







-
随着人口老龄化日趋加剧,骨质疏松性胸腰椎压缩性骨折(osteoporotic vertebral compression fracture,OVCF)发病率有逐年上升趋势,对于症状明显者,椎体成形术[经皮穿刺椎体成形术(PVP)或球囊扩张椎体后凸成形术(PKP)]因其创伤小、镇痛迅速、支持老年病人早期下床活动等优点[1-3],已成为治疗的首选方法。然而,PKP术后再骨折很常见,较大宗病例随访结果显示再骨折率达10.2%~15.6%[4-6]。而再骨折原因虽有许多研究但至今仍不十分清楚,本文结合我院临床病例对此进行探讨, 现作报道。
-
2014年6月至2019年3月,本组共纳入胸腰椎压缩性骨折病人84例,其中男15例,女69例,年龄59~ 97岁;无明确外伤史者51例,有明确外伤史者33例,均为轻微外伤,滑倒或摔倒引起;入院查骨密度均符合骨质疏松性骨折标准。骨折椎体分布:累及1节段68例、2节段15例、3节段1例,共累及101个椎体,其中T6 2例、T7 3例、T8 6例、T9 3例、T10 3例、T11 8例、T12 26例、L1 31例、L2 9例、L3 5例、L4 5例。
-
采用局麻(1%利多卡因注射液、罗哌卡因注射液、0.9%氯化钠溶液按1:1:2比例混合,每例剂量≤40 mg),精神过度紧张或多节段骨折同时进行PKP术或不耐受长时间俯卧者采用插管全麻。病人取俯卧位,加软垫使腹部悬空,适度过伸进行体位复位,手术在C形臂全程透视下进行。透视下定位骨折椎体及穿刺点做标记,采用经椎弓根两侧穿刺(椎弓根破损严重或者过于窄小者采用单侧穿刺),在导针引导下将空心钻钻入伤椎,建立工作通道,然后置入球囊至伤椎椎体前1/3进行扩张,尽可能复位椎体高度,将骨水泥在拉丝期经工作通道注入伤椎椎体内,有渗漏者及时停止,无渗漏者注射足够量尽可能使两侧弥散充分,每侧注入骨水泥2.00~3.75 mL,待硬化后拔出套管,无菌敷料覆盖切口。术后常规给予葡萄糖酸钙片、阿法骨化醇软胶囊、阿伦磷酸钠片等抗骨质疏松治疗,术后1~2 d病人佩戴支具下床活动,术后常规复查椎体正侧位片,了解骨水泥填充情况。
-
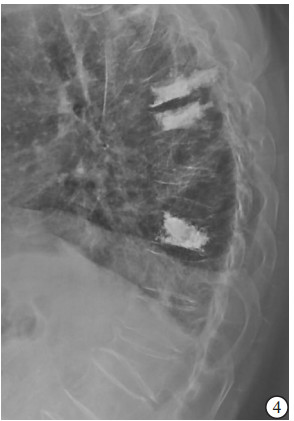
(1) 病人一般资料:包括性别、年龄、体质量指数(BMI)、骨密度,其中骨密度采用EXA-3000双能X线骨密度线仪对腰椎部位检查。(2)损伤节段数量、术前存在陈旧性椎体楔形变病例数及受累椎体数。(3)术中每个椎体骨水泥注入方式、骨水泥注射量。(4)术后有无骨水泥椎间盘渗漏、椎体前缘高度(anterior vertebral height,AVH)恢复率、术后后凸畸形角度。(5)力学结构类型:本研究将胸腰椎退变、陈旧性椎体楔形变和压缩性骨折PKP术后形成的胸腰椎结构分为以下8种类型:①屈度保持型,胸腰椎基本保持正常S形屈度,骨折节段局部后凸Cobb角<10°;②胸腰段局部后凸型,胸腰段椎体楔形变较重造成局部后凸畸形,Cobb角≥10°;③胸椎后凸型,超过正常范围的胸椎后凸畸形,而腰椎屈度正常;④胸椎后凸扩展型,胸腰段后凸畸形和胸椎后凸连续成比较平滑的更大范围的后凸,使胸椎后凸扩展到L1~L3节段;⑤腰椎变直型,腰椎生理前屈度显著减小或变直,胸椎屈度正常;⑥胸椎变直型,胸椎后凸显著减少而腰椎屈度正常;⑦节段僵硬型,指有连续2个节段及以上骨质增生骨桥形成使得局部节段性僵硬;⑧结构缺陷型,先天发育因素及后天退变因素导致的胸腰椎结构性缺陷使结构畸形及节段不稳定,如腰椎滑脱、分节不良或半椎体畸形等(见图 1~8)。屈度保持型视为正常结构类型,其余视为异常结构类型。

图 1 屈度保持型

图 2 胸腰段局部后凸型

图 3 胸椎后凸型
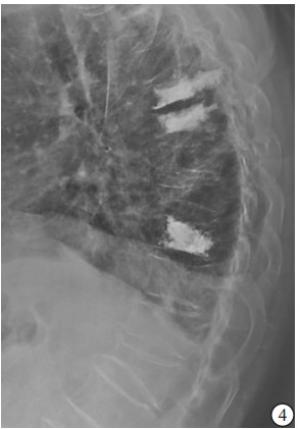
图 4 胸椎后凸扩展型

图 5 腰椎变直型

图 6 胸椎变直型

图 7 节段僵硬型
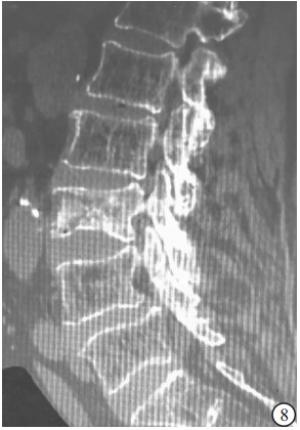
图 8 结构缺陷型
-
采用t(或t′)检验、χ2检验和Logistic回归分析。
-
84例病人术后均获得优良效果,7例次术后残余痛,经局部封闭或对症处理症状渐次缓解。术后均获随访12~57个月。因内科并发症死亡7例,死亡时手术均已超过12个月,死亡前腰痛症状缓解满意。PKP术后再发骨折13例,其中再发骨折1次10例、2次2例、4次1例,共18例次,再骨折部位发生于原骨折椎体(包括前驱陈旧性楔形变椎体)上方或下方相临椎体者12例次,间隔1个椎体者1例次,间隔2个椎体以上远隔椎体者4例次(原胸腰段骨折再发中胸段骨折3例次,再发下腰段骨折1例次),同时再发临椎及远隔椎体者1例次。18例次中,16例次再次入院行PKP术,2例次保守治疗,卧床休息及抗骨质疏松药物等治疗缓解。
-
单因素分析发现PKP术后再骨折病人BMI、骨密度均低于未再骨折病人(P<0.01);术前陈旧性椎体楔形变率、术后胸腰椎结构异常率高于未再骨折病人(P<0.05);而性别、年龄、损伤节段数、骨水泥注入方式、每椎体骨水泥注入量、骨水泥椎间渗漏、AVH恢复率和术后后凸畸形角度与未再骨折病人间差异无统计学意义(P>0.05)(见表 1)。
项目 再骨折(n=13) 未再骨折(n=71) χ2 P 性别(男/女) 3/10 12/59 0.20 >0.05 年龄(x±s)/岁 75.69±8.05 74.92±8.55 0.30* >0.05 BMI)/(kg/m2) 22.31±2.89 25.84±5.67 3.37△ <0.01 骨密度(x±s)/(g/cm2) 3.25±0.64 4.23±0.83 4.04* <0.01 损伤节段数(x±s) 1.63±0.73 1.78±0.81 0.62* >0.05 术前有陈旧性椎体楔形变 9(69.23) 26(36.62) 4.81 <0.05 骨水泥注入方式[n;百分率(%)] 单侧 2(11.11) 16(16.49) 0.33 >0.05 双侧 16(88.89) 81(83.51) 每椎体骨水泥注入量(x±s) 4.15±0.96 4.23±0.88 0.30* >0.05 骨水泥椎间渗漏[n;百分率(%)] 1(7.69) 4(5.63) — >0.05# AVH恢复率(x±s) 2.85±0.64 2.67±0.31 0.99* >0.05 术后后凸畸形角度(x±s)/(°) 14.12±1.87 13.17±1.69 1.83* >0.05 术后胸腰椎结构异常[n; 百分率(%)] 0(0.00) 26(36.62) 5.29 <0.05 *示t值;△示t′值;#示Fisher′s确切概率法 表 1 PKP术后再骨折的单因素分析
-
进一步logistic回归分析显示,BMI低、骨密度低、术前有陈旧性椎体楔形变及胸腰椎结构异常是术后椎体再骨折的危险因素(P<0.05~P<0.01)(见表 2)。
危险因素 B SE Wald χ2 P OR 95%CI BMI -0.44 0.14 9.18 <0.05 0.64 0.48~0.90 骨密度 -1.89 0.51 12.85 <0.01 0.08 0.08~0.38 椎体有陈旧性楔形变 1.41 0.66 4.57 <0.05 4.08 1.12~14.83 胸腰椎结构异常 -1.83 0.75 5.05 <0.05 0.16 0.04~0.75 表 2 PKP术后再骨折多因素logistic回归分析
-
随着社会进步,人均寿命延长,人口老龄化逐渐加重,老年OVCF发病率也呈现逐渐增高趋势,目前已经是一种临床极为常见疾病,主要表现为有诱因或者无明显诱因的胸腰部疼痛,伴活动受限,常规保守治疗如卧床休息,镇痛对症治疗,会导致长期卧床并发症的出现。PKP手术治疗骨质疏松性压缩性骨折目前已经取得了良好的近中期效果,其主要优势在于可以即时增加伤椎刚度及强度,恢复其稳定性,迅速有效缓解疼痛,改善脊柱后凸畸形,达到早期下床的目的,且相对安全,并发症较少,较PVP有更少的骨水泥渗漏,现已经被广泛认可和开展[7-9]。但随着该技术的广泛开展,术后椎体再骨折已成为较常见的并发症,给病人造成二次痛苦,严重影响病人的治疗信心和功能恢复。因而研究再骨折影响因素,及早采取相应预防措施具有重大现实意义。
关于椎体成形术后再骨折已有大量研究,尚无公认清晰的结论。本研究结果显示,PKP术后再骨折病人体质量更低、骨密度更低、术前已有椎体楔形变比例较高,且不少病人还是多节段变扁,这些病人多无明确的外伤病史,说明是陈旧的自发骨质疏松性压缩性骨折。同时低BMI、低骨密度和前驱陈旧性骨折楔形变均提示病人骨质疏松更严重。因而可以认为更严重的骨质疏松是椎体成形术后再骨折的主要原因。李智斐等[10]研究分析可能影响椎体成形术后诸多因素,认为低骨密度和骨质疏松是再骨折的根本原因。YOO等[11]对244例病人行PVP术后5年内随访,发现低骨密度是影响术后再骨折最重要的原因。RHO等[12]对临床资料进行多因素logistic回归分析得出:低骨密度是术后相邻椎体再发骨折唯一重要的因素。另有诸多研究[5-6, 13-16]发现再骨折的危险因素为非单一因素,而是多种危险因素,但其中低骨密度是再骨折的确定危险因素。且有研究[17]表明, 骨质疏松性椎体压缩骨折病人无论是否经过椎体成形术的治疗, 再次发生椎体压缩骨折的概率大约是首次发生椎体压缩骨折概率的4倍。综上所述,严重的骨质疏松是PKP术后再骨折的最主要的危险因素。
既往研究鲜有关注陈旧性椎体楔形变或陈旧性骨折对再骨折影响。本研究结果显示,再骨折病人术前陈旧性椎体楔形变率、术后胸腰椎结构异常率均高于未再骨折病人。陈旧性椎体楔形变、PKP术后残留楔形变,椎体强化硬度增加,承力点的变化导致的杠杆效应会导致原有结构的整体应力水平改变,从而加大再骨折风险。胸腰椎保持正常屈度时,利于纵向屈曲力的缓冲和分散,而各种异常的胸腰椎结构不利于纵向力的缓冲和分散,产生新的力学集中区和力学传导异常,因而易再骨折,且直接影响或决定着再发骨折的部位。同时骨折次数越多,脊柱正常结构破坏越重,失去正常屈度出现新的异常结构类型也是易再骨折的力学原因。
为预防PKP术后再骨折,要特别注意:(1)术后要高度重视系统抗骨质疏松治疗,并尽可能对病人进行长期随访监督指导。有研究[17-18]证实术后系统规律抗骨质疏松治疗有助于预防再骨折。(2)术后2个月内需佩戴胸腰部支具。椎体强化后,邻椎再骨折风险增加,特别是PKP术后有胸腰段、中胸椎后凸畸形或胸椎后凸扩展型病人,术后早期需要对病人临近椎体进行适应强化,因而有必要早期佩戴支具,防止再骨折。(3)重视早期活动指导,应嘱病人避免一切可能加重剪力的动作,如弯腰起床过急过猛、突然弯腰拾物、搬提重物、剧烈咳嗽、打喷嚏等;并嘱病人严防外伤、滑倒等。
骨质疏松性胸腰椎压缩性骨折PKP术后再骨折危险因素分析
Analysis of risk factors of the re-fracture of osteoporotic thoracolumbar compression fractures after PKP
-
摘要:
目的探讨骨质疏松性胸腰椎压缩性骨折球囊扩张椎体后凸成形术(PKP)术后再骨折的相关危险因素。 方法回顾分析84例PKP术治疗的胸腰椎骨质疏松性压缩性骨折病人的临床资料,术后均获随访12~57个月;根据病人随访期间是否发生再骨折,将病人分为再骨折组和未再骨折组,对2组病人的性别、年龄、体质量指数、骨密度、损伤节段数量、术前陈旧性楔形变椎体率及受累椎体数、骨水泥注入方式、骨水泥注射量、术后有无椎间盘骨水泥渗漏、椎体前缘高度恢复率、术后后凸畸形角度和胸腰椎结构类型进行对比分析。 结果84例病人术后再骨折13例(18例次)。单因素分析显示,PKP再骨折组体质量指数、骨密度均低于未再骨折组(P<0.01),术前陈旧性椎体楔形变率、术后胸腰椎结构异常率高于未再骨折组(P<0.05)。logistic回归分析显示,体质量指数低、骨密度低、术前有陈旧性椎体楔形变及胸腰椎结构异常是PKP术后再骨折的危险因素(P<0.05~P<0.01)。 结论骨质疏松和胸腰椎结构的损伤程度是诱发骨质疏松性胸腰椎压缩性骨折PKP术后再骨折的危险因素。 -
关键词:
- 压缩性骨折 /
- 胸腰椎 /
- 骨质疏松 /
- 球囊扩张椎体后凸成形术 /
- 再骨折
Abstract:ObjectiveTo explore the risk factors of the refracture of osteoporotic thoracolumbar compression fractures after percutaneous kyphoplasty(PKP). MethodsThe clinical data of 84 osteoporotic thoracolumbar compression fractures patients treated with PKP were retrospectively analyzed.All patients were followed up for 12 to 57 months.The patients were divided into the refracture group and non-refracture group according to the refracture condition.The gender, age, body mass index(BMI), bone mineral density(BMD), number of injured vertebrae, number of cases with wedge-shaped vertebral bodies, number of involved vertebrae, way of bone cement injection, bone cement injection volume, intervertebral disc leakage of bone cement, anterior vertebral height restoration, postoperative kyphosis and structural type of thoracolumbar vertebrae were compared between two groups. ResultsAmong 84 patients, the postoperative secondary fracture in 13 cases(18 times) after PKP were found.The results of univariate analysis showed the BMI and BMD in refracture group were lower than those in non-refracture group(P < 0.01), and the postoperative thoracolumbar structural abnormality rate in refracture group were higher than those in non-refracture group(P < 0.05).The results of logistic regression analysis showed that the body mass index, bone mineral density, preoperative old vertebral wedge-shaped change and postoperative thoracolumbar structural abnormality rate were the high risk factors of postoperative vertebral refracture. ConclusionsThe osteoporosis and degree of thoracolumbar structural injury are the risk factors of osteoporotic thoracolumbar compression fracture after PKP. -
Key words:
- compression fracture /
- thoracolumbar /
- osteoporosis /
- percutaneous kyphoplasty /
- refracture
-
表 1 PKP术后再骨折的单因素分析
项目 再骨折(n=13) 未再骨折(n=71) χ2 P 性别(男/女) 3/10 12/59 0.20 >0.05 年龄(x±s)/岁 75.69±8.05 74.92±8.55 0.30* >0.05 BMI)/(kg/m2) 22.31±2.89 25.84±5.67 3.37△ <0.01 骨密度(x±s)/(g/cm2) 3.25±0.64 4.23±0.83 4.04* <0.01 损伤节段数(x±s) 1.63±0.73 1.78±0.81 0.62* >0.05 术前有陈旧性椎体楔形变 9(69.23) 26(36.62) 4.81 <0.05 骨水泥注入方式[n;百分率(%)] 单侧 2(11.11) 16(16.49) 0.33 >0.05 双侧 16(88.89) 81(83.51) 每椎体骨水泥注入量(x±s) 4.15±0.96 4.23±0.88 0.30* >0.05 骨水泥椎间渗漏[n;百分率(%)] 1(7.69) 4(5.63) — >0.05# AVH恢复率(x±s) 2.85±0.64 2.67±0.31 0.99* >0.05 术后后凸畸形角度(x±s)/(°) 14.12±1.87 13.17±1.69 1.83* >0.05 术后胸腰椎结构异常[n; 百分率(%)] 0(0.00) 26(36.62) 5.29 <0.05 *示t值;△示t′值;#示Fisher′s确切概率法  下载: 导出CSV
下载: 导出CSV
表 2 PKP术后再骨折多因素logistic回归分析
危险因素 B SE Wald χ2 P OR 95%CI BMI -0.44 0.14 9.18 <0.05 0.64 0.48~0.90 骨密度 -1.89 0.51 12.85 <0.01 0.08 0.08~0.38 椎体有陈旧性楔形变 1.41 0.66 4.57 <0.05 4.08 1.12~14.83 胸腰椎结构异常 -1.83 0.75 5.05 <0.05 0.16 0.04~0.75
下载: 导出CSV
-
[1] 李军, 吴家昌, 蒋勇, 等.椎体成形术与椎体后凸成形术治疗椎体压缩性骨折疗效的Meta分析[J].中国矫形外科杂志, 2014, 22(8):696. doi: 10.3977/j.issn.1005-8478.2014.08.06 [2] BLASCO J, MARTINEZ-FERRER A, MACHO J, et al.Effect of vertebroplasty on pain relief, quality of life, and the incidence of new vertebral fractures:a 12-month randomized follow-up controlled trial[J].J Bone Mineral Res, 2012, 27(5):1159. doi: 10.1002/jbmr.1564 [3] KIM JH, YOO SH, KIM JH.Long-term follow-up of percutaneous vertebroplasty in osteo-porotic compression fracture:minimum of 5 years follow-up[J].Asian Spine J, 2012, 6(1):6. doi: 10.4184/asj.2012.6.1.6 [4] LEE WS, SUNG KH, JEONG HT, et al.Risk factors of developing new symptomatic vertebral compression fractures after percutaneous vertebroplasty in osteoporotic patients[J].Eur Spine J, 2011, 15(12):1777. [5] 朱书涛, 刘洋, 张明辉, 等.PKP术后患者再骨折危险因素分析[J].中国矫形外科杂志, 2016, 24(16):1445. [6] 李仁波, 尚静波, 姜丽.PKP治疗骨质疏松性压缩骨折后椎体再骨折的原因分析[J].大连医科大学学报, 2018, 40(1):43. [7] 马树伟, 吴继功, 马华松, 等.PKP治疗急性期及亚急性期椎体压缩骨折的效果分析[J].河北医科大学学报, 2018, 39(3):280. doi: 10.3969/j.issn.1007-3205.2018.03.008 [8] 李小宏, 张有为, 刘列, 等.PKP和PVP治疗骨质疏松性椎体压缩骨折的疗效比较[J].临床骨科杂志, 2018, 21(2):150. doi: 10.3969/j.issn.1008-0287.2018.02.009 [9] 黄文显, 邓颂波, 曾日祥, 等.PVP和PKP治疗骨质疏松性椎体压缩骨折临床随机对照研究[J].泰山医学院学报, 2019, 40(1):41. doi: 10.3969/j.issn.1004-7115.2019.01.012 [10] 李智斐, 付拴虎, 张家立, 等.椎体成形术后再骨折相关因素分析[J].中国脊柱脊髓杂志, 2014, 24(9):790. doi: 10.3969/j.issn.1004-406X.2014.09.05 [11] YOO CM, PARK KB, HWANG SH, et al.The analysis of patterns and risk factors of newly developed vertebral compression fractures after percutaneous vertebroplasty[J].J Korean Neurosurg Soc, 2012, 52(4):339. doi: 10.3340/jkns.2012.52.4.339 [12] RHO YJ, CHOE WJ, Chun YI.Risk factors predicting the new symptomatic vertebral compression fractures after percutaneous vertebroplasty or kyphoplasty[J].Eur Spine J, 2012, 21(5):905. doi: 10.1007/s00586-011-2099-5 [13] 彭冉东, 邓强, 李中锋, 等.骨质疏松性椎体压缩骨折PKP术后近期手术椎体再骨折原因探讨[J].实用骨科杂志, 2017, 23(9):781. [14] 李格, 梅伟, 刘沛霖, 等.骨质疏松性椎体压缩骨折经皮椎体成形术后邻近椎体再骨折的危险因素探讨[J].中医正骨, 2016, 28(6):18. [15] 王芳芳, 刘红正, 王拴池, 等.PVP术后手术强化椎再骨折因素分析[J].西部医学, 2018, 30(8):1150. doi: 10.3969/j.issn.1672-3511.2018.08.013 [16] 林森, 陈小强, 周涛, 等.骨质疏松性椎体压缩性骨折椎体成形术后再骨折的影响因素分析[J].中华临床医师杂志, 2016, 10(12):1670. doi: 10.3877/cma.j.issn.1674-0785.2016.12.003 [17] 吴鹏, 王博, 刘康, 等.唑来膦酸钠对高转换患者椎体成形术后椎体再骨折发生率影响因素的相关性分析[J].中国骨质疏松杂志, 2017, 23(8):1075. doi: 10.3969/j.issn.1006-7108.2017.08.021 [18] 段学会.椎体成形结合抗骨质疏松治疗减少再骨折发生率的可行性研究[J].青岛医药卫生, 2018, 50(1):32. doi: 10.3969/j.issn.1006-5571.2018.01.011 -

 点击查看大图
点击查看大图

图(8)表(2)
计量
- 文章访问数: 4341
- HTML全文浏览量: 2037
- PDF下载量: 11
- 被引次数: 0
