

-
血液透析是治疗慢性肾脏疾病终末期病人有效方式之一,而良好的血管通路将会大大提高血液透析病人的生活质量。动静脉内瘘是目前最理想的永久性血管通路,包括自体血管和人造血管内瘘[1]。而动静脉内瘘最常见的并发症就是血管狭窄,目前认为经皮经腔血管成型术(percutaneous transluminal angioplasty, PTA)是治疗动静脉内瘘狭窄的首选方式[2-3]。本研究选取我院动静脉内瘘吻合口近心端狭窄的病人,分别使用超声引导下PTA术和外科手术的方式治疗,并比较疗效是否一致。现作报道。
-
回顾性分析我院2016年1月至2018年9月收治的69例动静脉内瘘吻合口近心端狭窄的病人。所有病人内瘘吻合方式均为前臂桡动脉—头静脉端侧吻合。单一狭窄52例,多发狭窄17例。按手术方式分为A、B组, A组为彩超引导下行PTA术,B组为外科手术。A组36例,男21例,女15例,平均透析(4.11±3.06)年;B组33例,男22例,女11例,平均透析(3.85±2.81)年,2组病人一般资料差异无统计学意义(P>0.05)(见表 1)。本研究经过医院医学伦理委员会同意,所有病人都签署知情同意书。
分组 n 男 女 年龄/岁 透析
时间/年原发疾病 无 糖尿病肾病 慢性肾炎 其他疾病 A组 36 21 15 54.37±13.88 4.11±3.06 7 7 14 8 B组 33 11 22 52.38±15.53 3.85±2.81 6 6 12 9 χ2 — 0.51 0.56* 0.37* 0.24 P — >0.05 >0.05 >0.05 >0.05 *示t值 表 1 2组病人一般资料(x±s)
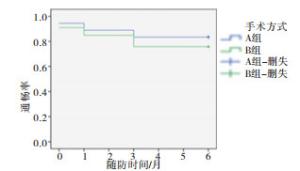
图 1 2组随访6个月的通畅率的生存曲线
-
针对血管狭窄超过周围正常血管管径50%伴有以下情况如:内瘘自然血流量<500 mL/min,不能满足透析时所需血流量;穿刺困难;透析充分性下降的病人进行入组。排除标准:因经皮动静脉瘘(AVF)建立时间短而无法进行透析者;AVF完全闭塞者; 因死亡失访;中心静脉狭窄导致肿胀手症者。术前常规使用彩超判断狭窄的部位、程度、狭窄的数量。根据病人意愿、医保因素、血管条件及合并基础疾病等情况分为2组。
-
术前及术后常规使用彩超测量狭窄部位血管内径、肱动脉血流量,测量3次取平均值。
-
术前超声明确狭窄部位后,选取距狭窄部位近心端3~10 cm左右为穿刺点,常规消毒铺巾后,探头戴无菌薄膜套,再次定位后,于局麻下穿刺针在穿刺点逆行穿刺动静脉内瘘的静脉端,置入5 F穿刺鞘,术者一手持导丝,一手持探头,沿穿刺鞘进入0.035超滑导丝,通过狭窄部位,沿导丝根据超声探查血管直径大小选择合适大小的球囊到达狭窄部位(球囊直径4~6 mm),逐渐增大压力至810.60~2 229.15 kPa,1 min后逐渐减压,2~3 min后重复上述操作,退出球囊,反复扩张2~3次,超声显示狭窄处血流明显好转,血管狭窄 < 30%,表明技术成功,退出球囊,无菌敷料包扎后,安返病房。
-
病人仰卧位,上肢外展,前臂常规消毒铺巾,前臂狭窄部位局部麻醉,作纵行切口长3~4 cm,钝性分离皮下组织,分别游离出头静脉、桡动脉,头静脉、桡动脉两端均用血管夹夹闭,沿两血管侧壁纵行切开约6~8 mm,头静脉近心端稀肝素盐水液压扩张,肝素、利多卡因冲洗血管,用6-0 prolene血管缝线,两血管行侧侧吻合,吻合结束,放开血管夹,见无渗血,可触及连续性震颤,阿米卡星局部冲洗后,缝合切口,术区消毒后无菌敷料包扎,安返病房。
-
术后彩超显示狭窄 < 30%, 表明技术成功。能够顺利完成一次血液透析表明临床成功[1]。
-
所有病人术后常规随访第1、3、6个月的通畅率。
-
采用t检验、χ2检验和生存分析。
-
A组彩超引导下行PTA术,临床成功率97%, 技术成功率100%。B组行外科手术,临床成功率94%, 技术成功率100%。
-
A组第1、3、6个月的通畅率与B组比较差异均无统计学意义(P>0.05)(见表 2)。术后6个月的通畅率生存曲线(见图 1)。并发症方面,A组中有1例因导丝不能通过狭窄部位放弃PTA,选择外科手术治疗;2例发生穿刺部位血肿,不作处理后自行吸收。B组2例出现术后渗血,予以止血后好转。2组并发症发生率差异无统计学意义(P>0.05)(见表 2)。
分组 n 通畅情况 并发症 1个月 3个月 6个月 A组 36 34(94.44) 32(88.89) 30(83.33) 3(8.33) B组 33 30(90.91) 28(84.85) 25(15.76) 2(6.06) χ2 — 0.32 0.25 0.61 0.13 P — >0.05 >0.05 >0.05 >0.05 表 2 2组通畅率、并发症的比较[n;百分率(%)]
-
术前及术后1个月的内瘘狭窄处血管内径与肱动脉血流量2组差异均无统计学意义(P>0.05),2组术后1个月的血管内径和血流量均明显大于术前(P < 0.01)(见表 3、4)。
分组 n 术前 术后1个月 t P A组 36 2.12±0.56 4.55±0.24 23.93 < 0.01 B组 33 1.98±0.72 4.95±0.31 21.76 < 0.01 t — 0.91 1.02 — — P — >0.05 >0.05 — — 表 3 2组病人术前与术后1个月血管内径的比较(x±s)
分组 n 术前 术后1个月 t P A组 36 472.21±75.32 654.65±71.22 10.31 < 0.01 B组 33 482.52±81.56 682.23±78.41 10.14 < 0.01 t — 0.55 1.53 — — P — >0.05 >0.05 — — 表 4 2组病人术前与术后1个月血流量比较(x±s)
-
良好的血管通路仍然是慢性血液透析病人的重中之重,动静脉内瘘是公认的首选血管通路形式[4],而血管通路的狭窄会导致透析不充分、穿刺点压力高等[5],是慢性肾功能衰竭尿毒症期病人反复住院的主要原因。
以前大多文献推荐采用外科手术重建内瘘治疗内瘘狭窄,而当前的文献多推荐PTA术治疗狭窄[2-4]。与外科手术相比,PTA术具有操作简便,降低感染发生率,可重复性强,保存病人的静脉血管等优势。本研究过程中,2组术后第1、3、6个月的通畅率差异无统计学意义, 术前与术后1个月相关彩超测量指标的比较差异无统计学意义, 表明两者疗效一致。国外的一项前瞻性研究表明,虽然外科手术与PTA术相比它的初次通畅率更高,但是在总体成功率上并没有统计学意义[6]。由此我们推荐PTA术作为治疗内瘘狭窄的首选方式。
行PTA治疗过程中,令人担忧的并发症是血管破裂。我们会在操作前评估血管条件,选择合适大小的球囊;操作时逐渐扩张球囊至完全打开,1min后减压,两次操作间隔2~3min。本次研究中无血管破裂发生,仅有2例发生穿刺部位血肿,不作处理后自行吸收。
在本次研究过程中A组3例病人应用普通球囊反复扩张3次后,残余狭窄仍>30%,更换Mustang高压球囊(压力>20atm)后,狭窄处血流明显好转。国内的一项前瞻性研究,分别采用高压球囊和普通球囊治疗内瘘狭窄,结果表明高压球囊组手术成功率及术后6个月的通畅率均高于普通球囊组[7]。对普通球囊扩张效果差的顽固狭窄,还可以使用切割球囊,国外的AFTAB等[8]的一项随机对照研究结果提示,切割球囊组的初次通畅率及二次通畅率比高压球囊组更高。
数字减影血管造影(digital subtraction angiography, DSA)是诊断血管狭窄的金标准,近年来超声对血管通路的检测逐渐替代DSA技术[9-10]。PTA术是在超声引导下实施的,首先,超声能够显示血管的三维结构,提高手术的安全性[11];其次,可以实时观察导丝及球囊在血管中的走行情况,球囊可精确定位在狭窄部位,也能够在球囊扩张过程中对其产生的并发症予以及时的处理(如血管破裂时可及时发现并予以扩张的球囊物理压迫,严重时可放血管支架等[12-13]);最后,它可及时观察手术疗效,判定手术是否成功,以及早期诊断内瘘的再次狭窄,故可广泛用于内瘘狭窄的筛查[14]。彩超引导下的球囊扩张术,与常规的DSA引导的PTA相比,它避免使用造影剂,医师和病人也不用受到辐射的影响;此外,它操作简便,一个受过超声培训的肾内科医师即可完成[15]。国外有报道4896例超声引导下血透通路腔内治疗的病例,其中内瘘狭窄的病人治疗成功率达到97.1%,内瘘闭塞的病人治疗成功率达到91.9%[13]。张树超等[16]对569例病人进行了1244例次超声引导下PTA术治疗血管通路狭窄,其技术成功率,临床成功率均达到98%。因此, 我们推荐彩超引导下的球囊扩张术作为治疗内瘘狭窄的首选方式。
本研究过程中也存在一些不足和遗憾。首先,超声对上肢浅表血管的评价较好,但我们也不能忽视对一些中心静脉的评估,如锁骨下静脉等,因其多位于骨骼及肺部组织附近,超声易受到影响,此时依赖于血管造影检查[17-18];其次,本研究采取的是回顾性分析,病例数只有69例,且所有病人均为动静脉内瘘吻合口近心端狭窄,缺乏对穿刺点狭窄、深静脉狭窄,供血动脉狭窄的进一步评估。而且随访时间太短。
彩超引导下球囊扩张在血管通路狭窄中的应用
Application value of balloon dilation guided by color doppler ultrasound in vascular access stenosis
-
摘要:
目的研究彩超引导下球囊扩张术与外科重建内瘘术在治疗动静脉内瘘吻合口近心端狭窄(距吻合口2 cm以内)时的疗效是否一致。 方法回顾性分析69例动静脉内瘘吻合口近心端狭窄病人,根据手术方式分为经皮腔内血管成形术(PTA)组(A组)36例,外科手术组(B组)33例。随访并比较2组第1、3、6个月的通畅率。 结果A组透析时间(4.11±3.06)年,临床成功率97%,技术成功率100%。B组透析时间(3.85±2.81)年,临床成功率94%,技术成功率100%。A组第1、3、6个月的通畅率高于B组(P>0.05)。术后2组并发症发生率差异无统计学意义(P>0.05)。术前及术后1个月的内瘘狭窄处血管内径与肱动脉血流量2组差异均无统计学意义(P>0.05),2组术后1个月的血管内径和血流量均明显大于术前(P < 0.01)。 结论彩超引导下球囊扩张术与外科手术治疗动静脉内瘘吻合口近心端狭窄具有相同的疗效,因为前者具有操作简便,术后即可透析,保存病人血管资源等优势可以推荐作为动静脉内瘘吻合口近心端狭窄首选的治疗方式。 Abstract:ObjectiveTo compare the efficacy between balloon dilatation guided by color ultrasound and surgical reconstruction in the treatment of hemodialysis autogenous fistula anastomotic proximal stenosis(within 2 cm from the anastomosis). MethodsThe clinical data of 69 patients with arteriovenous fistula anastomotic proximal stenosis were retrospectively analyzed.The patients were divided into the group A(36 cases treated with percutaneous transluminal angioplasty(PTA) and group B(33 cases treated with revascularization surgery).The patency rates in two groups at 1, 3 and 6 months of after treatment were evaluated. ResultsThe dialysis time, clinical success rate and technical success rate in group A were(4.11±3.06) years, 97% and 100%, respectively.The dialysis time, clinical success rate and technical success rate in group B were (3.85±2.81) years, 94% and 100%, respectively.The patency rates in A group at 1, 3 and 6 months after treatment were higher than that in group B(P < 0.05).There was no statistical significance in the incidence rate of complications between two groups(P>0.05).There was no statistical significance in the intravascular diameter of internal fistula stenosis and brachial artery blood flow between two groups before operation and after 1 month of operation(P>0.05).The blood vessel diameter and blood flow in two groups after operation were significantly greater than those before operation(P < 0.01). ConclusionsThe effects of balloon dilatation guided by color ultrasound and surgical reconstruction in the treatment of hemodialysis autogenous fistula anastomotic proximal stenosis are the same.The balloon dilatation guided by color ultrasound is simple, the patients can be dialysed after operation, the vascular resources can be preserved, so which can be recommended as the preferred treatment for arteriovenous fistula anastomotic proximal stenosis. -
表 1 2组病人一般资料(x±s)
分组 n 男 女 年龄/岁 透析
时间/年原发疾病 无 糖尿病肾病 慢性肾炎 其他疾病 A组 36 21 15 54.37±13.88 4.11±3.06 7 7 14 8 B组 33 11 22 52.38±15.53 3.85±2.81 6 6 12 9 χ2 — 0.51 0.56* 0.37* 0.24 P — >0.05 >0.05 >0.05 >0.05 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 2组通畅率、并发症的比较[n;百分率(%)]
分组 n 通畅情况 并发症 1个月 3个月 6个月 A组 36 34(94.44) 32(88.89) 30(83.33) 3(8.33) B组 33 30(90.91) 28(84.85) 25(15.76) 2(6.06) χ2 — 0.32 0.25 0.61 0.13 P — >0.05 >0.05 >0.05 >0.05
下载: 导出CSV
表 3 2组病人术前与术后1个月血管内径的比较(x±s)
分组 n 术前 术后1个月 t P A组 36 2.12±0.56 4.55±0.24 23.93 < 0.01 B组 33 1.98±0.72 4.95±0.31 21.76 < 0.01 t — 0.91 1.02 — — P — >0.05 >0.05 — —
下载: 导出CSV
表 4 2组病人术前与术后1个月血流量比较(x±s)
分组 n 术前 术后1个月 t P A组 36 472.21±75.32 654.65±71.22 10.31 < 0.01 B组 33 482.52±81.56 682.23±78.41 10.14 < 0.01 t — 0.55 1.53 — — P — >0.05 >0.05 — —
下载: 导出CSV
-
[1] 王玉柱, 叶朝阳, 金其庄.中国血液透析用血管通路专家共识[J].中国血液净化, 2014, 13(8):549. [2] FAN SS, CHEN CW, LU KC, et al.A comparison of efficacy of endovascular versus surgical repair for the treatment of arteriovenous fistula stenosis in Taiwan[J].J Vasc Access, 2017, 18(3):200. [3] PIROZZI N, SCRIVANO J, PIROZZI R, et al.Impaired maturation of arteriovenous fistula for haemodialysis due to forearm artery stenosis:percutaneous endovascular treatment[J].J Vasc Access, 2017, 18(6):503. [4] PATANÈ D, FAILLA G, CONIGLIO G, et al.Treatment of juxta-anastomotic stenoses for failing distal radiocephalic arteriovenous fistulas:Drug-coated balloons versus angioplasty[J].J Vasc Access, 2018, 20(2):1. [5] PIROZZI N, GARCIA-MEDINA J, HANOY M.Stenosis complicating vascular access for hemodialysis:indications for treatment[J].J Vasc Access, 2014, 15(2):76. [6] TESSITORE N, LIPARI G, POLI A, et al.Can blood flow surveillance and pre-emptive repair of subclinical stenosis prolong the useful life of arteriovenous fistulae-A randomized controlled study[J].Nephrol Dial Transplant, 2001, 19(9):2325. [7] 王耿, 陈志强, 李孝虎, 等.高压球囊对比普通球囊治疗自体动静脉内瘘狭窄疗效的前瞻性分析[J].中国血管外科杂志, 2016, 8(1):53. [8] AFTAB SA, TAY KH, IRANI FG, et al.Randomized clinical trial of cutting balloon angioplasty versus high-pressure balloon angioplasty in hemodialysis arteriovenous stenosis resistant to conventional balloon angioplasty[J].J Vasc Interv Radiol, 2014, 25(2):190. [9] DE GRAAFR, VAN LAANEN J, PEPPELENBOSCH N, et al.The value of intravascular ultrasound in the treatment of central venous obstructions in hemodialysis patients[J].J Vasc Access, 2016, 17(Suppl 1):S12. [10] DE GRAAFR.Endovascular treatment of swing-segment stenosis in vascular access:current and future directions[J].J Vasc Access, 2017, 18(Suppl 1):S74. [11] GALLAGHER J, BONISCAVAGE P, ASCHER P, et al.Clinical experience with office-based Duplex-guided balloon-assisted maturation of arteriovenous fistulas for hemodialysis[J].Ann Vasc Surg, 2012, 26(7):982. [12] GUEDES MARQUES M, IBEAS J, BOTELHO C, et al.Doppler ultrasound:a powerful tool for vascular access surveillance[J].Semi Dial, 2015, 28(2):206. [13] WAKABAYASHI M, HANADA S, NAKANO H, et al.Ultrasound-guided endovascular treatment for vascular access malfunction:results in 4896 cases[J].J Vasc Access, 2013, 14(3):225. [14] 王云燕, 黄龙, 付丽丽, 等.血管超声维护性筛查在早期诊断动静脉内瘘狭窄中的应用[J].中国血液净化, 2016, 15(12):697. [15] BEATHARD GA, LITCHFIELD T.Effectiveness and safety of dialysis vascular access procedures performed by interventional nephrologists[J].Kidney Int, 2004, 66(4):1622. [16] 张树超, 胡为民, 冯剑, 等.超声引导下腔内介入治疗内瘘血管狭窄[J].中国血液净化, 2016, 15(12):631. [17] 黄少敏, 岑忠耿, 张伟帅, 等.彩色多普勒超声评估透析病人动静脉内瘘血栓及狭窄的临床价值[J].中国超声医学杂志, 2016, 32(1):31. [18] 蔡晓峰, 王阿军, 查月琴, 等.超声在血液透析用动静脉内瘘并发症中的应用价值[J].中国血液流变学杂志, 2012, 22(2):357. -

 点击查看大图
点击查看大图

图(1)表(4)
计量
- 文章访问数: 4452
- HTML全文浏览量: 2431
- PDF下载量: 12
- 被引次数: 0
