


-
心尖肥厚型心肌病(apical hypertrophic cardiomyopathy, AHCM)是肥厚型心肌病的一种特殊类型,有研究[1]显示,AHCM老年病人心房颤动、脑卒中、慢性心力衰竭等心血管事件的发生率及死亡率均明显增高[1]。早期心尖肥厚型心肌病(pre-apical hypertrophic cardiomyopathy, PAHCM)病人常因临床症状不明显或较轻,极易被漏诊。因此,提高PAHCM的诊断率对临床及早预防心血管事件具有一定意义[2]。本研究分析32例PAHCM病人超声心动图及声学造影资料,并与健康志愿者作比较,总结PAHCM的超声特征,旨在提高本病的诊断准确率。现作报道。
-
选取2016-2017年我院就诊疑似肥厚型心肌病的病人60例,入选标准:具有肥厚型心肌病家族史且心电图检查出现异常。所有病人均行超声心动图、心脏声学造影、磁共振成像(MRI)和标准12导联心动图检查。以MRI为金标准[3],共有32例病人确诊为PAHCM,作为PAHCM组。诊断标准:病变部位局限于左室乳头肌水平以下的心尖部,呈弥漫性或局部节段性心肌肥厚,舒张末期心尖部心肌厚≥11 mm且<15 mm,舒张末期心尖部心肌的最大厚度与左室后壁心肌厚度比值≥1.3[4],排除高血压、心脏瓣膜病变、运动员生理性等其他心源性或系统性原因引起的心肌肥厚[5-6]。同期选取32名健康志愿者作为正常对照组,入选标准:体检无心血管系统阳性体征,无冠心病、高血压、瓣膜病、先天性心脏病、心律失常、超声心动图、心电图和胸部X线片检查均未见异常。
-
采用Philips EPIQ 7C型超声诊断仪,S5-1超声探头,频率1~5 MHz,帧频55~90帧/秒。造影剂选用的是意大利Bracco公司生产的SonoVue,使用时先用5 mL 0.9%氯化钠注射液稀释,手工震荡20 s后变成乳白色的微泡混悬液。在肘部正中静脉处建立静脉通道,抽取2.5 mL混悬液,以0.9 mL/min的速度推注至静脉通道内,最后再用5 mL 0.9%氯化钠注射液以相同速度冲管。
-
常规连接心电图实时监测心率,嘱受检者左侧卧位,常规超声心动图检测并记录4个心动周期的胸骨旁左室长轴切面、二尖瓣水平、乳头肌水平及心尖短轴切面,心尖四腔、两腔及三腔切面。设置声学造影模式,将超声诊断仪的机械指数设置为0.08,心动周期设置为20,在静息状态下点击动态采图,分别记录下心尖四腔、三腔及两腔切面在“flash”闪烁前5个左右的心动周期及闪烁后15个左右的心动周期。所有图像均由专人录制,保证图像的质量及稳定性。
-
于声学造影条件下,待造影剂均匀充盈左室腔,心内膜界限显影清晰时,测量舒张末期左室心尖部心肌的最大厚度(AT)、舒张末期左室后壁心肌厚度(LVPWT)、计算得出舒张末期左室心尖部与后壁心肌厚度比值(AT/LVPWT)、Simpson′s法测得左室射血分数(LVEF)。于常规超声心动图条件下,测量左室心肌重量(LVM)、双平面面积长度法测量收缩末期左房容积(LAV)、四腔心切面测量舒张期二尖瓣血流频谱E峰与A峰的比值(E/A)。应用QLab10.0软件中的ROI插件对声学造影条件下的心尖四腔、两腔及三腔切面进行分析,通过函数公式对造影结果进行曲线拟合得出相应节段的时间-强度曲线,并获得该心肌节段心肌灌注指标:造影剂平台峰值强度(A)、曲线上升的斜率(β)、并计算A×β值。上述所有数值均测量3次,取平均值。
-
左室心肌节段按照美国超声心动图协会推荐的17节段分法。将PAHCM组分为2个亚组:P-AM组代表PAHCM病人心尖部肥厚的心肌节段,共92个节段;P-LVPW组代表PAHCM病人左室后壁心肌节段,共64个节段。正常对照组也分为2个亚组:N-AM组代表心尖部心肌节段,共160个;N-LVPW组代表左室后壁心肌节段,共64个。
-
采用t检验和χ2检验。
-
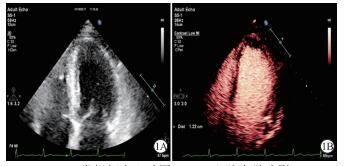
60例疑似肥厚型心肌病的病人经MRI检查,32例确诊为PAHCM。该60例受检者在单独使用常规超声心动图检查时,仅14例被诊断为PAHCM,以MRI为金标准,常规超声心动图的真阳性9例,假阳性5例,敏感性28.1%,特异性82.1%。该60例受检者在使用心脏声学造影检查时,32例被诊断出PAHCM,以MRI为金标准,假阳性为0,敏感性100%,特异性100%(见图 1)。PAHCM组心电图检查均出现为ST-T改变,主要表现为T波倒置、ST段水平型下移、左室高电压。2组在性别、年龄、身高和体质量方面差异均无统计学意义(P>0.05)(见表 1)。
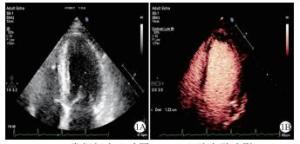
图 1 PAHCM病人常规超声心动图与心脏声学造影
分组 n 男 女 年龄/岁 身高/cm 体质量/kg 正常对照组 32 22 10 46.41±12.53 168.56±6.46 63.81±7.85 PAHCM组 32 21 11 48.25±11.47 168.77±6.33 65.62±8.15 t — 0.07* 0.61 0.13 0.91 P — >0.05 >0.05 >0.05 >0.05 *示χ2值 表 1 2组一般情况比较(x±s)
-
与正常对照组比较,PAHCM组的AT/LVPWT、LAV、LVM指标均增高(P<0.05),AT明显增高(P<0.01),E/A比值明显下降(P<0.01);2组LVPWT、LVEF差异无统计学意义(P>0.05)(见表 2)。
分组 AT/mm LVPWT/mm AT/LVPWT LAV/mL LVM/g LVEF/% E/A 正常对照组 8.24±1.21 9.03±0.76 0.95±1.04 41.25±8.57 116.35±24.51 68.45±4.67 1.23±0.52 PAHCM组 12.45±1.87 9.12±0.85 1.55±1.15 45.76±9.06 131.01±21.31 66.79±6.32 0.69±0.41 t 10.69 0.45 2.18 2.07 2.55 1.20 4.61 P <0.01 >0.05 <0.05 <0.05 <0.05 >0.05 <0.01 表 2 2组心脏构型及心功能指标的比较(ni=32;x±s)
-
与N-AM组比较,P-AM组A、β及A×β值均明显下降(P<0.01);与P-LVPW组比较,P-AM组A值下降(P<0.05),β及A×β值明显下降(P<0.01)(见图 2);与N-LVPW组比较,P-LVPW组的A、β及A×β值变化差异均无统计学意义(P>0.05)(见表 3)。
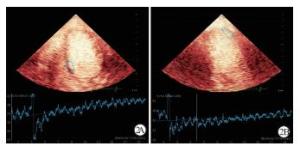
图 2 心肌声学造影曲线图
分组 n A/dB β/s A×β/(dB/s) P-AM组 92 6.86±1.74 0.81±0.43 5.89±2.64 N-AM组 160 7.50±1.65 1.18±0.49 8.17±3.11 t — 2.91 6.03 5.91 P — <0.01 <0.01 <0.01 P-LVPW组 64 7.48±1.59* 1.15±0.67** 7.93±2.69** N-LVPW组 64 7.51±1.71 1.17±0.36 8.15±2.92 t — 0.10 0.21 0.44 P — >0.05 >0.05 >0.05 与P-AM组比较*P<0.05,**P<0.01 表 3 2组心肌声学造影指标比较(x±s)
-
AHCM作为肥厚型心肌病的一种亚型,被认为是常染色体显性遗传性疾病,以男性多见[7]。PAHCM作为AHCM的早期阶段,随着时间推移,可能会发展为典型的AHCM。超声心动图因经济实惠、便捷、无创、无辐射等特点,被认为是目前筛查此类疾病高危人群的首选检查方法。本研究通过对32例PAHCM病人的超声心动图及声学造影资料进行分析,并与正常对照组比较,旨在总结PAHCM超声特征,提高诊断准确率。
为了避免因体表面积不同在心脏构型指标的比较中产生误差,本研究特意选择身高、体质量等一般情况指标与PAHCM组无明显差异的健康受检者作为正常对照组。PAHCM组常规超声心动图指标AT、AT/LVPWT、LVM、E/A、LAV与正常对照组相比差异有统计学意义。PAHCM病人心尖部心肌肥厚、心肌重量增加,这与病变心肌细胞肥大、心肌纤维粗大排列紊乱、结缔组织增生等因素有关。PAHCM组E/A比值较正常对照组下降,提示左室舒张功能减低。心肌对钙离子的敏感性增强,影响舒张期钙离子解离,阻碍肌动蛋白和肌球蛋白之间横桥分离,心肌松弛速率降低,心肌僵硬度增加,从而引起舒张功能障碍[8-9]。PAHCM组LAV增大,这是因为左室舒张功能减低,左室充盈压增高,左房容积受压力负荷的影响而增大[10-11]。
心脏声学造影包括心肌声学造影和心腔声学造影两部分。心肌声学造影技术是检测心肌血流灌注的新技术,通过公式y(t)=A[1-e-βt]+B拟合获得时间-强度曲线,得出平台峰值强度A、曲线上升的斜率β,A为局部心肌组织蓄积微气泡的数量,反映心肌血容量;β为局部心肌的造影剂充填速度,反映心肌血流速度;二者乘积A×β值,反映局部心肌血流量。P-AM组与P-LVPW组之间相比较,A、β及A×β值差异均有统计学意义;P-AM组与N-AM组相比较,A、β及A×β值差异均有统计学意义,这可能与肥厚心肌微循环受损有关[12]。有研究[13-14]表明,心肌微循环障碍可导致并发心肌缺血、心律失常、心衰,甚至心源性猝死,因此监测PAHCM微循环对临床评估PAHCM的发展及预后有着重要意义。本研究结果表明,A、β及A×β值在P-LVPW组与N-LVPW组之间比较差异均无统计学意义。由此提示,PAHCM病人可通对心尖肥厚心肌与自身左室后壁心肌声学造影指标的比较,及时发现病变心肌微循环灌注减低的情况,并定量评价,为以后随访复查提供参考依据。
PAHCM组中大部分病人无明显临床症状,仅少部分病人有胸闷、气短的表现,但心电图检查均出现ST-T改变,以MRI作为金标准,常规超声心动图对PAHCM检测的敏感性仅28.1%、特异性82.1%,而超声心动图结合声学造影检测的敏感性高达100%、特异性100%。常规超声心动图漏诊原因可能是由于胸部透声条件影响,近场回声较弱,心尖部二维图像显示欠清晰,部分超声医师诊断经验及仪器调节的经验不足,再加之临床症状及心电图表现缺乏特异性,所以造成漏诊、误诊。已有专家达成共识,当静息状态下不能满意获得常规超声心动图图像时,使用超声造影剂将明显提高图像质量、增强判断信心和诊断准确性[15]。由此提示,对于心电图出现异常的病人,尤其是有肥厚型心肌病家族史的病人,即使常规超声心动图未见明显异常,也有行心脏声学造影检查的必要性,为临床明确诊断提供依据。
综上所述,超声心动图结合声学造影,不仅能清晰显示心尖部解剖结构,提高PAHCM的诊断准确率,同时还可定量评价心肌微循环灌注情况,具有较高的临床应用价值,值得推广。
超声心动图结合声学造影对早期心尖肥厚型心肌病的诊断
Value of echocardiography combined with ultrasound contrast in the diagnosis of pre-apical hypertrophic cardiomyopathy
-
摘要:
目的探讨超声心动图结合声学造影在早期心尖肥厚型心肌病(PAHCM)诊断中的应用。 方法选择磁共振成像确诊为PAHCM的病人32例,正常对照组为32名健康志愿者,对比2组间超声心动图及声学造影特征。 结果与正常对照组比较,PAHCM组左室心尖部与后壁心肌厚度比值、左室心肌重量、左房容积指标均增高(P < 0.05),左室心尖部心肌厚度明显增高(P < 0.01),E/A比值明显下降(P < 0.01);与正常对照组心尖部心肌比较,PAHCM组心尖肥厚心肌组(P-AM组)平台峰值强度(A)、曲线上升斜率(β)及A×β值均明显下降(P < 0.01);与PAHCM组左室后壁组(P-LVPW组)比较,P-AM组造影A值下降(P < 0.05~P < 0.01)、β值及A×β值明显下降(P < 0.01);与正常对照组的左室后壁比较,P-LVPW组的A、β及A×β值差异无统计学意义(P>0.05)。以磁共振诊断为金标准,常规超声心动图诊断PAHCM的敏感性和特异性为28.1%、82.1%,超声心动图结合声学造影的敏感性和特异性为100%、100%。 结论超声心动图结合声学造影在PAHCM的诊断中具有较高的临床应用价值。 Abstract:ObjectiveTo discuss the application value of echocardiography combined with ultrasound contrast in the diagnosis of pre-apical hypertrophy cardiomyopathy(PAHCM). MethodsThirty-two patients with PAHCM diagnosed by MRI and 32 healthy volunteers were divided into the PAHCM group and normal control group, respectively.The characteristics of echocardiography and ultrasound contrast were compared between two groups. ResultsCompared with normal control group, the ratio of the myocardial thickness of left ventricular apical to posterior wall, left ventricular mass and left atrial volume increased(P < 0.05), the left ventricular apical myocardial thickness increased significantly(P < 0.01), and the value of E/A decreased significantly in PAHCM group(P < 0.01).Compared with the posterior wall myocardium of left ventricle of PAHCM group(P-LVPW group), the level of peak strength of platform(A) decreased(P < 0.05 to P < 0.01), and the curve rise slope(β) and A×β decreased significantly in P-AM group(P < 0.01).The differences of the levels of A, β and A×β between P-LVPW group and posterior wall myocardium of left ventricle in normal control group were not statistically significant(P>0.05).Using the diagnosis of MRI as a golden standard, the sensitivity and specificity of conventional echocardiography in the diagnosis of PAHCM were 28.1% and 82.1%, respectively, and both the sensitivity and specificity of echocardiography combined with ultrasound contrast in the diagnosis of PAHCM were 100%. ConclusionsEchocardiography combined with ultrasound contrast has great clinical application value in the diagnosis of PAHCM. -
Key words:
- hypertrophic cardiomyopathy /
- echocardiography /
- contrast agent
-
表 1 2组一般情况比较(x±s)
分组 n 男 女 年龄/岁 身高/cm 体质量/kg 正常对照组 32 22 10 46.41±12.53 168.56±6.46 63.81±7.85 PAHCM组 32 21 11 48.25±11.47 168.77±6.33 65.62±8.15 t — 0.07* 0.61 0.13 0.91 P — >0.05 >0.05 >0.05 >0.05 *示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 2组心脏构型及心功能指标的比较(ni=32;x±s)
分组 AT/mm LVPWT/mm AT/LVPWT LAV/mL LVM/g LVEF/% E/A 正常对照组 8.24±1.21 9.03±0.76 0.95±1.04 41.25±8.57 116.35±24.51 68.45±4.67 1.23±0.52 PAHCM组 12.45±1.87 9.12±0.85 1.55±1.15 45.76±9.06 131.01±21.31 66.79±6.32 0.69±0.41 t 10.69 0.45 2.18 2.07 2.55 1.20 4.61 P <0.01 >0.05 <0.05 <0.05 <0.05 >0.05 <0.01
下载: 导出CSV
表 3 2组心肌声学造影指标比较(x±s)
分组 n A/dB β/s A×β/(dB/s) P-AM组 92 6.86±1.74 0.81±0.43 5.89±2.64 N-AM组 160 7.50±1.65 1.18±0.49 8.17±3.11 t — 2.91 6.03 5.91 P — <0.01 <0.01 <0.01 P-LVPW组 64 7.48±1.59* 1.15±0.67** 7.93±2.69** N-LVPW组 64 7.51±1.71 1.17±0.36 8.15±2.92 t — 0.10 0.21 0.44 P — >0.05 >0.05 >0.05 与P-AM组比较*P<0.05,**P<0.01
下载: 导出CSV
-
[1] CAI C, DUAN FJ, YANG YJ, et al.Comparison of the prevalence, clinical features, and long-term outcomes of midventricular hypertrophy vs apical phenotype in patients with hypertrophic cardiomyopathy[J].Can J Cardiol, 2014, 30(4):441. [2] LEE CH, LIU PY, LIN LJ, et al.Clinical features and outcome of patients with apical hypertrophic cardiomyopathy in Taiwan[J].Cardiology, 2006, 106(1):29. [3] 韦云青, 赵世华, 陆敏杰, 等.心尖肥厚型心肌病的MRI诊断[J].中华放射学杂志, 2007, 41(8):800. doi: 10.3760/j.issn:1005-1201.2007.08.005 [4] 王欣欣, 董云, 张宇辉, 等.LVO测定心尖肥厚型心肌病的左心室传播速度[J].中国超声医学杂志, 2014, 30(7):603. [5] HANNEMAN K, CREAN AM, WILLIAMS L, et al.Cardiac magnetic resonance imaging findings predict major adverse events in apical hypertrophic cardiomyopathy[J].J Thorac Imaging, 2014, 29(6):331. doi: 10.1097/RTI.0000000000000115 [6] MASRUR S, MEMON S, CHHABRA L, et al.SPECT myocardial perfusion imaging in the diagnosis of apical hypertrophic cardiomyopathy[J].Tex Heart Inst J, 2016, 43(5):467. doi: 10.14503/THIJ-15-5485 [7] YAMAGUCHI H, ISHIMURA T, NISHIYAMA S, et al.Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy):ventriculographic and echocardiographic features in 30 patients[J].Am J Cardiol, 1979, 44(3):401. [8] GRUNER C, CHAN RH, CREAN A, et al.Significance of left ventricular apical-basal muscle bundle identified by cardiovascular magnetic resonance imaging in patients with hypertrophic cardiomyopathy[J].Eur Heart J, 2014, 35(39):2706. doi: 10.1093/eurheartj/ehu154 [9] SACCHERI MC, CIANCIULLI TF, MORITA LA, et al.Speckle tracking echocardiography to assess regional ventricular function in patients with apical hypertrophic cardiomyopathy[J].World J Cardiol, 2017, 9(4):363. doi: 10.4330/wjc.v9.i4.363 [10] 陈晓荣, 胡红杰, 钱玉娥, 等.心脏MR评价肥厚型心肌病左心房功能的应用研究[J].医学影像学杂志, 2014, 24(9):1482. [11] MINAMI Y, HAGIWARA N.Enlarged left atrium, atrial fibrillation and adverse outcome in hypertrophic cardiomyopathy:is there a difference between apical and non-apical phenotype[J].Heart, 2017, 103(19):1475. doi: 10.1136/heartjnl-2017-311501 [12] 朱黎, 赵新湘, 孙林.MR心肌首过灌注成像评估肥厚型心肌病心肌缺血[J].中国医学影像技术, 2018, 34(2):214. [13] MARON BJ.Contemporary insights and strategies or risk stratification and prevention of sudden death in hypertrophic cardiomyopathy[J].Circulation, 2010, 121(3):445. doi: 10.1161/CIRCULATIONAHA.109.878579 [14] RAJTAR-SALWA R, PETKOW-DIMITROW P, MISZALSKI-JAMKA T.Role of cardiac magnetic resonance in differentiating between acute coronary syndrome and apicalhypertrophic cardiomyopathy[J].Postepy Kardiol Interwencyjnej, 2016, 12(4):380. [15] 中华医学会超声医学分会超声心动图学组.中国心血管超声造影检查专家共识[J].中华超声影像学杂志, 2016, 25(4):277. doi: 10.3760/cma.j.issn.1004-4477.2016.04.001 -

 点击查看大图
点击查看大图
图(2)表(3)
计量
- 文章访问数: 4323
- HTML全文浏览量: 2199
- PDF下载量: 13
- 被引次数: 0
