

-
肝外胆管癌(extrahepatic cholangiocarcinoma,EHCC)早期诊断率较低,手术可切除率仅为20%~35%[1-2]。近年来,胆道引流及胆道支架植入术因可显著解除胆管癌病人胆道梗阻症状、改善病人生存状况,已被国内外部分学者应用于晚期EHCC的治疗[3-4]。化疗是晚期EHCC的重要治疗方法,然而整体疗效较差[5-6]。与静脉内途径相比,增加肿瘤组织中化学治疗药物的浓度可具有抗肿瘤作用。腔内给药途径将药物直接递送至肿瘤组织,从而起到抗肿瘤的作用。多项临床研究已经证实,腔内灌注化疗在卵巢癌伴胸膜转移、尿道上皮癌、结直肠癌腹膜转移、胶质母细胞瘤、恶性胸腹水等多种肿瘤的治疗应用中安全、有效[7-12]。部分学者曾对EHCC病人行经皮经肝腔内灌注化疗的治疗尝试,发现可取得较好的临床效果,且对肝脏和胆道的损伤程度较低[13],但其疗效仍需要更多的临床研究加以验证。本中心自2012年1月起对晚期EHCC病人行经皮经肝胆道支架置入(PTBS)治疗,并根据病人意愿联合或不联合125I腔内照射,取得了令人满意的疗效[14-16]。然而,有些病人并不愿接受125I粒子置入。我们根据病人及家属意愿,对部分病人采用了PTBS联合5-氟脲嘧啶(5-Fu)和丝裂霉素腔内灌注化疗,并与单纯行PTBS治疗的晚期EHCC病人的临床资料作一对比分析。
-
收集2012年1月至2017年4月在我科住院的晚期EHCC病人资料。纳入标准:(1)经病理和/或临床诊断为肝门部胆管癌(HCCA)或远端胆管癌(DCCA);(2)术前评估肿瘤不可切除的晚期胆管癌者;(3)接受PTBS但不愿意进一步接受125I粒子置入治疗;(4)肝内胆管扩张≥4 mm。排除标准:(1)良性胆道狭窄;(2)既往因EHCC接受过手术、内镜下支架植入或全身化疗等治疗;(3)既往接受过PTBS联合腔内放疗、全身放化疗等;(4)凝血功能显著异常;(5)肝肾功能衰竭者;(6)肿瘤已腹腔广泛转移失去治疗意义者;(7)处于终末期而无法耐受该手术者;(8)随访等资料不完整。最终,共纳入86例病人,其中,PTBS组71例,PTBS+腔内灌注化疗组15例。本研究遵守赫尔辛基宣言[17],并通过了我院伦理委员会的批准。
-
(1) 数字减影血管造影(DSA)设备购自美国GE公司,型号为Innova3100。(2)胆道支架购自南京微创医疗科技有限公司,是一种带有编织支架的镍钛形状记忆合金材料。术中根据胆道病变情况选择相应的规格(8 mm×40 mm,8 mm×60 mm,8 mm×80 mm,8 mm×100 mm,10 mm×40 mm,10 mm×60 mm,10 mm×80 mm,10 mm×100 mm);(3)超滑导丝和间隔导管均购自日本Terumo公司;(4)柱状扩张球囊购自瑞士百多力公司;(5)碘佛醇(规格:50 mL/33.9 g,每毫升含320 mg碘)(江苏恒瑞医药股份有限公司)。
-
(1) 术前准备:病人入院后完善血常规、生化常规、凝血功能、肿瘤指标、肝胆胰脾彩超、MRCP和MDCT等检查,评估病人的一般状态、胆道梗阻情况、肿瘤部位及范围等;排除手术禁忌后,制定手术方案,同时告知病人及家属后签署知情同意书。(2)手术方法:病人术前如有梗阻性黄疸、胆道感染等表现,均先在B超引导下行PTCD术。若病人一般情况良好,且无胆道出血等并发症,于PTCD术后5~7 d后在DSA下行PTBS术(见图 1)。手术步骤:病人平卧于DSA操作台上,经PTCD管注入稀释的碘佛醇进行造影,显示胆道狭窄的部位及胆管扩张情况(见图 1A);经PTCD管置入导丝后置换外鞘管,然后置入单弯造影导管,配合造影导管调整导丝越过梗阻部位进入十二指肠(见图 1B);进一步造影并测量梗阻段长度及宽度(见图 1C),根据梗阻情况选择合适规格的胆道支架沿导丝植入梗阻位置(见图 1D);循导丝再次置入合适型号的外引流导管(PTCD管),外周固定,外接抗反流引流袋。(4)胆管腔内灌注化疗:5-Fu 1 000 mg+0.9%氯化钠溶液250 mL,联合丝裂霉素6 mg+0.9%氯化钠溶液250 mL,每种药物经PTCD导管缓慢滴注3~4 h,每2周1次,共6~8次。
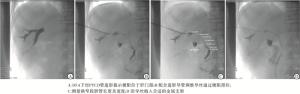
图 1 PTBS手术过程
-
术后常规使用抗生素预防感染、生长抑素、保肝、止血等对症治疗;术后1 h及次日早晨6时急查血淀粉酶,次日早晨复查血常规、生化常规,并密切观察病人术后并发症的情况。术后2~3 d如病人无畏寒、发热、腹痛、腹胀等不适,且引流液<100 mL/d,即关闭外引流管。收集病人的年龄、性别、肿瘤部位和相关实验室检查结果,包括血清总胆红素(TBIL)、丙氨酸氨基转移酶(ALT)、天门冬氨酸氨基转移酶(AST)、碱性磷酸酶(ALP)、谷酰转肽酶(GGT)、白蛋白(ALB)、CA19-9及癌胚抗原(CEA)等。
2组病人均随访至2017年9月或至病人死亡。随访内容包括:术后1、3及6月复查生化常规、肿瘤指标、腹部彩超、腹部立位平片;观察术后1、3及6月血清中ALT、AST、TBIL、DBIL、ALP及ALB水平的变化;每3月复查一次薄层CT,随访中有异常情况或并发症的发生,则及时处理。
-
采用t检验、秩和检验、χ2检验、单因素方差分析、Kaplan-Meier(KM)生存曲线、log-rank检验及多因素Cox回归模型。
-
PTBS组共71例,其中男43例,女38例;HCCA 44例,DCCA 27例。PTBS+腔内灌注化疗组共15例,其中男10例,女5例;HCCA 11例,DCCA 4例。2组之间性别、年龄、肿瘤部位、CA19-9、CEA、ALB及TBIL水平差异均无统计学意义(P>0.05);与PTBS组相比,PTBS+腔内灌注化疗组病人有较高的术前ALT、AST、ALP及GGT(P<0.05)(见表 1)。
基线资料 PTBS组(n=71) PTBS+腔内灌注化疗组(n=15) uc P 男/女 43/28 10/5 0.20▲ >0.05 年龄 68.8±14.1 66.8±9.5 0.52△ >0.05 HCCA/DCCA 44/27 11/4 0.69▲ >0.05 CA19-9/(ng/mL) 886(1.1~1967) 636.6(6.68~1200) 0.22 >0.05 CEA/(ng/mL) 4.35(0.96~490.51) 5.69(1.40~40.32) 0.27 >0.05 ALT/(U/L) 106(18~542) 149(67~273) 2.16 <0.05 AST/(U/L) 98(19~793) 158(56~347) 2.69 <0.01 ALP/(U/L) 404(102~1990) 685(176~1734) 2.41 <0.05 GGT/(U/L) 406(47~1837) 683(102~2528) 2.22 <0.05 TBIL/(μmol/L) 158(5.8~551.5) 212.4(108.3~706.2) 1.83 <0.05 ALB/(g/L) 34.6(25.1~43.6) 34.3(31.1~40.5) 0.62 >0.05 △示t值;▲示χ2值 表 1 病人基线资料比较
-
2组病人的临床症状(如皮肤瘙痒、发热等)均有不同程度的改善。与术前相比,PTBS组病人术后1月、3月及6月血清中ALT、AST及TBIL水平均有不同程度的降低(P<0.05),病人术后ALB水平的变化不明显(P>0.05);与术前相比,PTBS+腔内灌注化疗组病人术后1月、3月及6月血清中ALT、AST及TBIL水平均有不同程度的降低(P<0.05),且下降趋势比PTBS组更为显著;与术前相比,PTBS+腔内灌注化疗组病人术后1个月、3个月及6个月血清中ALB水平明显增加(P<0.05)(见表 2)。
分组 n 术前 术后1月 术后3月 术后6月 F P MS组内 TBIL/(μmol/L) PTBS组 71 198.9±16.8 55.7±13.6* 118.2±32.7* 57.2±37.2*# 443.50 <0.01 730.083 PTBS+腔内灌注化疗组 15 275.4±41.3 45.1±8.9* 20.4±5.9* 28.2±5.5*# 412.40 <0.01 462.491 t — 11.81 2.88 11.49 2.30 — — — P — <0.01 <0.01 <0.01 <0.01 — — — ALB/(g/L) PTBS组 71 34.2±0.5 34.3±0.8 33.2±1.4*■ 31.8±4.0*■# 20.33 0.01 4.713 PTBS+腔内灌注化疗组 15 35.1±0.8 39.6±1.0* 41.1±0.6* 38.5±0.9*# 138.80 <0.01 0.703 t — 5.64 22.29 21.36 6.42 — — — P — <0.01 <0.01 <0.01 <0.01 — — — ALT/(U/L) PTBS组 71 133.4±12.5 43.8±5.4* 90.2±25.6* 52.5±22.1*# 357.71 <0.01 332.295 PTBS+腔内灌注化疗组 15 160.6±16.0 60.8±7.7* 49.8±11.4* 64.3±18.8*# 199.42 <0.01 199.673 t — 7.30 10.23 1.92 0.41 — — — P — <0.01 <0.01 <0.01 >0.05 — — — AST/(U/L) PTBS组 71 130.4±15.2 56.3±9.5* 135.3±49.6 32.1±7.8*# 271.90 0.01 710.573 PTBS+腔内灌注化疗组 15 171.5±19.9 69.1±9.4* 64.2±15.0* 70.6±22.0*■# 135.11 <0.01 298.343 t — 9.00 4.75 5.48 11.82 — — — P — <0.01 <0.01 <0.01 <0.01 — — — 与术前比较*P<0.05;与术后1月比较■P<0.05;与术后3月比较#P<0.05 表 2 2组病人术后主要生化指标的变化情况
-
PTBS组病人术后总体并发症发生率为12.7%(9/71),其中6例出现高淀粉酶血症;有3例出现胆道感染,无其他严重并发症及围手术期死亡。PTBS+腔内灌注化疗组病人术后总体并发症发生率为13.3%(2/15),均为高淀粉酶血症,没有其他严重并发症,未发现由灌注化疗引起的相关并发症如肠黏膜损伤、肠功能紊乱等,无围手术期死亡。2组术后并发症的发生率差异无统计学意义(P>0.05)。
PTBS组术后共有25例(35.2%)病人发生胆道再次梗阻;PTBS+腔内灌注化疗组术后3例(20.0%)病人发生胆道再次梗阻。联合腔内灌注化疗降低了胆道再梗阻发生的风险,但2组间的差异无统计学意义(χ2=1.30,P>0.05)。
-
随访病人至2017年9月或至病人死亡。结果显示,PTBS组病人生存时间中位数为7(四分位数间距:4~10)个月,半年生存率为54.5%,1年生存率为11.3%;PTBS+腔内灌注化疗组病人生存时间中位数为10(四分位数间距:7~14)个月,半年生存率为86.7%,1年生存率为37.5%;log-rank检验提示2组之间总生存时间(OS)差异有统计学意义(χ2=6.27,P<0.05)。
单因素分析表明,术前CA19-9及治疗方式是病人术后OS的主要影响因素(见表 3)。随后,上述两个因素进入Cox多因素回归模型,结果表明接受PTBS+腔内灌注化疗和CA19-9(P<0.05<P<0.01)是独立的保护性预后因素。
变量 单因素分析 多因素分析 HR(95%CI) P HR(95%CI) P 性别 1.125(0.699~1.811) >0.05 2.285(1.308~3.993) <0.01 年龄 1.197(0.752~1.906) >0.05 DCCA/HCCA 1.040(0.638~1.694) >0.05 CA19-9 2.176(1.426~3.319) <0.01 ALT 1.058(0.688~1.626) >0.05 AST 1.100(0.703~1.724) >0.05 TBIL 1.003(0.954~1.055) >0.05 ALB 1.028(0.834~1.267) >0.05 PTBS+腔内灌注化疗/PTBS 0.454(0.229~0.902) <0.05 0.459(0.230~0.918) <0.05 表 3 影响病人术后OS的单因素和多因素分析
-
EHCC是一种源自胆管上皮细胞的高度恶性肿瘤,因其发病隐匿且缺乏特异性筛查手段,多数病人就医时已失去根治性手术治疗机会。目前,晚期胆管癌的主要姑息性治疗方法有:姑息性手术、经内镜治疗、经皮穿刺治疗以及联合射频消融、介入、化疗、内放射、外放射、分子靶向治疗等[18]。
经PTCD途径的胆道引流可缓解胆道梗阻、减轻胆道炎症及改善病人的生存状况[19-20]。此外,在PTCD基础上可同时给予化疗、放疗、获取标本活检等操作或治疗。PTBS是恶性梗阻性黄疸病人非手术治疗的有效手段,其具有恢复生理胆汁引流以减少胆汁及电解质等流失、手术创伤小及适应证广等特点[21],然而,单纯的支架置入并不能抑制肿瘤的生长,且支架再次狭窄或堵塞亦是影响病人预后的高危因素[22]。腔内灌注化疗目前常应用于恶性胸水、恶性腹水等。对于EHCC,腔内灌注化疗相关的报道较少。而腔内灌注化疗一般选用经典的、局部刺激小、抗肿瘤效果好、腔内注药后曲线下面积高于血浆的药物。目前使用较多的有顺铂、氟脲嘧啶、丝裂霉素、阿霉素、吉西他滨、长春瑞滨等。这些药物可通过降低CD4+CD25+调节性T细胞的水平和改善免疫抑制状态来抑制肿瘤的进展[23]。
在本中心,无手术指征的晚期EHCC病人常规行PTBS治疗,并同时行腔内125I放疗。然而,部分病人因各种原因不愿接受125I粒子置入。5-Fu是S期特异性广谱抗肿瘤药物,其可干扰肿瘤细胞中蛋白质的合成,从而对肿瘤细胞起到毒性和杀伤作用。丝裂霉素可以解聚细胞DNA,阻断DNA复制,从而抑制肿瘤细胞分裂。两者的联合使用可通过促进细胞凋亡、抑制细胞增殖、促进肿瘤细胞自噬从而取得较好的抗肿瘤作用[24]。基于此,我们尝试经PTCD管灌注5-Fu和丝裂霉素以改善病人的预后。
本研究结果表明,与单纯PTBS相比,PTBS联合腔内灌注化疗降低了胆道支架再梗阻的风险,说明胆管腔内灌注化疗对癌肿的腔内生长可起到一定的抑制作用。2组再梗阻率差异无统计学意义可能和纳入的病例数量过少有关。同时,由于PTBS联合腔内灌注化疗组较低的再梗阻率,该组病人术后血清中ALB水平增加更为明显,间接反映出改组病人更佳的生活质量。此外,联合腔内灌注化疗可将病人的生存时间从7个月延长至10个月,从而为晚期EHCC病人寻求更全面的治疗机会。当然,在化疗方案的选择上还需要进一步联合肿瘤内科及病理科等相关科室制定个性化的化疗方案,以期取得更佳的治疗效果。由于灌注的化疗药物会迅速进入肠道,且化疗药物对肠道黏膜和功能可能有影响,我们在本研究中对药物的灌注速度进行了严格控制(持续3~4 h),未发现灌注化疗药物相关的并发症,提示该腔内灌注化疗方法安全、有效。因本研究为回顾性研究且样本量较小,且联合腔内灌注化疗组治疗前ALT、AST、ALP、GGT水平显著高于单纯PTBS组,可能对研究结果有影响,具体结论仍需进一步临床研究分析。
综上所述,与单纯PTBS相比,PTBS联合胆管腔内灌注化疗可获得更佳治疗效果。具体化疗方案可根据个体差异性而适时调整,MDT模式是最终趋势。总的来说,该方法值得临床进一步研究与探索。
胆道支架植入联合胆管腔内灌注化疗在晚期肝外胆管癌中的应用
Effect of biliary stent implantation combined with intrabile duct perfusion chemotherapy in the treatment of advanced extrahepatic cholangiocarcinoma
-
摘要:
目的探讨胆道支架植入联合胆管腔内灌注化疗在晚期胆管癌中的治疗效果。 方法回顾性分析经皮经肝胆道支架置入(PTBS,PTBS组)或PTBS联合腔内灌注化疗(PTBS+腔内灌注化疗组)的86例晚期EHCC病人的临床资料,分析病人肝功能的改善情况、并发症发生情况及术后生存情况等。Kaplan-Meier曲线及Cox比例风险回归模型分析影响病人术后总体生存时间(OS)的相关因素。 结果与术前相比,2组病人术后1月、3月及6月血清中ALT、AST及TBIL水平均有不同程度的降低(P < 0.05),且PTBS+腔内灌注化疗组病人下降趋势比PTBS组更为显著;PTBS+腔内灌注化疗组病人术后血清ALB水平增加更为明显。2组病人术后并发症的发生差异无统计学意义(P>0.05)。PTBS组病人生存时间中位数为7个月,1年生存率为11.3%;PTBS+腔内灌注化疗组病人生存时间中位数为10个月,1年生存率为37.5%。log-rank检验提示PTBS联合腔内灌注化疗可改善EHCC病人的预后,延长其生存期。Cox多因素回归模型结果表明接受PTBS+腔内灌注化疗是预后独立的保护性因素(HR=0.46,95%CI:0.23~0.92,P < 0.05)。 结论与单纯PTBS相比,PTBS联合腔内灌注化疗可改善EHCC病人的预后,延长其生存期。PTBS联合腔内灌注化疗可获得更佳治疗效果,值得临床进一步探索与研究。 Abstract:ObjectiveTo explore the effects of biliary stent implantation combined with intrabile duct perfusion chemotherapy in the treatment of advanced extrahepatic cholangiocarcinoma(EHCC). MethodsThe clinical data of 86 advanced EHCC patients treated with percutaneous extrahepatic biliary stenting(PTBS group) or PTBS combined with intraductal perfusion chemotherapy(PTBS combined with intraductal perfusion chemotherapy group) were retrospectively analyzed.The improvement of liver function, complications and postoperative survival were analyzed.The influencing factors of overall survival(OS) were analyzed using Kaplan-Meier curve and Cox regression model. ResultsCompared with before operation, the serum levels of ALT, AST and TBIL significantly reduced after 1, 3 and 6 months of operation(P < 0.05), the decreasing degree of which in PTBS combined with intraductal perfusion chemotherapy group was more obviously than that in PTBS group, and the increasing degree of ALB level in PTBS combined with intraductal perfusion chemotherapy group was more obviously than that in PTBS group.The difference of the incidence rate of postoperative complication between two groups was not statistically significant(P>0.05).The median survival time and 1-year survival rate in PTBS group were 7 months and 11.3%, respectively.The median survival time and 1-year survival rate in PTBS combined with intraductal perfusion chemotherapy group were 10 months and 37.5%, respectively.Log-rank test suggested that the PTBS combined with intraductal perfusion chemotherapy could improve the prognosis, and prolong the survival of EHCC patients.Cox regression analysis showed that the PTBS combined with intraductal perfusion chemotherapy was an independent protective factor for prognosis(HR=0.46, 95%CI:0.23-0.92, P < 0.05). ConclusionsCompared with the simple PTBS, the PTBS combined with intraductal perfusion chemotherapy can improve the prognosis, and prolong the survival of EHCC patients.The PTBS combined with intraductal perfusion chemotherapy has good treatment effect, which is worthy of further clinical exploration and research. -
表 1 病人基线资料比较
基线资料 PTBS组(n=71) PTBS+腔内灌注化疗组(n=15) uc P 男/女 43/28 10/5 0.20▲ >0.05 年龄 68.8±14.1 66.8±9.5 0.52△ >0.05 HCCA/DCCA 44/27 11/4 0.69▲ >0.05 CA19-9/(ng/mL) 886(1.1~1967) 636.6(6.68~1200) 0.22 >0.05 CEA/(ng/mL) 4.35(0.96~490.51) 5.69(1.40~40.32) 0.27 >0.05 ALT/(U/L) 106(18~542) 149(67~273) 2.16 <0.05 AST/(U/L) 98(19~793) 158(56~347) 2.69 <0.01 ALP/(U/L) 404(102~1990) 685(176~1734) 2.41 <0.05 GGT/(U/L) 406(47~1837) 683(102~2528) 2.22 <0.05 TBIL/(μmol/L) 158(5.8~551.5) 212.4(108.3~706.2) 1.83 <0.05 ALB/(g/L) 34.6(25.1~43.6) 34.3(31.1~40.5) 0.62 >0.05 △示t值;▲示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 2组病人术后主要生化指标的变化情况
分组 n 术前 术后1月 术后3月 术后6月 F P MS组内 TBIL/(μmol/L) PTBS组 71 198.9±16.8 55.7±13.6* 118.2±32.7* 57.2±37.2*# 443.50 <0.01 730.083 PTBS+腔内灌注化疗组 15 275.4±41.3 45.1±8.9* 20.4±5.9* 28.2±5.5*# 412.40 <0.01 462.491 t — 11.81 2.88 11.49 2.30 — — — P — <0.01 <0.01 <0.01 <0.01 — — — ALB/(g/L) PTBS组 71 34.2±0.5 34.3±0.8 33.2±1.4*■ 31.8±4.0*■# 20.33 0.01 4.713 PTBS+腔内灌注化疗组 15 35.1±0.8 39.6±1.0* 41.1±0.6* 38.5±0.9*# 138.80 <0.01 0.703 t — 5.64 22.29 21.36 6.42 — — — P — <0.01 <0.01 <0.01 <0.01 — — — ALT/(U/L) PTBS组 71 133.4±12.5 43.8±5.4* 90.2±25.6* 52.5±22.1*# 357.71 <0.01 332.295 PTBS+腔内灌注化疗组 15 160.6±16.0 60.8±7.7* 49.8±11.4* 64.3±18.8*# 199.42 <0.01 199.673 t — 7.30 10.23 1.92 0.41 — — — P — <0.01 <0.01 <0.01 >0.05 — — — AST/(U/L) PTBS组 71 130.4±15.2 56.3±9.5* 135.3±49.6 32.1±7.8*# 271.90 0.01 710.573 PTBS+腔内灌注化疗组 15 171.5±19.9 69.1±9.4* 64.2±15.0* 70.6±22.0*■# 135.11 <0.01 298.343 t — 9.00 4.75 5.48 11.82 — — — P — <0.01 <0.01 <0.01 <0.01 — — — 与术前比较*P<0.05;与术后1月比较■P<0.05;与术后3月比较#P<0.05
下载: 导出CSV
表 3 影响病人术后OS的单因素和多因素分析
变量 单因素分析 多因素分析 HR(95%CI) P HR(95%CI) P 性别 1.125(0.699~1.811) >0.05 2.285(1.308~3.993) <0.01 年龄 1.197(0.752~1.906) >0.05 DCCA/HCCA 1.040(0.638~1.694) >0.05 CA19-9 2.176(1.426~3.319) <0.01 ALT 1.058(0.688~1.626) >0.05 AST 1.100(0.703~1.724) >0.05 TBIL 1.003(0.954~1.055) >0.05 ALB 1.028(0.834~1.267) >0.05 PTBS+腔内灌注化疗/PTBS 0.454(0.229~0.902) <0.05 0.459(0.230~0.918) <0.05
下载: 导出CSV
-
[1] RIZVI S, KHAN SA, HALLEMEIER CL, et al.Cholangiocarcinoma-evolving concepts and therapeutic strategies[J].Nat Rev Clin Oncol, 2018, 15(2):95. doi: 10.1038/nrclinonc.2017.157 [2] PU LZ, SINGH R, LOONG CK.Malignant biliary obstruction:evidence for best practice[J].Gastroenterol Res Pract, 2016, 2016(11):1. [3] SON RC, GWON DI, KO HK, et al.Percutaneous unilateral biliary metallic stent placement in patients with malignant obstruction of the biliary hila and contralateral portal vein steno-occlusion[J].Korean J Radiol, 2015, 16(3):586. doi: 10.3348/kjr.2015.16.3.586 [4] RAZUMILAVA N, GORES GJ.Classification, diagnosis, and management of cholangiocarcinoma[J].Clin Gastroenterol Hepatol, 2013, 11(1):13. [5] LEWIS HL, RAHNEMAI-AZAR AA, DILLHOFF M, et al.Current management of perihilar cholangiocarcinoma and future perspectives[J].Chirurgia, 2017, 112(3):193. doi: 10.21614/chirurgia.112.3.193 [6] PARK K, KIM KP, PARK S, et al.Comparison of gemcitabine plus cisplatin versus capecitabine plus cisplatin as first-line chemotherapy for advanced biliary tract cancer[J].Asia Pac J Clin Oncol, 2017, 13(1):13. doi: 10.1111/ajco.2017.13.issue-1 [7] JUN SY, SEOK YK, KATO T, et al.Hyperthermic intrathoracic chemotherapy with cisplatin for ovarian cancer with pleural metastasis[J].Obstet Gynecol Sci, 2017, 60(3):308. doi: 10.5468/ogs.2017.60.3.308 [8] MAURICE MJ, MADI R, CHUANG DY, et al.Retrograde chemoinfusion of the upper tract:standardizing the delivery of topical adjuvant therapy[J].J Endourol, 2013, 27(5):540. doi: 10.1089/end.2012.0608 [9] CEELEN W, VAN NIEUWENHOVE Y, PATTYN P.Surgery and intracavitary chemotherapy for peritoneal carcinomatosis from colorectal origin[J].Acta Gastroenterol Belg, 2008, 71(4):373. [10] WESTPHAL M, LAMSZUS K, HILT D.Intracavitary chemotherapy for glioblastoma:present status and future directions[J].Acta Neurochir Suppl, 2003, 88:61. doi: 10.1007/978-3-7091-6090-9 [11] 马泰, 潘跃银, 孙国平, 等.恶性胸/腹腔积液病人腔内应用贝伐珠单抗的价值及疗效影响因素分析[J].中华疾病控制杂志, 2017(7):727. [12] 于建全, 冯飞灵, 沈洋, 等.持续腹腔热灌注化疗治疗进展期胆管癌的临床疗效观察[J].第二军医大学学报, 2017, 38(5):570. [13] SAVIER E, AZOULAY D, HUGUET E, et al.Percutaneous isolated hepatic perfusion for chemotherapy:a phase 1 study[J].Arch Surg, 2003, 138(3):325. doi: 10.1001/archsurg.138.3.325 [14] 黄伟, 刘会春, 王远鹏, 等.胆管癌病人腔内综合治疗与姑息性手术疗效比较[J].中华肝胆外科杂志, 2017, 23(6):289. [15] 范恒伟, 刘会春, 李宗狂, 等.经PTCD途径胆道金属支架置入术治疗恶性梗阻性黄疸137例临床疗效分析[J].肝胆外科杂志, 2013, 21(2):94. doi: 10.3969/j.issn.1006-4761.2013.02.005 [16] 王勇, 刘会春, 李宗狂, 等.经皮胆道支架联合125I粒子腔内植入治疗恶性梗阻性黄疸的初步研究[J].中华放射学杂志, 2014, 48(5):403. doi: 10.3760/cma.j.issn.1005-1201.2014.05.011 [17] World Medical Association.World Medical Association Declaration of Helsinki:ethical principles for medical research involving human subjects[J].JAMA, 2013, 310(20):2191. doi: 10.1001/jama.2013.281053 [18] LABIB PL, DAVIDSON BR, SHARMA RA, et al.Locoregional therapies in cholangiocarcinoma[J].Hepat Oncol, 2017, 4(4):99. doi: 10.2217/hep-2017-0014 [19] SQUADRONI M, TONDULLI L, GATTA G, et al.Cholangiocarcinoma[J].Crit Rev Oncol Hematol, 2017, 116:11. doi: 10.1016/j.critrevonc.2016.11.012 [20] 金浩, 刘会春, 李宗狂, 等.肝门胆管癌103例诊治分析[J].蚌埠医学院学报, 2013, 38(11):1402. [21] KOZAREK R.Role of preoperative palliation of jaundice in pancreatic cancer[J].J Hepatobiliary Pancreat Sci, 2013, 20(6):567. doi: 10.1007/s00534-013-0612-4 [22] HASIMU A, GU JP, JI WZ, et al.Comparative study of percutaneous transhepatic biliary stent placement with or without Iodine-125 seeds for treating patients with malignant biliary pbstruction[J].J Vasc Interv Radiol, 2017, 28(4):583. doi: 10.1016/j.jvir.2016.11.038 [23] 毛丽伟, 王阳, 廖国清, 等.腹腔热灌注化疗对晚期胃癌病人外周血和腹水调节性T细胞的影响及意义[J].检验医学与临床, 2016, 13(17):2429. doi: 10.3969/j.issn.1672-9455.2016.17.008 [24] 胡惠, 王宗鼎, 李可洲, 等.氟尿嘧啶联合丝裂霉素通过改变自噬作用抑制胆管癌细胞QBC939衰老并促进凋亡[J].第三军医大学学报, 2013, 35(18):1915. -

 点击查看大图
点击查看大图

图(1)表(3)
计量
- 文章访问数: 4035
- HTML全文浏览量: 2038
- PDF下载量: 13
- 被引次数: 0
