombosis occurred in lung cancer chemotherapy patients.Univariate and multivariate logistic regression analysis showed that indwelling time, blood hypercoagulability status, tumor classification, and chemotherapy regimens were the main factors of infusion port-related thrombosis(P < 0.05 to P < 0.01).The multivariate logistic regression model predicted the probability P for ROC curve verification, and the AUC was 0.905(95%CI: 0.884-0.927), the sensitivity was 0.861, the specificity was 0.793, and the Youden index was 0.654. ConclusionsInfusion port-related thrombosis in lung cancer chemotherapy patients is related to catheter indwelling time, blood hypercoagulability status, tumor classification, and chemotherapy regimens.Nurses should do a good job in screening and education of venous thromboembolism high-risk groups, establish a follow-up registration system at the infusion port, and strengthen the standardized training of nursing staff in primary hospitals and communities, so as to reduce the incidence of thrombosis in the infusion port. -
Key words:
- lung neoplasms /
- infusion port /
- thrombosis /
- influencing factors /
- nursing strategies
-
表 1 输液港相关血栓形成的单因素分析结果[n;构成比(%)]
分组 n 男 女 年龄/岁 导管留置时间 植港部位 45~ 55~ 65~75 ≤6个月 >6个月 锁骨下静脉 颈内静脉 贵要静脉 无血栓组 127 80(63.0) 47(37.0) 17(13.4) 64(50.4) 46(36.2) 92(72.4) 35(27.6) 49(38.6) 58(45.7) 20(15.7) 血栓组 31 16(51.6) 15(48.4) 6(19.4) 14(45.2) 11(35.4) 21(67.7) 10(32.3) 9(29.0) 16(51.6) 6(19.4) χ2 — 1.35 0.75 6.75 1.00 P — >0.05 >0.05 < 0.05 >0.05 分组 n 高凝状态* 肿瘤分类 输液座材质 化疗方案 否 是 非小细胞肺癌 小细胞肺癌 钛金属 树脂 TP PP GP EP 无血栓组 127 75(59.1) 52(40.9) 67(52.8) 60(47.2) 80(63.0) 47(37.0) 42(33.1) 30(23.6) 39(30.7) 16(12.6) 血栓组 31 8(25.8) 23(74.2) 24(77.4) 7(22.6) 21(67.7) 10(32.3) 13(41.9) 8(25.8) 7(22.6) 3(9.7) χ2 — 11.05 4.35 0.24 5.50 P — < 0.01 < 0.05 >0.05 < 0.05 注:*凝血四项有1项超出正常范围即为高凝状态  下载: 导出CSV
下载: 导出CSV
表 2 自变量赋值
自变量 赋值 导管留置时间 < 6个月=0;≥6个月=1 血液高凝状态 否=0;是=1 肿瘤分类 设置哑变量:小细胞肺癌为参考;非小细胞肺癌=肿瘤分类(1) 化疗方案 设置哑变量:EP为参考;PP=化疗方案(1);TP=化疗方案(2);GP=化疗方案(3)
下载: 导出CSV
表 3 输液港相关血栓形成影响因素logistic回归分析(n=158)
自变量 B SE Waldχ2 P OR(95%CI) 常量 1.243 1.192 0.75 >0.05 导管留置时间 -0.356 0.204 4.41 < 0.05 0.324(0.215~0.516) 血液高凝状态 -0.663 0.363 4.94 < 0.05 0.491(0.231~0.972) 肿瘤分类 非小细胞肺癌 1.690 0.534 8.63 < 0.05 23.954(15.423~39.800) 小细胞肺癌 1.691 0.523 12.32 < 0.01 0.147(0.019~1.001) 化疗方案 TP -3.925 0.747 18.66 < 0.01 0.025(0.003~0.106) PP 2.365 1.135 5.34 < 0.05 11.537(1.195~23.437) GP -2.544 0.632 7.59 < 0.05 0.079(0.029~0.224)
下载: 导出CSV
-
[1] 赵玉杰, 茅奇峰, 李情操, 等. 导管相关性血流感染的病原菌检测及影响因素分析[J]. 中国卫生检验杂志, 2017, 27(4): 470. [2] NARDUCCI F, JEANLAURENT M, BOULANGER L, et al. Totally implantable venous access port systems and risk factors for complications: a one-year prospective study in a cancer centre[J]. Eur J Surg Oncol, 2011, 37(10): 913. doi: 10.1016/j.ejso.2011.06.016 [3] 文砚, 芳万笑. 植入静脉输液港与PICC在乳腺癌化疗患者中的效果分析[J]. 护理实践与研究, 2018, 15(4): 132. [4] 中华医学会外科学分会血管外科分组. 深静脉血栓形成的诊断和治疗指南[J]. 中华普通外科学杂志, 2017, 32(9): 807. [5] 邢磊, 孔令泉, 厉红元, 等. 乳腺癌患者携带PICC化疗并发PICC相关性上肢深静脉血栓形成的诊治探讨[J]. 中国肿瘤临床, 2011, 38(1): 1223. [6] 毛美芬, 徐文亚, 高雪娟, 等. 乳腺癌化疗患者输液港相关血栓形成的影响因素[J]. 护理学杂志, 2019, 34(11): 33. [7] KANG J, CHEN W, SUN W, et al. Peripherally inserted central catheter-related complications in cancer patients: approspective study of over 50, 000 catheter days[J]. J Vasc Access, 2017, 18(2): 153. [8] ALMASI-SPERLING V, HIEBER S, LERMANN J, et al. Femoral placement of totally implantable venous access ports in patients with bilateral breast cancer[J]. Geburtshife Frauenheilkd, 2016, 76(1): 53. [9] CHANG YF, LO AC, TSAI CH, et al. Higher complication risk of totally implantable venous access port systems in patients with advanced cancer—a single institution retrospective analysis[J]. Palliat Med, 2013, 27(2): 185. [10] LI Z. SC17.02 lung cancer in china: challenges and perspectives[J]. J Thora Oncol, 2017, 12(1): S113. [11] 崔向丽, 万子睿, 侯珂露, 等. 增加肿瘤患者血栓风险的药物概述[J]. 中国药物警戒, 2017, 14(7): 430. [12] LEUNG TK, LEE CM, TAI CJ, et al. Aretrospective study on the long-term placement of peripherally inserted central catheters and the importance of nursing care and education[J]. Cancer Nurs, 2011, 34(1): 25. [13] 闻曲. PICC临床应用中的安全隐患及管理现状[J]. 护理学杂志, 2013, 28(14): 6. [14] 何晓容, 沈英. 社区PICC专业护士规范化培训的效果[J]. 护理学杂志, 2018, 33(13): 52. [15] 施如春, 智晓旭, 孟爱凤, 等. 居家肿瘤患者不同中心静脉导管堵管危险因素分析[J]. 护理学杂志, 2019, 34(11): 36. -

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 2353
- HTML全文浏览量: 1238
- PDF下载量: 15
- 被引次数: 0
