


-
发育性髋关节发育不良(developmental dysplasia of the hip, DDH)是一种常见的骨骼肌肉系统疾病,病变常累及髋臼、股骨头、关节囊和髋关节周围的韧带和肌肉,是导致中青年继发性骨关节炎的最常见原因之一[1]。Bernese髋臼周围截骨术(Bernese periacetabular osteotomy, PAO)是目前临床上应用最为广泛的保髋手术之一[2-4]。虽然大多数DDH病人表现为髋臼前外上方的覆盖缺损,但有研究提示髋臼发育不良的部位及程度存在个体差异[5-6]。术前全面综合的评估髋臼覆盖缺损的部位和程度,术前设计个体化的手术方案是获得良好术后效果的前提条件[7-9]。目前临床上基于传统的二维影像资料无法对DDH病人进行术前精确评估是导致PAO术后效果不佳的主要原因之一[10-14]。因此,我们通过3D重建进行髋关节解剖形态学参数的测量,术前全面、综合地评估髋臼缺损的部位及程度,并通过计算机模拟手术设计个体化的手术方案,为实际PAO术提供参考,以提高手术精确性。现作报道。
-
本研究选取2012年6月至2019年2月因主诉髋关节酸痛不适超过半年以上、体格检查及影像学检查确诊为单侧DDH的病人10例(10髋),排除髋关节手术史(如切开复位)、合并有其他髋部畸形(如Legg-Calvé-Perthes病)、Crowe Ⅲ~Ⅳ型、Tonnis分期≥2的病人。其中男2例,女8例,年龄9~41岁。
-
病人仰卧于扫描台上,身体正中矢状面垂直于台面并与扫描台中线重合,髋、膝关节处于伸直位,双侧脚尖内旋10°~15°,扫描范围为髂嵴上缘至股骨近端1/3,相关数据以Dicom格式光盘刻录保存。
-
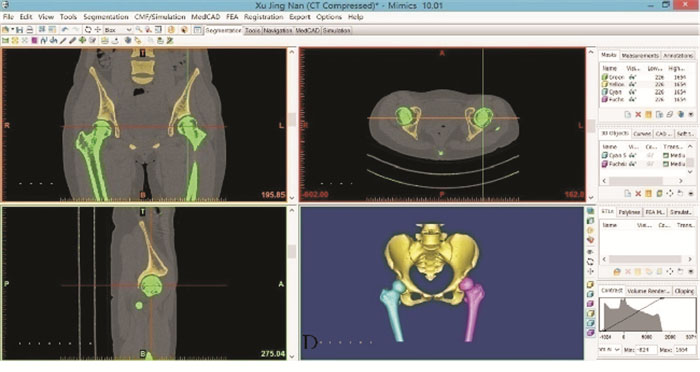
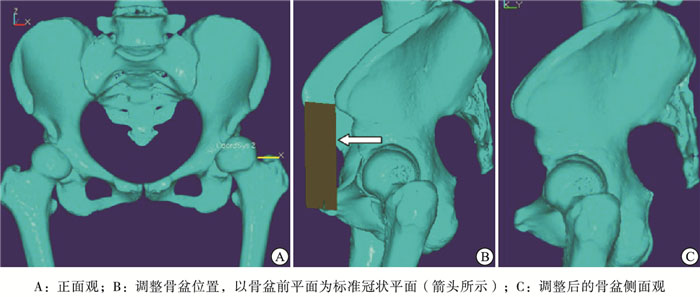
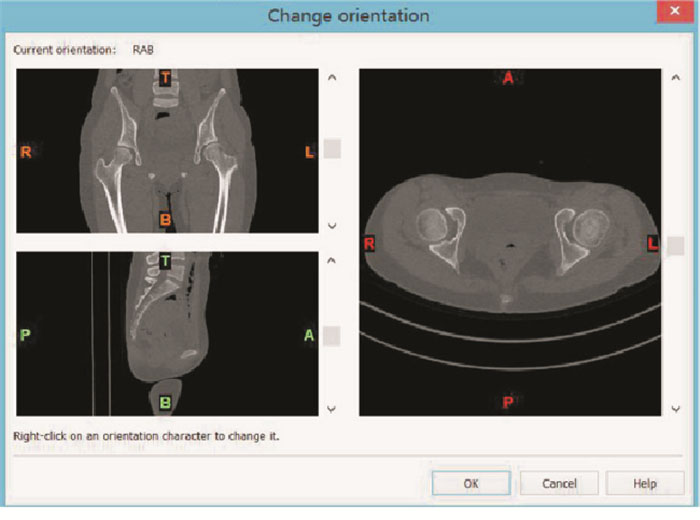
将Dicom格式的CT数据导入医学影像处理软件Mimics 10.01,定义好上、下、左、右方位后,自动生成冠状面、横断面、矢状面图像(见图 1)。利用Calculate 3D(计算3D模型)重建骨盆3D点云模型(见图 2)。将STL格式的DDH病人的骨盆3D模型数据导入逆向工程软件Imageware 13.2,生成髋关节的三维几何模型(见图 3),定义骨盆前平面,即将双侧髂前上棘及双侧耻骨联合中点所组成的平面定义为标准冠状平面,建立直角坐标系,调整摄片时由于病人体位倾斜所造成的骨盆倾斜及旋转。
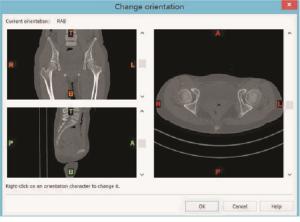
图 1 将Dicom格式的CT数据导入Mimics软件,定义上、下、左、右方位
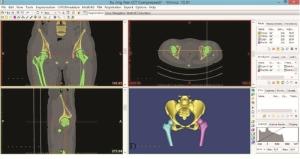
图 2 在Mimics中生成的重建骨盆3D点云模型
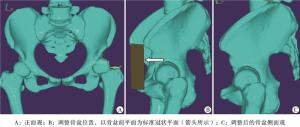
图 3 根据CT原始数据重建的髋关节三维几何模型
-
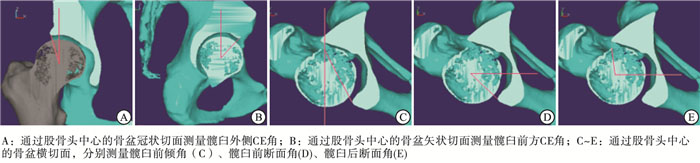
利用Imageware 13.2软件中的平面切割命令,对重建的三维图像进行切割。按照图 4中方法测量以下参数:(1)髋臼外侧中心边缘角(LCEA):三维重建图像中以通过股骨头中心的冠状切面,测量过股骨头中心的垂线与股骨头中心和髋臼外侧缘的连线的夹角;(2)髋臼前方中心边缘角(ACEA):三维重建图像中以通过股骨头中心的矢状切面,测量过股骨头中心的垂线与股骨头中心和髋臼前缘的连线的夹角;(3)髋臼前倾角(AAVA):三维重建图像中通过股骨头中心的横断切面,将髋臼前缘与髋臼后缘最外侧的两点连线称为和过股骨头中心的垂线的夹角即为髋臼的前倾角;(4)髋臼前断面角(AASA):三维重建图像中通过股骨头中心的横断切面,将髋臼前缘与股骨头中心连线和过股骨头中心的水平线的夹角即为髋臼前断面角;(5)髋臼后断面角(PASA):三维重建图像中通过股骨头中心的横断切面,将髋臼后缘与股骨头中心连线和过股骨头中心的水平线的夹角即为髋臼后断面角。

图 4 髋关节解剖形态学参数的测量方法
通过对每个DDH病人患侧与正常对照侧的髋关节解剖形态学参数进行对比,计算两者的差值(△LCEA、△ACEA、△AAVA、△AASA、△PASA),评估其髋臼开口方向(根据AAVA判断)、覆盖缺损的部位(根据LCEA、ACEA、AASA、PASA判断)及严重程度(根据△LCEA、△ACEA、△AAVA、△AASA、△PASA判断),设计个体化的手术方案,即髋臼截骨块旋转的方向及程度。
-
GANZ等[2]描述的Bernese髋臼周围截骨术包括对耻骨、坐骨和髂骨的系列截骨,将髋臼完全从骨盆上游离下来后重新旋转定位。根据其描述的方法,利用Imageware 13.2软件对重建的骨盆3D模型进行模拟手术。首先,通过软件定义相应的截骨平面来实现截骨(见图 5A)。截骨平面1定义为髂耻隆起内侧1 cm斜向身体中线的一个平面,实现对耻骨的截骨;截骨平面2定义为自髂前上、下棘之间朝向坐骨大切迹的一个平面,实现对髋臼上缘髂骨截骨;截骨平面3定义为从髋臼下缘坐骨体前方闭孔处朝向坐骨棘的一个平面,实现对髋臼下缘坐骨截骨;截骨平面4定义为距坐骨大切迹边缘约1 cm,连接截骨平面2、3并与标准冠状平面形成约25°夹角,实现对髋臼后缘骨盆后柱截骨。通过上述4个平面的模拟截骨操作可得到一个与实际PAO术中近似的髋臼截骨块(见图 5A)。随后再通过Imageware 13.2软件中“旋转”的命令对髋臼截骨块进行旋转操作(见图 5B)。旋转的方向及程度取决于△LCEA、△ACEA、△AAVA、△AASA、△PASA的大小(见图 5C、D)。完成模拟PAO术后再次按照上述的测量方法,测量模拟PAO术后髋臼的LCEA、ACEA、AAVA、AASA、PASA,避免出现继发性的髋股撞击症(FAI)及后方覆盖过度减少导致的关节不稳定。最后,记录每例DDH病人髋臼截骨块分别向外侧及前方旋转的度数,作为实际PAO术中参考。
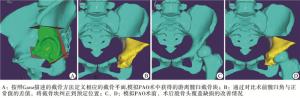
图 5 计算机模拟PAO术及手术前后效果比较
-
术后1周复查所有病人骨盆平片及CT,重建术后的髋关节3D模型并测量术后的LCEA、ACEA、AAVA、AASA、PASA。嘱所有病人术后前3个月每月复诊一次,以后每半年复诊一次,分别记录髋关节功能评分(Harris hip score,HHS)和反映髋关节疼痛严重程度的视觉模拟评分(visual analogue scale,VAS),同时检查髋关节活动度、复查骨盆平片。
-
采用t检验。
-
DDH病人患侧术前平均LCEA、ACEA、AASA、PASA均小于正常对照侧(P < 0.05),AAVA大于正常对照侧(P < 0.05)。按照术前设计,实际PAO术后病人的平均LCEA、ACEA、AAVA、AASA较术前改善(P < 0.05),但PASA与术前差异无统计学意义(P>0.05)。术后LCEA、ACEA、AAVA与正常对照侧差异无统计学意义(P>0.05)(见表 1)。
分组 LCEA/(°) ACEA/(°) AAVA/(°) AASA/(°) PASA/(°) 术前 对照侧 35.23±6.24 57.15±6.75 18.12±2.53 61.50±7.26 99.13±8.17 患侧 11.26±11.19 35.59±13.76 22.57±3.12 43.50±9.05 88.45±8.14 t 5.92 4.45 3.50 4.91 2.93 P < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 术后 对照侧 35.23±6.24 57.15±6.75 18.12±2.53 61.50±7.26 99.13±8.17 患侧 33.80±2.26** 55.28±2.19** 20.03±2.17** 51.39±7.63** 84.61±7.74 t 0.68 0.83 1.81 3.04 4.08 P >0.05 >0.05 >0.05 < 0.05 < 0.05 与术前患侧比较**P < < 0.05 表 1 DDH病人正常对照侧与患侧术前、术后髋关节的影像学测量(n=10;x±s)
-
所有入选病人术后均按时复诊,平均随访时间约10个月。术前、术后DDH病人的患侧HHS和VAS评分与对照侧差异均有统计学意义(P < 0.05),末次随访时患侧的HHS和VAS评分均较术前改善(P < 0.05)(见表 2)。
分组 HHS评分/分 VAS评分/分 术前 对照侧 99.35±1.24 0 患侧 66.86±5.22 3.25±0.61 t 19.15 16.85 P < 0.05 < 0.05 末次随访 对照侧 99.35±1.24 0 患侧 94.23±1.87** 1.04±0.81** t 7.22 4.06 P < 0.05 < 0.05 与术前患侧比较**P < 0.05 表 2 DDH病人的术前、术后临床功能评价(x±s)
-
PAO术是目前应用最为广泛的保髖手术之一,超过20年的临床随访证明,早期、精确实施的PAO术能获得良好的中长期效果[10-11, 15]。由于DDH病人最常出现髋臼前外上方的缺损,因此在PAO术中多将髋臼截骨块向前外侧方向旋转。然而通过3D测量发现DDH病人髋臼缺损的位置及程度存在较大的个体差异,例如,有的DDH病人髋臼外侧缺损较重而前方缺损较轻,在将髋臼截骨块向外侧旋转的同时其实前方覆盖缺损已经同时得到纠正。因为髋臼边缘波浪形的解剖形态,三维空间构象上髋臼截骨块在一个方向上的旋转必然伴随着其他方向上髋臼覆盖率的变化,所以如果再将髋臼截骨块向前旋转,就会人为的增加前方FAI及髋臼后方覆盖减少的风险,导致术后关节不稳定[5]。对于那些伴有髋臼后倾的DDH病人,在髋关节解剖形态上存在髂前下棘下移与髋臼前缘融合,造成空间上髋臼缘与股骨近端的相互靠近[16],PAO术中在纠正了外侧及前方覆盖的情况下还需将髋臼截骨块沿着身体纵轴适当内旋,以防止可能出现的术后FAI。对于髋臼缺损较重的某些DDH病人,由于髋臼周围的骨贮存量就严重不足,再加上髋臼边缘的“波浪形”外形,在将髋臼截骨块向前外侧方向旋转纠正前外侧覆盖缺损的同时,必然以后方覆盖的减少为代价,导致关节的不稳定;例如本研究中术后PASA较术前变小,就是因为在增加了前外侧覆盖的同时,后方覆盖减少。而且为了把最终的解剖形态学参数(LCEA、ACEA)恢复到所谓的正常解剖位置,就必须要将截骨块做大角度的旋转,此时关节周围的韧带、肌肉张力必将相应的增加,反而会导致关节内的压力增加[17]。因此,术前对髋关节解剖形态的全面综合评估并术前设计个体化的手术方案是获得良好术后效果的前提条件。目前,对于DDH病人髋关节发育状况的评估主要依赖于在X线片或二维CT影像资料上进行相关参数的测量,并不能直观、立体地提供病变部位的整体信息,而且扫描层面也容易受到病人摄片时体位的影响,无法全面真实地反映髋关节的三维立体形态[18]。
本研究通过对研究对象的原始CT数据进行三维建模,排除由于病人体位差异造成的测量误差, 分别测量髋臼的LCEA、ACEA评估髋臼的外侧、前上方覆盖情况, 测量髋臼的AAVA、AASA、PASA评估髋臼的开口方向、前方及后方覆盖情况, 然后与正常对照侧正常相应的参数进行对比,计算两者的差值,全面综合地评估髋臼缺损的位置及程度,设计个体化的手术方案,即髋臼截骨块旋转的方向及角度,并按照术前设计指导术中操作。结果显示,实际PAO术后DDH病人的LCEA、ACEA、AAVA较术前明显改善,即髋臼的前外侧覆盖较术前增加,基本达到正常范围,与对照侧无统计学差异。所有病人术后的HHS和VAS评分较术前都获得了明显的改善,但是仍未达到正常对照侧水平,分析原因可能与我们随访时间较短有关。因此,基于三维CT重建的计算机模拟技术在PAO术中具有很高的应用价值,值得推广。
基于三维CT重建的计算机模拟技术在DDH病人个体化手术方案设计中的应用
Application value of the computer simulation technology based on 3D-CT reconstruction in the design of individualized surgery for DDH patients
-
摘要:
目的探讨基于三维CT重建的计算机模拟手术在Bernese髋臼周围截骨术治疗发育性髋关节发育不良(DDH)的术前评估、术前手术设计以及术后评估中的指导作用。 方法应用Mimics和Imageware等医学影像处理软件对10例(10髋)DDH病人的CT原始数据进行3D重建、髋关节解剖形态学参数测量,术前评估髋臼开口方向、覆盖缺损的部位及程度,然后通过计算机模拟手术,设计个体化的手术方案,为实际手术提供参考。通过比较术前、术后的髋关节解剖形态学参数及临床功能评分评估效果。 结果DDH病人患侧术前髋臼外侧中心边缘角(LCEA)、髋臼前方中心边缘角(ACEA)、髋臼前断面角(AASA)、髋臼后断面角(PASA)均小于正常对照侧(P < 0.05),髋臼前倾角(AAVA)大于正常对照侧(P < 0.05)。按照术前设计,术后病人的LCEA、ACEA、AAVA、AASA均较术前改善(P < 0.05),PASA与术前差异无统计学意义(P>0.05)。术后LCEA、ACEA、AAVA与正常对照侧差异无统计学意义(P>0.05)。术前、术后DDH病人的患侧髋关节功能评分(HHS)和疼痛视觉模拟评分(VAS)与对照侧差异有统计学意义(P < 0.05),末次随访时患侧的HHS和VAS评分均较术前有明显改善(P < 0.05)。 结论基于三维CT重建的计算机模拟技术通过对DDH病人的髋关节解剖形态学参数进行测量,实现了术前对DDH病人的解剖结构发育畸形作出精确量化,并设计个体化的手术方案指导实际手术,使术后的影像学参数及临床功能评分获得明显的改善。 -
关键词:
- 先天性髋关节发育不良 /
- Bernese髋臼周围截骨术 /
- 三维CT重建 /
- 计算机模拟手术
Abstract:ObjectiveTo explore the role of virtual surgery based on 3D-CT reconstruction in the preoperative evaluation, surgical program and postoperative evaluation of Bernese periacetabular osteotomy(PAO) in the treatment of developmental dysplasia of the hip(DDH). MethodsThe 10 hips with DDH were reconstructed using Mimics and Imageware software, the anatomic morphological parameters of each hip were measured, and the direction of acetabular opening and location and extent of covering defect were evaluated before operation.The computer simulating operation and designing individualized surgical program provided the reference in actual operation.The results were evaluated by comparing preoperative and postoperative anatomical and morphological parameters of hip joint, and clinical function scores. ResultsBefore operation, the average values of LCEA, ACEA, AASA and PASA in affected side were less than those in normal side(P < 0.05), and the value of AAVA in affected side was bigger than that in normal side in DDH patients(P < 0.05).Compared with before operation, the mean values of LCEA, ACEA, AAVA, and AASA in PAO patients were significantly improved after PAO surgery(P < 0.05), but the PASA decreased, and the difference of which between before and after operation was not statistically significant(P>0.05).There was no statistical significance in the postoperative LCEA, ACEA and AAVA between affected side and normal side(P>0.05).The differences of the scores of HHS and VAS between two sides in DDH patients before and after surgery were statistically significant(P < 0.05).The scores of HHS and VAS in affected side at the last follow-up were significantly improved compared with those before operation(P < 0.05). ConclusionsThe computer simulation technology based on 3D CT reconstruction can measure the anatomical and morphological parameters of hip joint, accurately quantify the anatomic structural development deformity of DDH patients before surgery, design the individualized surgical plan to guide actual surgery, and significantly improve the imaging parameters and clinical function scores after surgery. -
表 1 DDH病人正常对照侧与患侧术前、术后髋关节的影像学测量(n=10;x±s)
分组 LCEA/(°) ACEA/(°) AAVA/(°) AASA/(°) PASA/(°) 术前 对照侧 35.23±6.24 57.15±6.75 18.12±2.53 61.50±7.26 99.13±8.17 患侧 11.26±11.19 35.59±13.76 22.57±3.12 43.50±9.05 88.45±8.14 t 5.92 4.45 3.50 4.91 2.93 P < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 术后 对照侧 35.23±6.24 57.15±6.75 18.12±2.53 61.50±7.26 99.13±8.17 患侧 33.80±2.26** 55.28±2.19** 20.03±2.17** 51.39±7.63** 84.61±7.74 t 0.68 0.83 1.81 3.04 4.08 P >0.05 >0.05 >0.05 < 0.05 < 0.05 与术前患侧比较**P < < 0.05  下载: 导出CSV
下载: 导出CSV
表 2 DDH病人的术前、术后临床功能评价(x±s)
分组 HHS评分/分 VAS评分/分 术前 对照侧 99.35±1.24 0 患侧 66.86±5.22 3.25±0.61 t 19.15 16.85 P < 0.05 < 0.05 末次随访 对照侧 99.35±1.24 0 患侧 94.23±1.87** 1.04±0.81** t 7.22 4.06 P < 0.05 < 0.05 与术前患侧比较**P < 0.05
下载: 导出CSV
-
[1] GANZ R, LEUNIG M.Morphological variations of residual hip dysplasia in the adult[J].Hip Int, 2007, 17(5):22. [2] GANZ R, KLAUE K, VINH TS, et al.A new periacetabular osteotomy for the treatment of hip dysplasias.Technique and preliminary results[J].Clin Orthop Relat Res, 1988(232):26. [3] 赵秀祥, 于建华.髋臼周围截骨术在治疗成人髋关节发育不良中的应用[J].中国矫形外科杂志, 2011, 19(7):578. [4] 宋永兴, 曾忠友, 陈晓东, 等.髋臼周围截骨术治疗中青年髋关节发育不良[J].中国矫形外科杂志, 2018, 26(10):878. [5] WANG XY, PENG JP, ZHU JF, et al.Application of three-dimensional computerised tomography reconstruction and image processing technology in individual operation design of developmental dysplasia of the hip patients[J].Int Orthop, 2016, 40(2):255. [6] WANG XY, PENG JP, LI D, et al.Does the optimal position of the acetabular fragment should be within the radiological normal range for all developmental dysplasia of the hip? A patient-specific finite element analysis[J].J Orthop Surg Res, 2016, 11(1):109. doi: 10.1186/s13018-016-0445-3 [7] 彭建平, 王旭义, 朱俊峰, 等.发育性髋关节发育不良患者股骨近端畸形特点的研究[J/CD].中华关节外科杂志(电子版), 2017, 11(3): 228. [8] INOUE D, KABATA T, MAEDA T, et al.Value of computed tomography-based three-dimensional surgical preoperative planning software in total hip arthroplasty with developmental dysplasia of the hip[J].J Orthop Sci, 2015, 20(2):340. [9] SUH DH, LEE DH, JEONG WK, et al.Virtual Bernese osteotomy using three-dimensional computed tomography in hip dysplasia[J].Arch Orthop Trauma Surg, 2012, 132(4):447. doi: 10.1007/s00402-011-1435-x [10] 程徽, 张洪, 罗殿中, 等.伯尔尼髋臼周围截骨术治疗髋关节发育不良的中长期疗效[J].中华骨科杂志, 2014, 34(12):1190. doi: 10.3760/cma.j.issn.0253-2352.2014.12.003 [11] 崔一民, 陈晓东, 朱俊峰, 等.髋臼周围截骨联合股骨转子间截骨术治疗复杂的髋关节发育不良的近期疗效[J].中华骨科杂志, 2015, 35(3):212. [12] ZHU J, CHEN X, CUI Y, et al.Mid-term results of Bernese periacetabular osteotomy for developmental dysplasia of hip in middle aged patients[J].Int Orthop, 2013, 37(4):589. doi: 10.1007/s00264-013-1790-z [13] 鞠盛涛, 贾堂宏, 宁斌.髋臼周围截骨术治疗成人髋关节发育不良的疗效[J].山东大学学报(医学版), 2014, 52(10):100. doi: 10.6040/j.issn.1671-7554.0.2014.208 [14] 张建立, 冯超, 尤海峰, 等.伯尔尼髋臼周围截骨术治疗青少年髋关节发育不良5~10年随访结果[J].中华外科杂志, 2014, 52(12):902. doi: 10.3760/cma.j.issn.0529-5815.2014.12.006 [15] STEPPACHER SD, TANNAST M, GANZ R, et al.Mean 20-year followup of Bernese periacetabular osteotomy[J].Clin Orthop Relat Res, 2008, 466(7):1633. doi: 10.1007/s11999-008-0242-3 [16] 黄瑛, 沈超, 朱俊峰, 等.髂前下棘与棘下撞击综合征[J/CD].中华关节外科杂志(电子版), 2017, 11(3): 280. [17] 张琳琳, 王旭义, 陈晓东.Bernese髋臼周围截骨术术前规划的有限元分析方法研究[J].生物医学工程学杂志, 2016, 33(3):455. [18] COBB J, LOGISHETTY K, DAVDA K, et al.Cams and pincer impingement are distinct, not mixed:the acetabular pathomorphology of femoroacetabular impingement[J].Clin Orthop Relat Res, 2010, 468(8):2143. doi: 10.1007/s11999-010-1347-z -

 点击查看大图
点击查看大图
图(5)表(2)
计量
- 文章访问数: 4693
- HTML全文浏览量: 2321
- PDF下载量: 14
- 被引次数: 0
