


-
凶险性前置胎盘(pernicious placenta previa,PPP)指既往有过剖宫产史,此次妊娠胎盘附着于原手术瘢痕部位,常伴有胎盘植入,分娩时容易引起难以控制的大出血[1]。近年来随着我国剖宫产率的居高不下以及人口生育政策的放开,同时伴随B超声及MRI诊断技术的提高,PPP发生率呈逐年上升趋势[2]。PPP伴胎盘植入病人手术过程中平均失血量3 000~5 000 mL,大于10 000 mL并非少见,是产科最具挑战性的疾病之一。MACHADO等[3]报道,PPP伴胎盘植入已取代子宫收缩乏力成为产科子宫切除的首要原因。如何减少PPP剖宫产术中失血,降低子宫切除率,改善母儿结局,一直是产科研究的难点和热点。本研究对PPP伴胎盘植入剖宫产术中应用髂内动脉球囊阻断术,进一步探讨该方法的临床效果和应用价值。现作报道。
-
收集2016年1月至2019年6月我院产科住院符合以下标准者纳入研究对象:经B超及MRI结合术中情况确诊为植入型凶险性前置胎盘(见图 1)。排除标准:(1)合并子宫畸形,双胎或者多胎,凝血功能异常等疾病;(2)孕妇因大出血行紧急剖宫产术者。共有86例符合标准纳入研究,术前充分告知手术风险和采取手术方式,依据知情选择原则进行分组,其中50例选择髂内动脉球囊阻断术(球囊组),36例拒绝行髂内动脉球囊阻断术(对照组),所有病人在剖宫产术前均签署手术知情同意书。
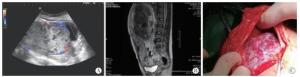
图 1 经彩超及MRI检查及术中情况确诊为凶险性前置胎盘伴胎盘植入
-
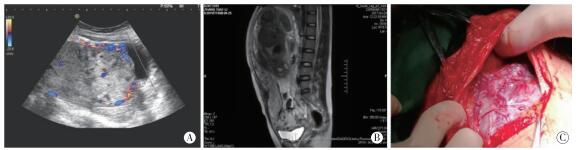
2组病人剖宫产术均由同一组高年资产科医师进行,球囊组介入手术在杂交手术室由同一组介入科医师进行。(1)球囊组:硬膜外麻醉成功后平卧于数字减影血管造影(DSA)台上,吸氧、心电监护,腹部及双侧腹股沟区消毒铺巾,行改良Seldinger技术分别穿刺左、右侧股动脉,导丝引导将6F球囊导管(美国强生公司生产,型号:4401004s)分别插入左右髂内动脉(见图 2)。胎儿娩出后,立即充盈球囊阻断双侧髂内动脉,宫缩剂应用及子宫按摩,待子宫收缩后人工剥离胎盘,胎盘剥离面进行局部缝扎,并采取宫腔填塞纱条等操作进行止血,缝合子宫,观察阴道流血情况,若有活动性出血需加行双侧子宫动脉栓塞术,必要时行子宫切除术。(2)对照组:根据剖宫产术中出血情况及胎盘植入情况,采用宫缩剂应用、子宫按摩、止血带控制出血、局部缝扎、双侧子宫动脉结扎术、宫腔纱条填塞术等多种方法进行止血,必要时行子宫切除术。

图 2 球囊组手术方法图示
-
介入手术过程中的放射量由DSA机进行记录。记录2组产妇手术时间、术中出血量及输血量、子宫切除率、术后住院时间及相关并发症的发生率。术中出血量统计按容积法和称重法。术后观察产妇双下肢感觉、运动和足背动脉搏动情况以及有无异常疼痛、发热等状况。
-
采用t检验和χ2检验。
-
2组的年龄、分娩孕周、孕产次、既往剖宫产次数、孕妇体质量指数(BMI)、距离末次剖宫产时间等差异均无统计学意义(P>0.05)(见表 1)。胎儿射线暴露:球囊组胎儿射线暴露剂量为(23.4±2.8)mGy。
分组 n 年龄/岁 孕周 孕次 产次 BMI/(kg/m2) 剖宫产
次数距末次剖宫产
时间/年球囊组 50 32.0±5.1 34.6±1.6 3.6±1.3 1.2±0.4 26.0±1.3 1.2±0.5 6.9±3.7 对照组 36 31.9±5.1 34.5±2.7 3.3±1.4 1.3±0.6 26.9±1.6 1.1±0.4 5.2±3.5 t — 0.07 0.22 1.02 0.28 1.83 1.02 1.98 P — >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 表 1 2组一般资料比较(x±s)
-
球囊组术中出血量及术中输血量均少于对照组(P < 0.05),2组手术时间、术后住院时间、子宫切除率及膀胱损伤发生率差异均无统计学意义(P>0.05)(见表 2)。球囊组有1例术后发生右下肢动脉血栓,2组均无输尿管及肠管损伤。
分组 n 术中出血量/mL 输红细胞量/U 手术时间/min 术后住院时间/d 子宫切除 膀胱损伤 血栓形成 球囊组 50 1 585.3±769.9 4.5±3.8 139.7±50.3 7.9±3.1 20(40.00) 6(12.00) 1(2.00) 对照组 36 2 044.1±1 362.9 6.8±4.9 143.8±45.4 7.5±2.9 16(44.44) 4(11.11) 0(0.00) t — 2.15 2.44 0.39 0.58 0.17* 0.02* 0.73* P — < 0.05 < 0.05 >0.05 >0.05 >0.05 >0.05 >0.05 *示χ2值 表 2 2组手术情况比较[n; 百分率(%); x±s]
-
PPP是剖宫产术后再次妊娠的严重并发症,分为植入型和非植入型。正常妊娠发生胎盘植入的风险为0.04%,而前置胎盘并发胎盘植入的发生率则高达10.00%[4]。植入型PPP易导致严重的产科大出血,必要时需切除子宫以挽救产妇生命。有学者认为,植入型PPP最佳处理孕周是34~35周,择期剖宫产同时主动行子宫切除术[5]。
介入技术已在产科广泛应用,因子宫的血供主要来自髂内动脉,术前应用髂内动脉球囊阻断术可阻断大部分的子宫血流,降低其动脉压,有利于手术创面的止血和凝血[6];理论上,栓塞或结扎双侧髂内动脉,能有效阻断子宫血流,但因胎儿影响,胎儿娩出前无法预防性栓塞或结扎,一旦胎儿娩出结扎双侧髂内动脉耗时且增加手术操作难度。而双侧髂内动脉球囊阻断术因其独特的优势临时阻断血供,为植入型凶险性前置胎盘带来曙光。在DSA的引导下此技术将球囊预置入髂内动脉,待胎儿娩出后充盈球囊,阻断血供,达到暂时性止血的目的。BROEKMAN等[7]研究发现,预置髂内动脉球囊阻断平均出血量800 mL,低于对照组1 000 mL;TAN等[8]研究也表明预置髂内动脉球囊可以降低胎盘植入的出血量;凶险性前置胎盘剖宫产术中应用髂内球囊封堵术,术中出血量约500~2 300 mL[9-10]。
髂内动脉球囊阻断需注意(1)控制放射剂量:根据国际辐射及防护委员会规定,射线量≤100 mGy[11]时,并不增加胎儿的致畸风险。本研究中,球囊阻断术组胎儿射线暴露剂量为(23.4±2.8)mGy,远低于上述标准。(2)球囊放置时间:因盆腔存在丰富的侧支循环,长时间阻断双侧髂内动脉并不会造成盆腔组织的缺血坏死[12],本研究中球囊组最长阻断时间达3 h,未出现并发症。相反,双侧髂总动脉阻断术及腹主动脉球囊阻断术在阻断盆腔血供的同时,也阻断下肢血供,时间过长可导致下肢缺血—再灌注损伤甚至缺血坏死,一次性阻断时间不宜超过30 min,需多次阻断间歇恢复血流。本研究中球囊组有1例术后并发右下肢动脉血栓,经血管外科手术取栓及配合术后抗凝治疗后血栓治愈。因此,术中及术后注意观察产妇双下肢皮肤颜色、皮温和足背动脉搏动等,一旦发现血栓形成,应尽快治疗。有文献报道1例产妇髂总动脉球囊阻断术后常规使用肝素钠预防血栓,仍发生腘动脉血栓,因此,认为动脉球囊阻断术是产妇血栓形成的危险因素[13]。(3)术中管理:髂内动脉球囊阻断术部分病例封堵效果不理想,不能有效控制术中出血。由于子宫同时接收来自腹主动脉、髂外动脉和股动脉吻合支的血流,文献报道在髂内动脉急性闭塞的情况下,吻合系统即刻发挥作用[14]。因此,预防性使用髂内动脉球囊阻断术,仍有继续出血的风险,应根据术中具体情况实施其他止血方法,必要时切除子宫。
本研究中,植入型PPP剖宫产术中应用髂内动脉球囊阻断术可减少术中出血量和术中输血量,但并不能有效降低子宫切除率,且可能增加介入手术带来的并发症,如下肢血栓等。如何合理使用髂内动脉球囊阻断术,需权衡利弊,术前充分医患沟通,告知风险,病人知情选择,同时做好风险防范措施。本研究不足在于样本量有限,且缺乏远期随访资料。
髂内动脉球囊阻断术在植入型凶险性前置胎盘剖宫产术中的应用疗效分析
Analysis of the application value of internal iliac artery balloon occlusion in cesarean section patients with pernicious placenta previa
-
摘要:
目的探讨髂内动脉球囊阻断术在植入型凶险性前置胎盘剖宫产术中的应用价值。 方法选择凶险性前置胎盘伴胎盘植入产妇86例临床资料,其中50例选择髂内动脉球囊阻断术(球囊组),36例仅行剖宫产术(对照组)。比较2组术中出血量、术中输血量、手术时间、术后住院时间、子宫切除率及相关并发症。 结果球囊组术中出血量(1 585.3±769.9)mL及术中输红细胞量(4.5±3.8)U,均小于对照组术中出血量(2 044.1±1 362.9)mL及术中输红细胞量(6.8±4.9)U(P < 0.05);球囊组子宫切除率40.00%,膀胱损伤率12.00%,与对照组子宫切除率44.44%、膀胱损伤率11.11%,差异均无统计学意义(P>0.05);球囊组有1例发生术后右下肢动脉血栓,对照组未发生。 结论植入型凶险性前置胎盘剖宫产术中采用髂内动脉球囊阻断术,可减少出血量及输血量,并不能有效降低子宫切除率,且有血栓形成风险。 Abstract:ObjectiveTo explore the application value of the internal iliac artery balloon occlusion in cesarean section patients with pernicious placenta previa (PPP). MethodsThe clinical data of 86 puerperas were retrospectively analyzed.Fifty cases treated with internal iliac artery balloon occlusion and 36 cases treated with cesarean section were divided into the balloon group and control group, respectively.The operative time, intraoperative blood loss, intraoperative blood transfusion, hysterectomy rate, postoperative hospital stay and related complications were compared between two groups. ResultsThe intraoperative blood loss and intraoperative red blood cell transfusion in balloon group[ (1 585.3±769.9)mL, (4.5±3.8)U] were less than those in control group[ (2 044.1±1 362.9)mL, (6.8±4.9)U], respectively (P < 0.05).The hysterectomy rate and bladder injury rate in balloon group and control group were (40.00%, 12.00%) and (44.44%, 11.11%), respectively, and the difference of which was not statistically significant (P>0.05).One case of right lower extremity artery thrombosis occurred in balloon group. ConclusionsThe internal iliac artery balloon occlusion in cesarean section patients with PPP can reduce the amount of intraoperative blood loss and blood transfusion, but not effectively reduce the rate of uterine resection, and has a risk of occuring thrombus. -
Key words:
- placenta previa /
- placental implantation /
- cesarean section /
- balloon occlusion /
- internal iliac artery
-
表 1 2组一般资料比较(x±s)
分组 n 年龄/岁 孕周 孕次 产次 BMI/(kg/m2) 剖宫产
次数距末次剖宫产
时间/年球囊组 50 32.0±5.1 34.6±1.6 3.6±1.3 1.2±0.4 26.0±1.3 1.2±0.5 6.9±3.7 对照组 36 31.9±5.1 34.5±2.7 3.3±1.4 1.3±0.6 26.9±1.6 1.1±0.4 5.2±3.5 t — 0.07 0.22 1.02 0.28 1.83 1.02 1.98 P — >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 2组手术情况比较[n; 百分率(%); x±s]
分组 n 术中出血量/mL 输红细胞量/U 手术时间/min 术后住院时间/d 子宫切除 膀胱损伤 血栓形成 球囊组 50 1 585.3±769.9 4.5±3.8 139.7±50.3 7.9±3.1 20(40.00) 6(12.00) 1(2.00) 对照组 36 2 044.1±1 362.9 6.8±4.9 143.8±45.4 7.5±2.9 16(44.44) 4(11.11) 0(0.00) t — 2.15 2.44 0.39 0.58 0.17* 0.02* 0.73* P — < 0.05 < 0.05 >0.05 >0.05 >0.05 >0.05 >0.05 *示χ2值
下载: 导出CSV
-
[1] CHEN Z, LI J, SHEN J, et al.Direct puncture embolization of the internal iliac artery during cesarean delivery for pernicious placenta previa coexisting with placenta accreta[J].Int J Gynaecol Obstet, 2016, 135(3):264. [2] KAPLANOGLU M, KARATEKE A, UN B, et al.Complications and outcomes of repeat cesarean section in adolescent women[J].Int J Clin Exp Med, 2014, 7(12):5621. [3] MACHADOLS.Emergency peripartum hysterectomy:Incidence, indications, risk factors and outcome[J].N Am J Med Sci, 2011, 3(8):358. [4] BALAYLA J, BONDARENKO HD.Placenta accreta and the risk of adverse maternal and neonatal outcomes[J].J Perinat Med, 2013, 41(2):141. [5] HULL AD, MOORE TR.Multiple repeat cesareans and the threat of placenta accreta:incidence, diagnosis, management[J].Clin Perinatol, 2011, 38(2):285. [6] GUPTA S, TALAULIKAR VS, ONWUDE J, et al.A pilot study of Foley's catheter balloon for prevention of intrauterine adhesions following breach of uterine cavity in complex myoma surgery[J].Arch Gynecol Obstet, 2013, 288(4):829. [7] BROEKMAN EA, VERSTEEG H, VOS LD, et al.Temporary balloon occlusion of the internal iliac arteries to prevent massive hemorrhage during cesarean delivery among patients with placenta previa[J].Int J Gynaecol Obstet, 2015, 128(2):118. [8] TAN YL, SUHARJONO H, LAU NL, et al.Prophylactic bilateral internal iliac artery balloon occlusion in the management of placenta accreta:A 36-month review[J].Med J Malaysia, 2016, 71(3):111. [9] SADASHIVAIAH J, WILSON R, THEIN A, et al.Role of prophylactic uterine artery balloon catheters in the management of women with suspected placenta accreta[J].Int J Obstet Anesth, 2011, 20(4):282. [10] YI KW, OH MJ, SEO TS, et al.Prophylactic hypogastric artery ballooning in a patient with complete placenta previa and increta[J].J Korean Med Sci, 2010, 25(4):651. [11] SAWADA A, MIYASHITA R, EDANAGA M, et al.Anesthetic management of caesarean section using common iliac artery balloon occlusion in patients with placenta previa[J].Masui, 2011, 60(12):1401. [12] DILAURO MD, DASON S, ATHREYA S.Prophylactic balloon occlusion of internal iliac arteries in women with placenta acereta:literature review and analysis[J].Clin Radiol, 2012, 67(6):515. [13] NICHOLSON PJ, O'CONNOR O, BUCKLEY J, et al.Prophylactic placement of internal iliac balloons in patients with abnormal placental implantation:Maternal and foetal outcomes[J].Cardiovasc Intervent Radiol, 2018, 41(10):1488. [14] LIU J, WANG Y, JIAO D, et al.Prophylactic occlusion balloonplacement in the abdominal aorta combined with uterine orovarian artery embolization for the prevention of cesareanhysterectomy due to placenta accreta:A retrospective study[J].Cardiovasc Interv Rad, 2019, 42(6):829. -

 点击查看大图
点击查看大图
图(2)表(2)
计量
- 文章访问数: 3971
- HTML全文浏览量: 1983
- PDF下载量: 5
- 被引次数: 0
