

-
骨性关节炎属于退行性疾病,包括年龄、劳损、肥胖、创伤、先天性关节异常、关节畸形等众多原因造成的软骨退化损伤以及软骨下骨、关节边缘反应性增生是其发病主要原因[1]。临床表现为进行性关节压痛、疼痛、僵硬、肿胀、功能受限以及关节畸形等,药物治疗虽然一定程度上能缓解疼痛及炎症反应,但大多数学者建议对于退变明显、疼痛严重以及明显关节活动受限的病人应进行手术治疗以达到根治目的[2]。全髋关节置换术(total hip arthroplasty,THA)是治疗骨性关节炎的主要方案,国内外众多临床报道均证实THA在治疗包括骨性关节炎、股骨颈骨折等疾病中具有优良疗效。但值得注意的是,THA虽然能使病人髋功能获得恢复,但术后并发症问题一直是影响THA预后的主要因素[3]。NEWMAN等[4]报道THA病人术后髋关节脱位发生率为4.65%~14.96%,术后髋关节早期脱位已成为THA较为常见的并发症,返修手术对病人造成经济负担及生理痛苦。因此,探寻术后脱位发生的危险因素,对采取针对性措施防治术后脱位具有十分重要的意义。本研究通过分析骨性关节炎THA病人的病历资料,探讨骨性关节炎THA术后脱位发生情况及危险因素,旨在提出针对性预防措施减少THA术后脱位,改善远期预后效果。现作报道。
-
选择2012年4月至2018年2月于我院治疗的266例骨性关节炎病人,均采用THA治疗,术后随访6个月,记录髋关节脱位发生情况,将术后髋关节脱位病人设为脱位组,未脱位病人设为未脱位组。纳入标准:(1)均符合中华医学会风湿病学分会《骨关节炎诊断及治疗指南》[5]诊断标准;(2)病人同意手术治疗;(3)均顺利完成THA,术后随访6个月;(4)病历资料保存完整;(5)年龄18~80岁,单侧手术。排除标准:(1)先天性下肢发育畸形者;(2)因外伤性骨折等需手术治疗;(3)随访期间遭受严重外伤。
-
THA:常规消毒、铺巾及全身麻醉,术前30 min静滴2.0 g头孢孟多酯钠预防感染。取侧卧位,髋关节后外侧或前外侧做弧形切口,长10~15 mm,逐层切开组织直至髂胫束筋膜显露,纵行切开并进行肌肉组织钝性分离,直至显露后方短外旋肌群,切开肌群,暴露后方髋关节关节囊并做“T”形切开,使关节腔显露。选择股骨小转子上方1.5 mm左右位置,采用摆动锯进行股骨头切除,进行股骨颈成型。髋关节附近滑膜、关节囊进行彻底清理。通过髋臼锉完成髋臼成型,去除髋臼软骨并将软骨下骨组织显露。以前倾20°、外展45°方向安放髋臼假体。随后通过股骨髓腔锉逐步完成股骨髓腔成型,股骨假体试模安放后进行复位,稳定性检查确定髋关节稳定性满意后将髋关节假体试模取出。采用0.9%氯化钠溶液、稀释聚维酮碘反复冲洗后再次安放髋关节假体。术中透视检查明确髋关节假体放置位置良好。再次冲洗后安置1根引流管,逐层缝合关闭切口。术后静脉给予头孢孟多酯钠进行抗感染治疗。髋关节脱位诊断标准[6]:髋关节明显活动性疼痛,关节运动受限,下肢缩短或异常外旋、内旋;经X线检查确诊。影响因素分析:记录2组病人性别、年龄、人工股骨头直径、髋关节手术史、手术入路、合并糖尿病、股骨假体前倾角、股骨偏心距、体质量指数(body mass index,BMI)、手术时间、术后输血率、术后引流量、手术失血量、手术侧别等,分析骨性关节炎THA术后脱位的独立危险因素。
-
采用t检验、χ2检验和logistic回归分析。
-
266例骨性关节炎病人THA术后脱位25例,脱位率9.40%,左侧14例(56.00%),右侧11例(44.00%)。
-
2组病人年龄、人工股骨头直径、髋关节手术史、手术失血量、术后股骨假体前倾角、术后股骨偏心距差异有统计学意义(P < 0.05~P < 0.01),而性别、BMI、手术入路、合并糖尿病、手术时间、术后输血率、术后引流量、手术侧别差异无统计学意义(P>0.05)(见表 1)。
项目 脱位组(n=25) 未脱位组(n=241) χ2 P 性别 男 10(40.00) 133(55.19) 2.10 >0.05 女 15(60.00) 108(44.81) 年龄/岁 ≤75>75 16(64.00)9(36.00) 288(78.01)53(21.99) 6.93 <0.01 人工股骨头直径/mm <30 12(48.00) 50(20.75) ≥30 13(52.00) 191(79.25) 9.41 <0.01 髋关节手术史 4(16.00) 12(4.98) 4.87 <0.05 手术入路 前外侧后外侧 7(28.00)18(72.00) 108(44.81)133(55.19) 2.61 >0.05 合并糖尿病 8(32.00) 40(16.60) 3.63 >0.05 BMI/(kg/m2) 22.45±1.87 22.87±1.90 1.05△ >0.05 手术时间/min 57.65±6.56 55.65±6.70 1.42△ >0.05 术后输血率 6(24.00) 54(22.41) 0.03 >0.05 术后引流量/mL 93.66±9.34 95.03±10.02 0.65△ >0.05 手术失血量/mL 323.82±32.77 309.76±29.02 2.28△ <0.05 手术侧别 左 14(56.00) 133(55.19) 0.01 >0.05 右 11(44.00) 108(44.81) 股骨假体前倾角(°) 9.54±1.32 7.96±0.98 7.40△ <0.01 术后股骨偏心距/mm 40.23±3.23 42.65±3.17 3.63△ <0.01 △示t值 表 1 骨性关节炎病人THA术后脱位单因素分析[n;百分率(%)]
-
多因素logistic回归分析结果显示,年龄>75岁、女性、人工股骨头直径<30 mm、髋关节手术史、后外侧入路、术后股骨假体前倾角>10°是骨性关节炎THA术后脱位的独立危险因素(P < 0.05)(见表 2)。
变量 β SE Wald P OR(95%CI) 年龄>75岁 0.834 0.265 8.667 <0.05 2.34(1.12~8.93) 女性 1.322 0.365 9.376 <0.05 2.90(1.41~9.03) 人工股骨头直径<30 mm 1.154 0.360 8.187 <0.05 2.70(1.14~989) 髋关节手术史 1.336 0.375 11.288 <0.05 3.57(1.49~12.32) 后外侧入路 0.956 0.297 7.518 <0.05 2.30(1.20~7.67) 术后股骨假体前倾角>10° 0.855 0.310 6.754 <0.05 2.12(1.27~7.18) 表 2 骨性关节炎病人THA术后脱位多因素分析
-
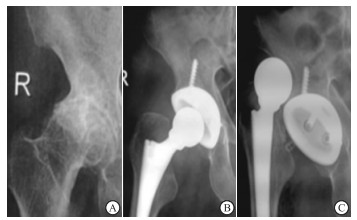
男性,77岁,图 1A正位X线片显示右髋臼发育不良、骨性关节炎;图 1B:接受后外侧入路THA治疗1周复查显示内固定良好;术后2月病人髋关节明显活动性疼痛,关节运动受限,下肢左侧外旋,图 1C正位X线显示髋关节脱位。

图 1 骨性关节炎THA术后髋关节脱位典型病例
-
THA在髋关节功能重建中广泛应用,其通过人造髋关节替换病损髋关节达到改善髋关节疼痛症状,恢复髋关节功能的目的,还能防止髋关节畸形出现或加重。THA适应症众多,股骨无菌性坏死、部分髋部骨折以及骨性关节炎等均可采用THA治疗[7]。但随着THA的临床应用,病人基数逐渐增大,术后并发症对手术预后的影响受到骨科医师的极大重视。术后髋关节脱位是THA最常见的并发症之一,需进行再次翻修手术,对病人髋关节功能恢复产生极大影响[8]。因此探寻术后脱位发生的危险因素,对采取针对性措施防治术后脱位具有十分重要的意义。
关于THA术后脱位发生率报道不一,罗肖等[9]报道GardenⅢ、Ⅳ股骨颈移位骨折病人THA术后脱位率9.72%,YOAHIMOTO等[10]报道THA术后脱位率7.67%,既往研究显示THA术后髋关节脱位发生率为4.65%~14.96%。本研究266例骨性关节炎病人THA术后脱位25例,脱位率9.40%,与既往研究结果一致。THA术后脱位原因众多,可归为3个方面,即自身原因、手术相关原因以及假体因素[11]。随着年龄的增加,髋关节周围软组织明显疏松,肌力显著降低,经THA治疗后出现手术区域及附近软组织张力失衡情况,关节稳定性下降,易造成术后髋关节脱位。TAKEGAMI等[12]报道称年龄>75岁病人THA术后早期脱位风险是≤75岁者的2.37倍,与本研究结果相一致。女性被作为OP的独立危险因素之一,其对THA术后脱位的影响主要与髋部骨质疏松有关[13]。雌激素对早期成骨细胞的分化具有促进作用,同时能刺激胶原蛋白合成。女性绝经后雌激素分泌降低,引起破骨细胞活性上升,骨密度下降,骨转化率增加,钙盐沉积受影响,促进骨消融,骨质大量丢失,骨关节骨脆性增加,稳定性下降,增加脱位风险。人工股骨头直径较大时能够提高关节活动度,降低假体摩擦、碰撞,髋关节及四周软组织获得更强的包容性,从而降低脱位风险[14]。YOSHIMOTO等[15]研究显示人工股骨头直径22 mm、28 mm是THA术后脱位危险因素,>30 mm是保护因素,与本研究结果相一致。髋关节手术史多与病人早期骨折有关,李志昌等[16]认为手术后外展肌力下降,肢体长度未完全恢复或者软组织张力降低等均会髋关节结构稳定性造成影响,再进行THA术时容易脱位。李文龙等[17]一项对比试验认为外侧入路手术操作简单、组织暴露清晰、不易造成臀中小肌损伤。但后外侧入路较前外侧入路对四块肌肉、关节韧带结构破坏较大,影响髋关节稳定性,导致术后关节保护较差,造成假体脱位。既往研究显示假体放置位置对THA术后脱位具有明显影响,集中在股骨假体前倾角、股骨偏心距等方面,本研究中术后股骨假体前倾角>10°是THA术后脱位的独立危险因素,与卢仲琳等[18]报道结果一致。其原因在于术后股骨前倾角度的增加会增加关节假体旋转扭曲,关节松动的风险增加,导致假体脱位。
本研究THA术后脱位发生情况及多因素分析显示,年龄>75岁、女性、人工股骨头直径<30 mm、髋关节手术史、后外侧入路、术后股骨假体前倾角>10°是THA术后脱位的独立危险因素,其临床意义在于术前能通过对术后脱位的高危病人采取针对性干预措施以降低脱位风险;同时具有手术相关危险因素者术后需增加随访及复查频率,密切关注手术效果。
综上所述,骨性关节炎THA术后容易发生髋关节脱位,年龄>75岁、女性、人工股骨头直径<30 mm、髋关节手术史、后外侧入路均可增加其脱位风险。本研究不足之处在于纳入病例数少,结果可能存在偏倚,需后期增加样本量进一步研究。
骨性关节炎全髋关节置换术术后脱位发生情况及其影响因素研究
Study on the occurrence of postoperative dislocation of total hip arthroplasty in patients with osteoarthritis, and its multivariate analysis
-
摘要:
目的研究骨性关节炎全髋关节置换术(total hip arthroplasty,THA)术后脱位发生情况及其危险因素分析。 方法选取266例骨性关节炎病人,均采用THA治疗,术后随访6个月,记录髋关节脱位发生情况,将术后髋关节脱位病人设为脱位组,未脱位病人设为未脱位组。记录2组病人手术相关指标及病历资料,经单因素分析、logistic回归分析探讨骨性关节炎THA术后脱位的独立危险因素。 结果266例骨性关节炎病人THA术后脱位25例,脱位率9.40%;2组病人年龄、人工股骨头直径、髋关节手术史、手术失血量、术后股骨假体前倾角、术后股骨偏心距差异有统计学意义(P < 0.05~P < 0.01),而性别、BMI、手术入路、合并糖尿病、手术时间、术后输血率、术后引流量、手术侧别差异无统计学意义(P>0.05)。多因素logistic回归分析显示,年龄>75岁、女性、人工股骨头直径 < 30 mm、髋关节手术史、后外侧入路、术后股骨假体前倾角>10°是骨性关节炎THA术后脱位的独立危险因素(P < 0.05)。 结论骨性关节炎THA术后容易发生髋关节脱位,年龄>75岁、女性、人工股骨头直径 < 30 mm、髋关节手术史、后外侧入路均可增加其脱位风险。 Abstract:ObjectiveTo study the occurrence and risk factors of dislocation after total hip arthroplasty(THA) for osteoarthritis. MethodsA total of 266 patients with osteoarthritis were treated with THA, and followed up for 6 months.The occurrence of dislocation of the hip joint was recorded.The patients with postoperative dislocation of the hip joint were set as the dislocation group, and the patients without dislocation were set as undislocation group.The surgical indicators and medical record in two groups were analyzed using univariate and logistic regression analysis to explore the independent risk factors of postoperative dislocation in patients treated with THA. ResultsAmong 266 patients with osteoarthritis, 25 cases with dislocation after THA were found, and the dislocation rate was 9.40%.The differences of the age, artificial femoral head diameter, history of hip surgery, postoperative blood loss, anterior angle of femoral prosthesis and postoperative femoral eccentricity between two groups were statistically significant(P < 0.05 to P < 0.01), and the differences of the gender, body mass index, surgical approach, combined diabetes mellitus, operative time, postoperative transfusion rate, postoperative drainage volume and operative side between two groups were not statistically significant(P>0.05).The results of multivariate logistic regression analysis showed that age >75 years, female, diameter of artificial femoral head < 30 mm, history of hip surgery, posterolateral approach and anteversion of femoral prosthesis >10° were the independent risk factors of dislocation after aosteoarthritis treated with THA(P < 0.05). ConclusionsThe hip joint with osteoarthritis is prone to dislocation after THA, the age >75 years, female, artificial femoral head diameter < 30 mm, hip surgery history and posterior lateral approach can increase the risk of dislocation. -
Key words:
- osteoarthritis /
- total hip arthroplasty /
- postoperative dislocation /
- risk factor
-
表 1 骨性关节炎病人THA术后脱位单因素分析[n;百分率(%)]
项目 脱位组(n=25) 未脱位组(n=241) χ2 P 性别 男 10(40.00) 133(55.19) 2.10 >0.05 女 15(60.00) 108(44.81) 年龄/岁 ≤75>75 16(64.00)9(36.00) 288(78.01)53(21.99) 6.93 <0.01 人工股骨头直径/mm <30 12(48.00) 50(20.75) ≥30 13(52.00) 191(79.25) 9.41 <0.01 髋关节手术史 4(16.00) 12(4.98) 4.87 <0.05 手术入路 前外侧后外侧 7(28.00)18(72.00) 108(44.81)133(55.19) 2.61 >0.05 合并糖尿病 8(32.00) 40(16.60) 3.63 >0.05 BMI/(kg/m2) 22.45±1.87 22.87±1.90 1.05△ >0.05 手术时间/min 57.65±6.56 55.65±6.70 1.42△ >0.05 术后输血率 6(24.00) 54(22.41) 0.03 >0.05 术后引流量/mL 93.66±9.34 95.03±10.02 0.65△ >0.05 手术失血量/mL 323.82±32.77 309.76±29.02 2.28△ <0.05 手术侧别 左 14(56.00) 133(55.19) 0.01 >0.05 右 11(44.00) 108(44.81) 股骨假体前倾角(°) 9.54±1.32 7.96±0.98 7.40△ <0.01 术后股骨偏心距/mm 40.23±3.23 42.65±3.17 3.63△ <0.01 △示t值  下载: 导出CSV
下载: 导出CSV
表 2 骨性关节炎病人THA术后脱位多因素分析
变量 β SE Wald P OR(95%CI) 年龄>75岁 0.834 0.265 8.667 <0.05 2.34(1.12~8.93) 女性 1.322 0.365 9.376 <0.05 2.90(1.41~9.03) 人工股骨头直径<30 mm 1.154 0.360 8.187 <0.05 2.70(1.14~989) 髋关节手术史 1.336 0.375 11.288 <0.05 3.57(1.49~12.32) 后外侧入路 0.956 0.297 7.518 <0.05 2.30(1.20~7.67) 术后股骨假体前倾角>10° 0.855 0.310 6.754 <0.05 2.12(1.27~7.18)
下载: 导出CSV
-
[1] 袁普卫, 康武林, 李小群, 等.骨性关节炎发病机制及相关细胞因子的研究进展[J].中国矫形外科杂志, 2016, 24(11):1010. [2] HOMMA Y, BABA T, SANO K, et al.Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty[J].Int Orthop, 2016, 40(8):1587. doi: 10.1007/s00264-015-2942-0 [3] KOBAYASHI H, HOMMA Y, BABA T, et al.Surgeons changing the approach for total hip arthroplasty from posterior to direct anterior with fluoroscopy should consider potential excessive cup anteversion and flexion implantation of the stem in their early experience[J].Int Orthop, 2016, 40(9):1813. doi: 10.1007/s00264-015-3059-1 [4] NEWMAN EA, HOLST DC, BRACEY DN, et al.Incidence of heterotopic ossification in direct anterior vs posterior approach to total hip arthroplasty:a retrospective radiographic review[J].Int Orthop, 2016, 40(9):1967. doi: 10.1007/s00264-015-3048-4 [5] 中华医学会风湿病学分会.骨关节炎诊断及治疗指南[J].中华风湿病学杂志, 2010, 14(6):416. doi: 10.3760/cma.j.issn.1007-7480.2010.06.024 [6] 贾金领, 侯文根, 张君, 等.髋关节置换术后发生脱位的危险因素分析[J].中国矫形外科杂志, 2016, 24(17):1624. [7] ARABNEJAD S, JOHNETON B, TANZER M, et al.Fully porous 3D printed titanium femoral stem to reduce stress-shielding following total hip arthroplasty[J].Orthop Res, 2017, 35(8):1774. doi: 10.1002/jor.23445 [8] YORK PJ, SMARCKC T, JUDET T, et al.Total hip arthroplasty via the anterior approach:tips and tricks for primary and revision surgery[J].Int Orthop, 2016, 40(10):2041. doi: 10.1007/s00264-016-3125-3 [9] 罗肖, 陈敬忠, 张怀学, 等.髋关节置换术后发生早期脱位的危险因素分析[J].局解手术学杂志, 2014, 23(1):46 [10] YOSHIMOTO K, NAKASHIMA Y, AOTA S, et al.Re-dislocation after revision total hip arthroplasty for recurrent dislocation:a multicentre study[J].Int Orthop, 2017, 41(2):1. [11] BUCKLAND AJ, PUVANESARAJAH V, VIGDORCHIK J, et al.Dislocation of a primary total hip arthroplasty is more common in patients with a lumbar spinal fusion[J].Bone Joint J, 2016, 16(10):S263. [12] TAKEGAMI Y, KOMATSU D, SEKI T, et al.Total hip arthroplasty after failed curved intertrochanteric varus osteotomy for avascular necrosis of the femoral head[J].Nagoya J Med Sci, 2016, 78(1):89. [13] 罗殿中, 张洪.一项基本的保髋手术技术:髋关节外科脱位技术[J].中华解剖与临床杂志, 2015, 20(5):475. doi: 10.3760/cma.j.issn.2095-7041.2015.05.025 [14] 董玉雷, 翁习生.全髋关节置换术后脱位的防治[J].中华解剖与临床杂志, 2014, 19(1):67. [15] YOSHIMOTO K, NAKASHIMA Y, YAMAMOTO T, et al.Dislocation and its recurrence after revision total hip arthroplasty[J].Int Orthop, 2016, 40(8):1625. doi: 10.1007/s00264-015-3020-3 [16] 李志昌, 李儒军, 柯岩, 等.人工髋关节置换术后股骨假体周围骨折的分型与治疗[J].中华骨科杂志, 2017, 37(15):952. doi: 10.3760/cma.j.issn.0253-2352.2017.15.008 [17] 李文龙, 范亚楠, 张蕾蕾, 等.微创全髋关节置换术直接前侧入路与外侧小切口入路的对比研究[J].中医正骨, 2016, 28(3):24. [18] 卢仲琳, 曹志强, 高国梁, 等.股骨假体颈干角、前倾角变化对全髋关节置换术后预后的影响[J].中国现代医学杂志, 2018, 28(11):68. [19] KIM MW, CHUNG YY, LEE JW, et al.Effect of femoral head size and surgical approach on risk of revision for dislocation after total hip arthroplasty[J].Acta Orthop Belg, 2017, 29(2):91. -

 点击查看大图
点击查看大图
图(1)表(2)
计量
- 文章访问数: 3624
- HTML全文浏览量: 2478
- PDF下载量: 8
- 被引次数: 0
