

 下载:
下载:
-
随着社会的进步,广大妇女对乳腺疾病的重视程度越来越高,早期乳腺癌发现率随之增高,手术作为乳腺癌治疗的重要手段之一,有着不可替代的作用。如何最大程度切除肿瘤,同时把手术后的并发症降低到最小程度,改善病人的生活质量,一直是乳腺外科界孜孜追求的目标。文献显示常规乳腺癌改良根治术行腋窝淋巴结清扫(ALND)后,2年内同侧上臂水肿的发生率最高达40%~60%[1],随着前哨淋巴结活检术的开展,使得一部分病人避免了ALND,同侧上臂淋巴水肿的发生率也随之下降,但是最高也能达到7%[2]。上臂水肿不仅影响美观,严重者甚至影响到日常生活,给病人精神和肉体带来不可弥补的创伤。如何找到有效的方法来进一步减少甚至杜绝此类并发症的发生。我们的团队在这方面已经做了很多工作,自2009年至今,术中开展腋窝反向淋巴作图(ARM)达500余例,在严格控制适应证的情况下,作图成功并保留ARM淋巴结的病人,2年随访出现严重的上肢水肿的发生率为0[3]。然而,目前对上臂淋巴回流与腋窝淋巴结之间关系的应用解剖基础研究甚少,为了给临床ARM提供解剖学上的理论依据,本实验对20具(40侧)经甲醛溶液固定的成年女性尸体标本的腋窝及上臂区域进行解剖,观察上臂淋巴回流与腋窝淋巴结之间的解剖学关系,为临床医生在手术时保护上臂淋巴回流网,有效减少ALND及前哨淋巴结活检(SLNB)术后上臂水肿提供解剖学依据。
-
选取20例(40侧)成人女性尸体标本,由蚌埠医学院解剖教研室提供,年龄(46±5.6)岁,死因均为非疾病自然死亡;亚甲蓝溶液2 mL×10支;常规手术解剖器械一套;手术丝线若干;索尼SDH-10数码相机。
-
实验前对尸体上臂及腋窝给予过氧化氢浸泡预处理,使淋巴导管扩张。常规解剖法解剖腋区及近侧上臂区。观察腋窝各区淋巴结位置及数目,主要淋巴管走行;观察上臂浅层淋巴管走行;结扎腋静脉近心入口端,远端静脉内加压注射亚甲蓝溶液,待蓝染后观察回流静脉的淋巴管及淋巴结。
-
外侧群淋巴结数目为(3±1.3)个,肩胛下群淋巴结数目为(4±1.8)个,胸肌群淋巴结数目为(4±1.1)个,中央群淋巴结数目为(5±1.3)个,尖群淋巴结数目为(2±1.3)个。外侧群与胸肌群、中央群有淋巴管相互交通,并汇向尖群淋巴结(见图 1)。

图 1 上臂回流淋巴管、淋巴结与腋静脉关系
-
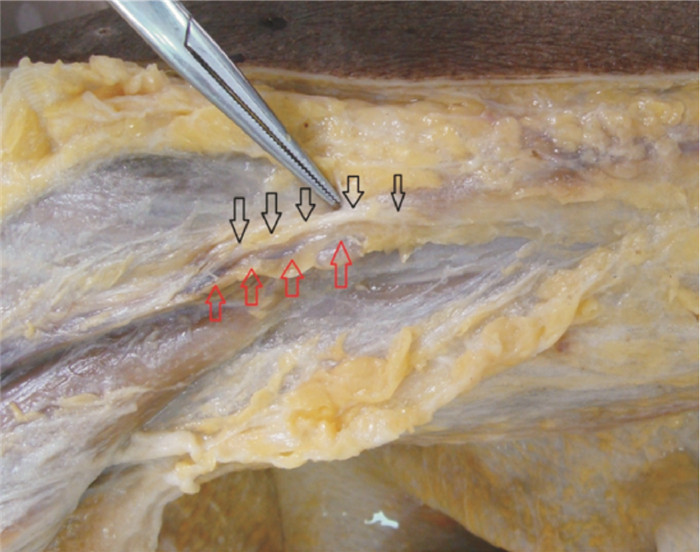
上臂浅层(内侧)皮下淋巴管在上臂区域有分支汇入贵要静脉12/40(见图 2),进入腋窝后主要汇入外侧群淋巴结25/40和中央群淋巴结13/40,有分支直接汇入腋静脉有20/40。
图 2 上臂淋巴导管注人到贵要静脉(黑色箭头所示为淋巴管,红色箭头所示为贵要静脉)
-
手术是乳腺癌的重要治疗手段,在病人罹患乳腺癌后,首先想到的就是外科治疗,外科手术可以有效地清除肿瘤病灶及淋巴结,在提高乳腺癌的治愈率及生存率上,有着非同一般的意义。但是术后一部分病人出现上臂的淋巴水肿,一直是难以克服的难题。从理论上分析,最主要的原因是术中损伤了上肢回流的淋巴管网。国外学者[4-5]对ALND术后并发严重上肢水肿的病人,行淋巴结移植及淋巴管吻合术后,发现可以减轻上臂的水肿程度,从而从另一面印证了上臂水肿的发生是因为术中对淋巴管的破坏造成。研究[6]发现,上臂的淋巴回流分为深、浅2组,2组互不干涉,几乎没有交通支,浅层淋巴回流的破坏导致了皮下淋巴回流不畅,极易出现水肿。所以,对上臂浅层回流淋巴管的保护,显得尤为重要。目前临床上开展的ARM技术,其过程是,术前30 min在上臂内侧皮下注射染料,通过活体淋巴液的流动,在术中显示出上臂回流的淋巴管及腋窝染色的淋巴结,并予以保留。通过这种方式保留下淋巴管及淋巴结的病人,无一例出现上臂水肿,为避免ALND及SLNB术后上臂水肿提供了极为有效的方法。但是,ARM的成功率只在70%左右,并且位置并不恒定[7-9]。况且在Ⅱb、Ⅲ期乳腺癌,强行保留此组淋巴结可能导致肿瘤残留,对其安全性提出疑问[10]。
本实验通过对成年女性尸体进行解剖,观察上臂浅层淋巴回流与腋窝淋巴结的关系。结果显示,上臂浅层的淋巴管,25例汇入外侧组淋巴结,与术中ARM常见位置相吻合。13例淋巴管汇入到了中央组淋巴结,这些淋巴结位置正好是文献报道的SLN检出率较高的区域,据此分析,SLNB术后上臂出现淋巴水肿的原因,是因为行SLNB术时损伤了上臂回流的淋巴管。国外文献[11-12]发现大约有10%的病人ARM位置与前哨淋巴结位置存在重叠。
本文我们还发现,上臂内侧皮下层淋巴管行走在肱二头肌表面结缔组织内,向腋窝方向回流,途中有回收淋巴结并有淋巴导管注入到头静脉(见图 1),比例达30.0%(12/40)。说明上臂浅层的淋巴管在汇入腋窝淋巴之前,即有部分头静脉已进入体循环。此部分病人术中在腋窝处上肢淋巴回流遭受破坏时,可能通过此循环代偿,减轻术后淋巴水肿的程度。
进一步发现,在完整地保护腋静脉鞘及喙锁筋膜完全打开之前,找出腋静脉胸廓入口,用7#慕丝线结扎腋静脉近心端,结扎处远端5 mL注射器7号针头加压注射亚甲蓝注射液,仔细操作,防止染料自针孔处外漏(见图 1)。5 min后发现,显露段腋血管完全蓝染,腋血管远端下方出现细小的网状蓝染淋巴管,并向上臂延伸,外侧组淋巴结有染色。蓝染淋巴结位置与文献描述的ARM淋巴结位置一致(见图 2)。根据观察到的情况,我们推测,上臂浅层淋巴管与腋窝淋巴结有交通支,尚存在细小的淋巴管交通支呈网状经腋鞘直接汇入腋静脉。由于上述两个因素的存在,使得一部分病人在行ALND术后,不会出现明显的上肢水肿现象。建议术中在不违背无瘤原则的情况下,尽可能减少对腋鞘的损伤,可最大程度降低上臂水肿发生率。由于交通支的存在,当某腋窝一组淋巴结被肿瘤侵犯,肿瘤细胞会沿着这些交通支蔓延到其他组,包括ARM淋巴结。故术前应充分评估腋窝淋巴结的状态,对N1期以上乳腺癌,在ALND同时行ARM时,一定要慎重考虑是否保留染色淋巴结。
通过此实验的初步观察证实,上肢的淋巴引流有其自身的引流通路,此通路与乳房的淋巴引流在腋窝处存在交通支。临床上,当腋窝淋巴结明确有淋巴结转移时,保留ARM存在肿瘤残留的风险。术中保护腋鞘的完整性,或可降低术后上肢淋巴水肿的严重程度。乳腺癌术中上肢ARM在技术上是可行性的,但安全性还存在很多不确定因素,需要进一步的临床研究。
上臂淋巴回流与腋窝淋巴结的应用解剖关系及意义
Applied anatomical relation between upper arm lymphatic drainage and axillary lymph node, and its significance
-
摘要:
目的为乳腺癌病人行前哨淋巴结活检(SLNB)及腋窝淋巴结清扫术(ALND)中,保留上臂淋巴回流,减轻上臂淋巴水肿提供解剖学依据。 方法对20具成人女性尸体的40侧腋区及近侧上臂区进行解剖,观察腋区各组淋巴结的数量、位置及近侧上臂浅表淋巴回流与腋区淋巴结、腋静脉三者的关系。 结果外侧群淋巴结数目为(3±1.3)个,肩胛下群淋巴结数目为(4±1.8)个,胸肌群淋巴结数目为(4±1.1)个,中央群淋巴结数目为(5±1.3)个,尖群淋巴结数目为(2±1.3)个,上臂浅层淋巴管有分支汇入贵要静脉12例(30.0%),至腋窝主要汇入外侧群淋巴结25例(62.5%),中央群淋巴结13例(32.5%);并有分支直接汇入液静脉20例(50.0%)。 结论ALND和SLNB术中保留反向淋巴作图淋巴管及淋巴结可有效保障上臂淋巴回流。 Abstract:ObjectiveTo provide the anatomical basis in preserving the upper limb lymphatic drainage to alleviate upper limb lymphedema during the sentinel lymph node biopsy (SLNB) and axillary lymph node (ALN) dissection (ALND) in breast cancer patients. MethodsThe axillary region and proximal upper arm region of 40 sides in female adult cadavers were dissected, and the number and location of lymph node in each axillary region were observed.The relationships among the superficial lymphatic reflux of proximal upper arm, axillary lymph node and axillary vein were analyzed. ResultsThe average number of lateral ALN, subscapularis ALN, pectoral ALN, central ALN and apical ALN was (3±1.3) (4±1.8) (4±1.1) (5±1.3) and (2±1.3), respectively.The superficial lymphatic drainage of upper limb draining into basilic vein in 12 cases (30.0%), lateral ALN in 25 cases (62.5%), central ALN in 13 cases (32.5%) and axillary vein in 20 cases (50.0%) were identified. ConclusionsPreservating the axillary reverse mapping lymphatic drainage and lymph nodes during ALND and SLNB can effectively protect the upper limb lymphatic drainage. -
[1] 王玲, 汪苗, 周丽华.乳腺癌腋窝淋巴结清扫术后上肢淋巴水肿相关症状研究[J/CD].中华乳腺病杂志(电子版), 2017, 11(2): 87. [2] HEERDT AS.Lymphatic mapping and sentinel lymph node biopsy for breast cancer[J].JAMA Oncol, 2018, 4(3):431. doi: 10.1001/jamaoncol.2017.4000 [3] 喻大军, 钱军, 李靖, 等.染料法腋窝反向淋巴作图 300例临床研究[J].中国肿瘤临床, 2013, 40(21):1296. doi: 10.3969/j.issn.1000-8179.20131127 [4] WEISS M, BAUMEISTER RG, FRICK A, et al.Lymphedema of the upper limb:evaluation of the functional outcome by dynamic imaging of lymph kinetics after autologous lymph vessel transplantation[J].Clin Nucl Med, 2015, 40(2):e117. [5] POUMELLEC MA, FOISSAC R, CEGARRA-ESCOLANO M, et al.Surgical treatment of secondary lymphedema of the upper limb by stepped microsurgical lymphaticovenous anastomoses[J].Breast Cancer Res Treat, 2017, 162(2):219. doi: 10.1007/s10549-017-4110-2 [6] GENTILESCHI S, SERVILLO M, ALBANESE R, et al.Lymphatic mapping of the upper limb with lymphedema before lymphatic supermicrosurgery by mirroring of the healthy limb[J].Microsurgery, 2017, 37(8):881. doi: 10.1002/micr.v37.8 [7] KUMAR KS, HEMANTH GN, PANJWANI PK, et al.Feasibility of axillary reverse mapping and clinicopathological features predicting ARM node metastasis in breast cancer-a pilot study[J].Indian J Surg Oncol, 2017, 8(2):119. doi: 10.1007/s13193-016-0578-1 [8] BEEK MA, GOBARDHAN PD, SCHOENMAECKERS EJ, et al.Axillary reverse mapping in axillary surgery for breast cancer:an update of the current status[J].Breast Cancer Res Treat, 2016, 158(3):421. doi: 10.1007/s10549-016-3920-y [9] HAN C, YANG B, ZUO WS, et al.The feasibility and oncological safety of axillary reverse mapping in patients with breast cancer:a systematic review and meta-analysis of prospective studies[J].PLoS One, 2016, 11(2):e0150285. doi: 10.1371/journal.pone.0150285 [10] NGUI NK, FRENCH J, KILBY CJ, et al.Axillary reverse mapping in patients with breast cancer:is it oncologically safe[J].J Surg Oncol, 2016, 113(7):726. doi: 10.1002/jso.v113.7 [11] TJALMA W, VERBELEN H, GEBRUERS N.The role of an ARM procedure in the prevention of breast cancer related lymphedema[J].Eur J Surg Oncol, 2016, 42(1):151. doi: 10.1016/j.ejso.2015.09.028 [12] NOGUCHI M, MIURA S, MORIOKA E, et al.Is axillary reverse mapping feasible in breast cancer patients?[J].Eur J Surg Oncol, 2015, 41(4):442. doi: 10.1016/j.ejso.2015.01.029 -

 点击查看大图
点击查看大图

图(2)
计量
- 文章访问数: 7666
- HTML全文浏览量: 4288
- PDF下载量: 12
- 被引次数: 0
