



-
近年来,随着人民生活水平的提高,健康体检的普及率大大增加,超声仪器的不断优化,甲状腺结节的检出率每年递增。甲状腺影像报告和数据系统(thyriod imaging reporting and data system,TI-RADS)为区分甲状腺结节良恶性提供了超声诊断依据,但因分级法不易量化控制,故选取其中与甲状腺结节相关性较高的方面对其进行计分,并与血清促甲状腺素(TSH)值联合,以期为提高甲状腺结节良恶性鉴别的准确率提供依据。
-
选取我院收治的因甲状腺结节而手术的病人109例,共159个结节,其中男59例,女50例,年龄18~89岁。所有病例术前均接受规范化甲状腺超声检查,并进行甲状腺功能检查,结节性质均经术后病理证实。
-
使用Philips ie33、Aloka α5、Philips iu22及迈瑞N6彩色多普勒超声诊断仪高频线阵探头,探头频率8~12 MHz。其中进行颈部131I放射治疗的病人需在治疗结束30 d后再次接受甲状腺超声检查,进行发射型计算机断层扫描仪检查的病人应当于检查结束后7 d,再次接受甲状腺超声检查。病人仰卧位时松弛颈项部并适当抬高,取得良好的颈前区及侧方颈部视野,对各区域进行多切面反复探查,探查范围包括甲状腺及其周边相邻区域,如甲状腺可探及结节,探查内容应包括:结节的数量、大小、形态、边界、内部回声、有无钙化、钙化大小及其分布、后方声影、血流及周围淋巴结等,并对结节边界、纵横比、内部回声、钙化及淋巴结进行计分,以推测结节的性质。血清TSH值在病人入院后于清晨空腹状态时抽取静脉血,3 000 r/min离心10 min,使用Siemens centaurXP全自动化学发光检测仪及配套试剂,化学发光免疫分析法进行检测。
-
超声细化计分法:根据TI-RADS及ATA指南对甲状腺结节的超声恶性风险表现[6]进行超声细化计分(见表 1)。病理诊断:对超声检出的甲状腺结节经手术或穿刺获取标本后,均送病理实验室检查分析,以病理石蜡切片经HE染色结果为准,对少数不典型病变结节可通过免疫组织化学法检查明确其性质。
项目 指标 计分/分 形态 规则 0 不规则 1 分叶,毛刺,浸润性 2 边界 清晰,壁光滑,包膜完整 0 模糊,壁欠清晰,无包膜 1 毛糙,甲状腺被膜外侵犯 2 纵横比 <1 0 =1 1 >1 2 回声 均匀无回声 0 等回声或高回声,可偏心 1 实性或囊实性低回声 2 钙化 未见 0 直径≥1 mm 1 直径<1 mm,边缘钙化中断 2 周围淋巴结 大小、结构、回声正常 0 长径≥2 cm,结构正常 1 结构失常,回声减低、不均 2 表 1 超声细化计分法标准
-
绘制受试者工作特征曲线(ROC),计算ROC曲线下面积(AUC),评价超声细化计分法、血清TSH值和两者联合区分甲状腺良恶性结节的诊断价值。
-
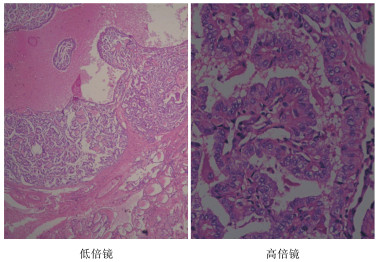
59例病人中,共检出甲状腺结节90个,病理诊断66个为良性结节,其中26个右结节性甲状腺肿,30个甲状腺瘤,7个慢性淋巴细胞性甲状腺肿及3个亚急性甲状腺炎;24个为恶性结节,其中20个乳头状癌(见图 1),4个微小癌。
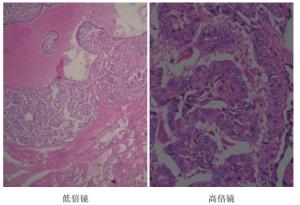
图 1 甲状腺乳头状癌HE染色
-
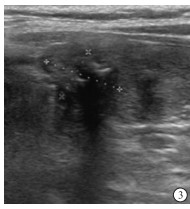
ROC分析显示(见图 2),超声细化计分法区分甲状腺良恶性结节的敏感度88.6%,特异度83.9%,AUC为0.779(95%CI:0.718~0.839),约登指数最大时,超声细化计分法最佳临界值为9分,≥9分判定结节为恶性(见图 3、4),<9分判定结节为良性;血清TSH值区分甲状腺良恶性结节的敏感度71.1%,特异度50.9%,AUC为0.703(95%CI:0.624~0.782),约登指数最大时最佳临界值2.31 mIU/L;超声细化计分法与血清TSH值联合区分甲状腺良恶性结节的敏感度90.1%,准确度84.5%,特异度84.3%。
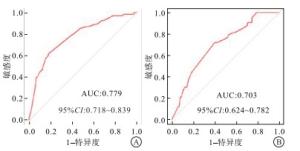
图 2 超声细化计分法和血清TSH值的ROC分析
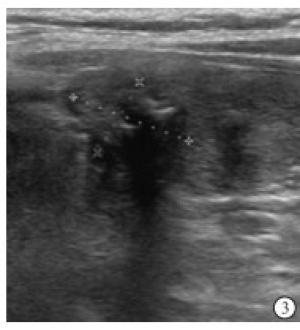
图 3 灰阶超声显示结节形态不规则,纵横比大于1

图 4 灰阶超声显水结节形态不规则, 内有多处钙化灶
-
甲状腺疾病的临床表现常常不具有特征性,而当甲状腺结节较小时自检不易察觉。近年来随着超声诊断技术的不断发展和高分辨率超声仪器的使用,甲状腺结节的检出率升高[1],而近年来甲状腺癌的增长速度居各种恶性肿瘤之首[2]。并且超声以其简便、无创、准确率较高的优势成为甲状腺疾病的首选检查,但仍具有一定误差,如何结合其他无创检查降低结节穿刺及手术率是我们所关注的。
在以往的常规超声诊断中,甲状腺疾病尤其是甲状腺结节一般根据超声图像所显示的结节形态学特征及血流特征进行良恶性鉴别。近年来随着甲状腺结节早期检出增多,结节各径线的超声测量值通常较小,血流分布受各方面影响往往不显著。且由于发生于甲状腺的结节往往伴随其他甲状腺疾病的背景,所以显示的甲状腺结节的超声图像常常较为复杂,同一声像图特征往往因为伴随其他声像图表现而有不同的诊断结果,而同一种甲状腺疾病也常常出现不同超声表现。甲状腺良恶性结节的二维声像图表现常常相似[3],特异性不高。PARK等[4]依据经统计学计算的恶性可能性建立了甲状腺影像报告和数据系统,将甲状腺结节根据超声表现进行分级,提出了TI-RADS分级建议。TI-RADS分级的建立对甲状腺结节的术前定性诊断、评估及制定手术方案有重要的意义。但在实际工作中TI-RADS分级系统中的项目繁多,且指标系统较为庞大,同一结节在不同项目中往往符合不同分级标准,在无侧重的情况下,较难对结节做出准确分级。因此,国内学者对甲状腺结节的超声危险因素进行分析,得出超声高危恶性风险表现为:以低回声为主的实性结节及囊实性结节中,同时具有以下一项或多项超声表现:(1)结节形态不规则,如小分叶、毛刺或呈浸润性;(2)结节纵横比>1;(3)结节内微小钙化(钙化直径<1 mm)多为簇状;(4)发生于结节边缘的钙化,其连续性中断,可见低回声向外突出于钙化外;(5)甲状腺包膜外侵犯[5]。
甲状腺癌的病灶特点是细胞大而重叠,分化程度低,间质少,乳头间质含量和纤维间质成分都非常少,加上大部分纤维间质发生玻璃样变致使对声的阻抗界面减少[6],超声图像上不会形成强烈反射界面,故肿瘤的透声性好,因此超声二维图像上会出现低回声的情况。甲状腺乳头状癌中最特异的超声表现是钙化,它的发生可能与肿瘤迅速生长,而局部血供不足,使局部纤维组织发生增生、退化、坏死的病理生理改变,进而引起肿瘤内的钙盐发生沉着有关。这些病理生理改变造成肿瘤声阻抗发生改变,导致声像图特征的多形性。笔者根据以上特征在甲状腺结节良恶性分辨上较主要的几个较敏感的方面如形态、边界、纵横比、结节内部回声、有无微钙化及周围淋巴结进行指标细化计分,并采用统计学方法绘制曲线,确定诊断临界值。
近年来,一些研究[7-9]证实甲状腺功能与甲状腺癌的发生相关,但结论不完全一致。TSH是腺垂体分泌的促进甲状腺的生长和机能的激素。分化型甲状腺癌细胞膜表面可表达TSH受体,血清中TSH的分泌长期过多会对cAMP的合成起促进作用,激活cAMP依赖性蛋白激酶信号转导系统。同时促进表皮生长因子介导的细胞增殖,减少转化生长因子B1产生,从而刺激甲状腺细胞生长,使甲状腺癌发生的危险性增加[10],由此可以推测,血清TSH很可能在甲状腺癌的发生发展过程中起促进作用。
但基于TI-RADS的超声细化计分法和血清TSH值两者单独对甲状腺结节良恶性作鉴别时,常常因个体化差异及病人其他伴随疾病等不确定因素的影响导致甄别的失败,二者联合后可最大程度减小不确定因素的影响,使鉴别敏感度、准确度、特异度均有所提高。因此,基于TI-RADS的超声细化计分法和血清TSH值联合对甲状腺结节良恶性的诊断符合率较两者独立诊断甲状腺结节良恶性有一定程度提高。
基于TI-RADS的超声细化计分法和血清TSH值联合鉴别甲状腺结节良恶性
Value of ultrasonic refined scoring method based on TI-RADS combined with serum TSH level in the differentiation diagnosis of benign and malignant thyroid nodules
-
摘要:
目的评价基于甲状腺影像报告和数据系统(TI-RADS)的超声细化计分法和血清促甲状腺素(TSH)值联合对甲状腺结节良恶性进行鉴别诊断的意义。 方法选取进行甲状腺结节手术的病人,基于TI-RADS分级系统,根据超声图像中结节边界、纵横比、回声、钙化及颈部淋巴结对甲状腺结节进行细化计分,联合病人入院血清TSH值,绘制受试者工作特征曲线(ROC),计算ROC曲线下面积(AUC),评价超声细化计分法、血清TSH值和两者联合区分甲状腺良恶性结节的诊断价值。 结果ROC分析显示,超声细化计分法区分甲状腺良恶性结节的敏感度88.6%,特异度83.9%,AUC为0.779(95%CI:0.718~0.839),约登指数最大时,超声细化计计分法最佳临界值为9分,≥ 9分判定结节为恶性, < 9分判定结节为良性;血清TSH值区分甲状腺良恶性结节的敏感度71.1%,特异度50.9%,AUC为0.703(95%CI:0.624~0.782),约登指数最大时取最佳临界值2.31 mIU/L;超声细化计分法与血清TSH值联合区分甲状腺良恶性结节的敏感度90.1%,准确度84.5%,特异度84.3%。 结论基于TI-RADS的超声细化计分法和血清TSH值联合鉴别甲状腺结节良恶性可使诊断符合率进一步提高,降低甲状腺结节的穿刺活检或手术率。 -
关键词:
- 甲状腺结节 /
- 超声细化计分法 /
- 甲状腺影像报告和数据系统 /
- 促甲状腺素
Abstract:ObjectiveTo assess the significance of ultrasonic refined scoring method based on thyroid imaging reporting and data system(TI-RADS) combined with serum thyroid stimulating hormone(TSH) level in the differentiation diagnosis of benign and malignant thyroid nodules. MethodsThe refined scoring of the boundary, aspect ratio, echo and calcification of thyroid nodules in ultrasonoscopy in patients treated with operation based on TI-RADS grading system combined with serum level of TSH on admission were analyzed to draw the receiver operating characteristic(ROC) curve and calculate the area under ROC curve(AUC).The value of serum level of TSH, ultrasonic refined scoring method and both combination in the differentiation diagnosis of benign and malignant thyroid nodules were evaluated. ResultsThe ROC analysis showed that the sensitivity and specificity of ultrasonic refined scoring method in differentiating benign and malignant thyroid nodules were 88.6% and 83.9%, respectively.The AUC was 0.779(95%CI:0.718 to 0.839).When the Youden's index was the largest, the optimal critical value of ultrasonic refined scoring method was 9 points, and the nodules with score ≥ 9 and < 9 points were malignant and benign, respectively.The sensitivity and specificity of serum level of TSH in distinguishing benign and malignant thyroid nodules were 71.1% and 50.9%, recpectively, and the AUC was 0.703(95%CI:0.624 to 0.782).When the Youden's index was the largest, the optimal critical value was 2.31 mIU/L, and the sensitivity, accuracy and specificity of ultrasonic refined scoring method combined with serum TSH value in distinguishing benign and malignant thyroid nodules were 90.1%, 84.5% and 84.3%, respectively. ConclusionsThe ultrasonic refined scoring method based on TI-RADS combined with serum level of TSH in the differentiation diagnosis of benign and malignant thyroid nodules can further improve the diagnostic coincidence rate, and reduce the rate of thyroid nodule biopsy or operation. -
表 1 超声细化计分法标准
项目 指标 计分/分 形态 规则 0 不规则 1 分叶,毛刺,浸润性 2 边界 清晰,壁光滑,包膜完整 0 模糊,壁欠清晰,无包膜 1 毛糙,甲状腺被膜外侵犯 2 纵横比 <1 0 =1 1 >1 2 回声 均匀无回声 0 等回声或高回声,可偏心 1 实性或囊实性低回声 2 钙化 未见 0 直径≥1 mm 1 直径<1 mm,边缘钙化中断 2 周围淋巴结 大小、结构、回声正常 0 长径≥2 cm,结构正常 1 结构失常,回声减低、不均 2  下载: 导出CSV
下载: 导出CSV
-
[1] 孙彤, 田晶, 李辰运, 等.相关实验室检查和超声特征在分化型甲状腺癌与结节性甲状腺肿鉴别诊断中的意义[J].中国超声医学杂志, 2017, 33(10):847. [2] 田文, 郗洪庆.甲状腺癌病人生存现状分析[J].中国实用外科杂志, 2016, 36(5):489. [3] ZHAN WW.Ultrasonic diagnosis progress of thyroid nodule[J/CD].Chin J Med Ultrasound (Electronic Edition), 2011, 8(6): 1170. [4] PARK JY, LEE HJ, JANG HW, et al.A proposal for a thyroid imaging reporting and data system for ultrasound features of thyroid carcinoma[J].Thyroid, 2009, 19(11):1258. [5] 刘如玉, 姜玉新, 杨筱, 等.甲状腺结节的影像报告与数据系统分级与2015年美国甲状腺学会推荐超声恶性风险分层的比较研究[J/CD].中华医学超声杂志(电子版), 2017, 14(4): 263. [6] 林建军, 邓伟, 罗永香, 等.桥本甲状腺炎合并微小癌的超声表现与病理对照分析[J].现代医药卫生, 2017, 33(16):2428. doi: 10.3969/j.issn.1009-5519.2017.16.007 [7] DUCCINI K, DE SOUZA MVL, DELFIM R, et al.High serum thyrotropin concentrations within the reference range:A predictor of malignancy in nodular thyroid disease[J].Med Princ Pract, 2018, 27(3):272. doi: 10.1159/000488196 [8] HUANG H, RUSIECKI J, ZHAO N, et al.Thyroid-stimulating hormone, thyroid hormones, and risk of papillary thyroid cancer:A nested case-control study[J].Cancer Epidemiol Biomarkers Prev, 2017, 26(8):1209. doi: 10.1158/1055-9965.EPI-16-0845 [9] BASER H, TOPALOGLU O, TAM AA, et al.Higher TSH can be used as an additional risk factor in prediction of malignancy in euthyroid thyroid nodules evaluated by cytology based on Bethesda system[J].Endocrine, 2016, 53(2):520. doi: 10.1007/s12020-016-0919-4 [10] 刘长路, 吴岩, 毕立夫.甲状腺癌流行现状及危险因素的研究进展[J].中国地方病学杂志, 2012, 31(2):234. doi: 10.3760/cma.j.issn.1000-4955.2012.02.035 -

 点击查看大图
点击查看大图
图(4)表(1)
计量
- 文章访问数: 3822
- HTML全文浏览量: 2029
- PDF下载量: 7
- 被引次数: 0
