




-
2019年12月以来, 湖北省武汉市陆续发现了新型冠状病毒肺炎病人, 随着疫情的发展, 我国其他地区及境外也相继发现了此类病例。2月11日, 世界卫生组织总干事谭德赛宣布, 新型冠状病毒感染的肺炎将正式被命名为“2019冠状病毒病(COVID-19)”。国家疾病预防控制中心宣布将COVID-19纳入国家“乙类”传染病, 采取“甲类”传染病防控措施[1]。近期, 有关COVID-19的基础、临床及流行病学研究不断报道[2-6]。在我国举全国之力采取积极有效的防控措施和广大医务人员的努力下, 疫情已基本得到控制, 但在境外, 特别是意大利、西班牙等国, 病例数仍在迅速增长, 且死亡率较高。我们在临床救治工作中发现部分普通型病人可以很短时间内向重型病人演变, 甚至演变为危重型, 给提高救治成功率带来很大困难。如何早期发现该部分病人将对提高诊治水平有很大价值。本文分析我院收治的24例普通型向重型演变COVID-19病人的临床资料, 并与同期41例普通型病人的临床资料作比较, 分析COVID-19病人普通型向重型演变的可能危险因素。
-
该研究已通过蚌埠医学院第一附属医院医学伦理委员会批准, 符合赫尔辛基宣言的原则。我院为安徽省省级COVID-19收治的定点医院, 为全省4家重症病人集中救治基地之一。所有病例均符合当时“新型冠状病毒感染的肺炎诊疗方案”COVID-19诊断标准(试行第六版)。(1)流行病学史:①发病前14 d内有武汉市及周边地区, 或其他有病例报告社区的旅行史或居住史; ②发病前14 d内与新型冠状病毒感染者(核酸检测阳性)有接触史; ③发病前14 d内曾接触过来自武汉市及周边地区, 或来自有病例报告社区的发热或有呼吸道症状的病人; ④聚集性发病。(2)临床表现:①发热和/或呼吸道症状; ②具有上述COVID-19影像学特征; ③发病早期白细胞总数正常或降低, 或淋巴细胞计数减少。有流行病学史中的任何1条, 符合临床表现中任意2条。无流行病学史的, 符合临床表现中的三条, 就可诊断为疑似病例。纳入标准(确诊病例):疑似病例, 具备以下病原学证据之一者, ①实时荧光RT-PCR检测新型冠状病毒核酸阳性; ②病毒基因测序, 与已知的新型冠状病毒高度同源。收集2020年1月至2020年2月20日在蚌埠医学院第一附属医院隔离病房收治的24例普通型向重型演变COVID-19病人(演变组)的临床资料, 分析临床特征、血液学检验、炎性指标、胸部CT影像学特征及抗病毒治疗, 并与同期41例普通型病人(普通型组)的临床资料作比较, 分析COVID-19病人普通型向重型演变的可能危险因素。
-
所有确诊病人入院时均根据当时“新型冠状病毒感染的肺炎诊疗方案”进行临床分型。(1)普通型:具有发热、呼吸道等症状, 影像学可见肺炎表现; (2)重型:符合下列任何一条, ①呼吸窘迫, 呼吸频率(RR)≥30次/分; ②静息状态下, 指氧饱和度≤93%;③动脉血氧分压(PaO2)/吸氧浓度(FiO2)≤300mmHg; ④肺部影像学显示24~48h内病灶明显进展>50%者按重型管理。
-
入院后第2天清晨取空腹静脉血送检验科检查血常规、血生化, 并应用酶联免疫吸附试验法检测血清炎症因子白细胞介素(IL)-6, 操作严格按照说明书进行。
-
采用t检验和χ2检验。
-
演变组在合并基础疾病和呼吸频率上与普通型组比较差异有统计学意义(P<0. 05), 但在性别、年龄和临床症状上2组病人差异均无统计学意义(P>0. 05)(见表 1)。
分组 n 男 女 年龄/岁 合并基础疾病 临床症状 主要体征/(次/分) < 40 40~50 51~60 ≥60 0~1种 ≥2种 发热 咳嗽/咳痰 胸闷气喘 其他 < 24 ≥24 演变组 24 15 9 1 4 12 7 13 11 21 8 3 0 16 8 普通型组 41 20 21 5 11 15 10 36 5 41 12 1 1 36 5 χ2 — 1.15 2.52 13.32 3.41 6.13 P — >0.05 >0.05 <0.05 >0.05 <0.05 表 1 2组病人临床特征比较(n)
-
对2组病人的入院后第2天血液学指标比较,演变组淋巴细胞计数和血浆白蛋白明显低于普通型组(P<0.01)。血糖和尿素演变组明显高于普通型组(P<0.01)。2组在白细胞计数、血小板计数及丙氨酸氨基转移酶差异均无统计学意义(P>0.05)(见表 2)。
分组 n 白细胞计数/
(×109/L)淋巴细胞计数/
(×109/L)血小板计数/
(×109/L)白蛋白/
(g/L)ALT/
(U/L)血糖/
(mmol/L)尿素/
(μmol/L)演变组 24 6.34±3.68 0.98±0.53 237.58±125.53 35.03±5.92 42.88±41.83 8.84±3.88 5.97±2.96 普通型组 41 6.42±3.53 1.56±0.55 257.68±84.12 40.01±3.85 36.73±34.71 6.51±1.86 3.74±1.31 t — 0.09 4.16 0.77 4.11 0.63 3.27 4.19 P — >0.05 <0.01 >0.05 <0.01 >0.05 <0.01 <0.01 表 2 2组病人的血液学指标比较(x±s)
-
演变组IL-6和CRP明显高于普通型组(P<0.01)(见表 3)。
分组 n IL-6/(pg/mL) CRP/(mg/L) 演变组 24 9.88±4.59 47.88±16.63 普通型组 41 6.69±4.23 28.35±14.91 t — 2.84 4.88 P — <0.01 <0.01 表 3 2组病人的炎性指标比较(x±s)
-
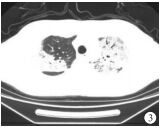
根据65例COVID-19病人的CT影像学表现,较为典型的征像有:(1)单发磨玻璃阴影;(2)多发外周胸膜下磨玻璃阴影;(3)双肺磨玻璃阴影、斑片状影及实变影同时存在;(4)双肺弥漫性磨玻璃阴影伴支气管充气征;(5)大面积实变影伴肺间质改变(见图 1~5)。2组病人的影像学表现差异有统计学意义(P<0.05)。虽然2组影像学表现中均为多发外周胸膜下磨玻璃阴影和双肺磨玻璃阴影、斑片状影及实变影同时存在为主,但演变组中以双肺磨玻璃阴影、斑片状影及实变影同时存在影像学表现比例最高,普通型组以多发外周胸膜下磨玻璃阴影比例最高(χ2=10.92, P<0.05)(见表 4)。

图 1 单发磨玻璃阴影
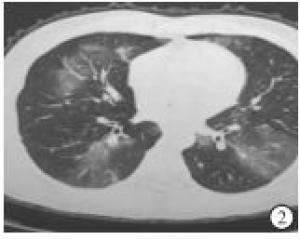
图 2 多发外周胸膜下磨玻璃阴影
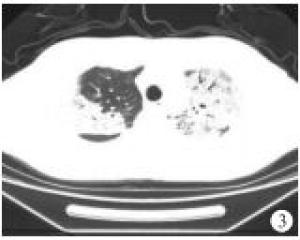
图 3 双肺磨玻璃阴影、斑片状影及实变影

图 4 双肺弥漫性磨玻璃阴影伴支气管充气征

图 5 大面积实变影伴肺间质改变
分组 n 单发磨
玻璃阴影多发外周胸膜下
磨玻璃阴影双肺磨玻璃阴影、
斑片状影及实变影双肺弥漫性磨玻璃
阴影伴支气管充气征大面积实变影
伴肺间质改变演变组 24 1(4.17) 3(12.50) 12(50.00) 7(29.16) 1(4.17) 普通型组 41 8(19.51) 17(41.46) 10(24.39) 6(14.64) 0(0.00) 合计 65 9(13.85) 20(30.77) 22(33.85) 13(20.00) 1(1.54) 表 4 2组病人的影像学表现比较[n;百分率(%)]
-
对于COVID-19临床抗病毒治疗,演变组2种抗病毒药物联合20例,3种药物联合4例,普通型组分别为35例、6例,2组差异无统计学意义(χ2=0.05,P>0.05),三种药物联合并没有减少向重型演变。
-
新型冠状病毒属于β属的冠状病毒,为多形性,直径为50~200 nm。S蛋白是病毒的主要蛋白之一,其编码基因可用于病毒分型;N蛋白包裹病毒基因组,可作为诊断抗原[7-8]。经过病毒序列比对分析,前期推测新型冠状病毒的自然宿主可能是蝙蝠等野生动物,在从蝙蝠到人的传染过程中也很可能存在未知的中间宿主媒介[9]。该病毒存在明确的人传人现象[10],因而采取“隔离”措施在控制传染源和传播途径上起巨大作用,中国的经验已证实了这一点。
临床工作中我们发现部分入院时分型为普通型病人可以很短时间内向重型演变,甚至为危重型,这给临床提高救治成功率带来很大困难。如何能对该部分病人早期发现将对提高诊治水平有很大价值。本研究分析我院收治的24例普通型向重型演变COVID-19病人的临床资料,并与同期41例普通型病人的临床资料作比较,结果显示演变组在合并基础疾病和呼吸频率上与普通型组比较差异有统计学意义(P<0.05),提示合并有2个及以上基础疾病和呼吸频率较快的病人更易向重型演变,这与GUO等[11]研究结果一致。合并基础疾病最多的是高血压病、糖尿病和冠心病等,可能是由于病人多为老年人,免疫力低下,因此对老年病人要高度重视。但进一步分析性别、年龄和临床症状与普通型向重型演变又无显著相关性(P>0.05),可能是病例数少的原因。对2组病人的入院后血液学指标比较,演变组在淋巴细胞计数和血浆白蛋白水平明显低于普通型组(P<0.01)。淋巴细胞计数降低提示可能存在免疫受损,白蛋白降低推测可能与病毒对肝细胞的直接损害造成的肝脏白蛋白合成障碍有关。有研究者[11]提出将淋巴细胞计数<0.8×109/L作为预测病毒性肺炎死亡风险模型的指标之一。同时在血糖和尿素上演变组明显高于普通型组(P<0.01)。血糖增高可能由于病人应激或本身合并糖尿病有关,尿素增高则可能与重型病人炎症反应更重及发热导致的高代谢相关。但2组的白细胞计数、血小板计数及丙氨酸氨基转移酶相比较差异则无统计学意义(P>0.05)。提示对于入院时淋巴细胞计数、白蛋白较低的普通型病人更易向重型演变,这与临床多数研究[12]结果一致,因此要更加重视。同时我们还观察到,每个病人对病毒产生的免疫应答是不一样的,具有很大的个体差异,由此产生的临床症状、疾病进展、对治疗药物的反应差异很大[13]。因此,我们对COVID-19的临床演变还应该考虑个体的炎症反应,寻找一些客观指标,帮助预测临床演变的准确性,以弥补不足。
众所周知,免疫功能可使机体获得防卫能力,抵抗外界感染,良好的免疫功能可帮助机体清除外来微生物,控制感染,使机体恢复健康。但是任何事物都有两面性,当病毒入侵人体时,如果免疫系统被过度激活或者失去控制,就会产生极端的免疫反应,释放大量细胞因子,反过来攻击宿主,这种现象被称之为“炎症风暴”。有研究[14]结果显示,细胞因子和趋化因子在重症感染病人体内明显升高,被认为可反映疾病严重程度。COVID-19病人的血清中IL-2R、IL-6等表达平均显著增高,且以危重型升高最明显,外周血IL-6可以作为独立预测COVID-19进程的关键因子。基于此我们推测以IL-6作为阻断靶点可能具有潜在的抑制炎症反应的临床价值。托珠单抗即人源性抗人IL-6受体单克隆抗体降低外周血IL-6活性达到阻断或减轻炎症反应的目的[15]。本研究通过检测病人血清中CRP和IL-6发现,演变组在IL-6和CRP水平明显高于普通型组,差异有统计学意义(P<0.01),也提示可能存在免疫受损。对于CRP、IL-6升高的普通型病人更易向重型演变。
COVID-19病人为了解肺部病变情况,我们建议做胸部HRCT,以减少误诊和漏诊。临床研究发现COVID-19在胸部CT上有特征性表现,我们分析65例COVID-19病人的CT影像学表现,较为典型的征像有单发磨玻璃阴影,多发外周胸膜下磨玻璃阴影,双肺磨玻璃阴影、斑片状影及实变影同时存在,双肺弥漫性磨玻璃阴影伴支气管充气征,两肺大面积实变影伴肺间质改变。2组病人的影像学表现比较差异有统计学意义(P<0.05)。特别强调的是,COVID-19病人胸腔积液或淋巴结肿大少见[8]。
对于抗病毒治疗,国家卫健委“新型冠状病毒感染的肺炎诊疗方案”中诊疗方案也不断调整,可试用α-干扰素、洛匹那韦/利托那韦、阿比多尔片、利巴韦林及磷酸氯喹等,疗程也在不断变化,不建议同时使用三种及以上抗病毒药物。本研究绝大部分病例,采用两种抗病毒药物,但在征求病人的同意下,少部分年轻病人选用三种抗病毒药物,但结果显示使用三种抗病毒药物治疗并没有减少普通型向重型演变(P>0.05),同时也没有缩短病毒转阴时间,部分病人还出现了不良反应。
本研究普通型向重型演变的24例病人中经积极治疗,大部分转为普通型,1例转为危重型,最后均痊愈出院。综上,在COVID-19病人普通型向重型演变的可能危险因素有:合并基础疾病、呼吸频率、淋巴细胞计数、血糖、白蛋白、尿素水平、炎症因子(CRP、IL-6)和影像学表现,临床工作中要特别注意,及早发现,早期处理,对提高救治率,降低死亡率将有非常大的意义。本研究病例数较少,以后可能要对该部分相关研究进行Meta分析,结果将更有说服力。
普通型向重型演变的新型冠状病毒肺炎病人的危险因素分析
Analysis of the risk factors of the common type evolving into severe type COVID-19
-
摘要:
目的 探讨新型冠状病毒肺炎(COVID-19)病人普通型向重型演变的临床危险因素。 方法 收集24例普通型向重型演变COVID-19病人的临床资料(演变组),分析临床特征、血液检验、炎性指标、胸部CT影像学特征及抗病毒治疗,并与同期41例普通型病人(普通型组)的临床资料进行比较,分析COVID-19病人普通型向重型演变的可能危险因素。 结果 临床特征,演变组在合并基础疾病和呼吸频率上与普通型组比较差异有统计学意义(P<0.05),但在性别、年龄和临床症状上2组病人差异无统计学意义(P>0.05)。血液学检验结果分析,演变组淋巴细胞计数和血浆白蛋白明显低于普通型组(P<0.05),演变组血糖和尿素明显高于普通型组(P<0.05)。但在白细胞计数、血小板计数及丙氨酸氨基转移酶差异均无统计学意义(P>0.05)。演变组炎性指标明显高于普通型组(P<0.05)。COCID-19普通型病人影像学表现为双肺磨玻璃阴影、斑片状影及实变影,双肺弥漫性磨玻璃阴影伴支气管充气征,两肺大面积实变影伴肺间质改变更易向重型演变,临床应重视。两种抗病毒药物联合和三种药物联合,在演变组和普通型组间差异无统计学意义(P>0.05)。 结论 COVID-19普通型向重型演变的可能危险因素有合并基础疾病、呼吸频率、淋巴细胞计数、血糖、白蛋白、尿素水平、炎症因子和影像学表现。 Abstract:Objective To investigate the clinical risk factors of common type evolving into severe type corona virus disease 2019 (COVID-19). Methods The clinical data of 24 patients with common type evolving into severe type COVID-19 were collected(evolution group), the clinical characteristics, blood test results, inflammatory indexes, chest CT imaging characteristics and antiviral treatment were analyzed, which was compared with the clinical data of 41 patients with common type COVID-19 patients(common type group).The possible risk factors of COVID-19 patients developing from common type to severe type were analyzed. Results For the clinical characteristics between evolution group and common type group, the differences of the complication with underlying disease and respiratory rate were statistically significant(P<0.05), and the differences of the sex, age and clinical symptoms were not statistically significant(P>0.05).The results of blood test showed that the lymphocyte counts and plasma albumin level in evolution group were significantly lower than those in common type group(P<0.05), the blood glucose and urea levels in evolution group were significantly higher than those in common type group(P<0.05), and the differences of the white blood cell count, platelet count and alanine aminotransferase levels between two groups were not statistically significant(P>0.05).The inflammatory indexes in evolution group were significantly higher than that in common type group(P<0.05).The double lung ground glass shadow, patchy shadow and consolidation shadow, double lung with diffuse ground glass shadow complicated with bronchogram were the mainly imaging findings of the common type group, and the common type patients with two lung large area consolidation shadow complicated with pulmonary interstitial change were more likely to develop to severe type.The differences of the clinical effects of two and three kinds of drugs treatment between two groups were not statistically significant(P>0.05). Conclusions The combination of underlying diseases, respiratory frequency, lymphocyte count, blood glucose, albumin, urea level, inflammatory factors and imaging manifestations are the possible risk factors of common type evolving into severe type COVID-19. -
Key words:
- corona virus disease 2019 /
- common type /
- severe type /
- risk factor
-
表 1 2组病人临床特征比较(n)
分组 n 男 女 年龄/岁 合并基础疾病 临床症状 主要体征/(次/分) < 40 40~50 51~60 ≥60 0~1种 ≥2种 发热 咳嗽/咳痰 胸闷气喘 其他 < 24 ≥24 演变组 24 15 9 1 4 12 7 13 11 21 8 3 0 16 8 普通型组 41 20 21 5 11 15 10 36 5 41 12 1 1 36 5 χ2 — 1.15 2.52 13.32 3.41 6.13 P — >0.05 >0.05 <0.05 >0.05 <0.05  下载: 导出CSV
下载: 导出CSV
表 2 2组病人的血液学指标比较(x±s)
分组 n 白细胞计数/
(×109/L)淋巴细胞计数/
(×109/L)血小板计数/
(×109/L)白蛋白/
(g/L)ALT/
(U/L)血糖/
(mmol/L)尿素/
(μmol/L)演变组 24 6.34±3.68 0.98±0.53 237.58±125.53 35.03±5.92 42.88±41.83 8.84±3.88 5.97±2.96 普通型组 41 6.42±3.53 1.56±0.55 257.68±84.12 40.01±3.85 36.73±34.71 6.51±1.86 3.74±1.31 t — 0.09 4.16 0.77 4.11 0.63 3.27 4.19 P — >0.05 <0.01 >0.05 <0.01 >0.05 <0.01 <0.01
下载: 导出CSV
表 3 2组病人的炎性指标比较(x±s)
分组 n IL-6/(pg/mL) CRP/(mg/L) 演变组 24 9.88±4.59 47.88±16.63 普通型组 41 6.69±4.23 28.35±14.91 t — 2.84 4.88 P — <0.01 <0.01
下载: 导出CSV
表 4 2组病人的影像学表现比较[n;百分率(%)]
分组 n 单发磨
玻璃阴影多发外周胸膜下
磨玻璃阴影双肺磨玻璃阴影、
斑片状影及实变影双肺弥漫性磨玻璃
阴影伴支气管充气征大面积实变影
伴肺间质改变演变组 24 1(4.17) 3(12.50) 12(50.00) 7(29.16) 1(4.17) 普通型组 41 8(19.51) 17(41.46) 10(24.39) 6(14.64) 0(0.00) 合计 65 9(13.85) 20(30.77) 22(33.85) 13(20.00) 1(1.54)
下载: 导出CSV
-
[1] 中华人民共和国国家卫生健康委员会.新型冠状病毒感染的肺炎诊疗方案[EB/OL]. [2] HUANG C, WANG Y, LI X, et al.Clinicalfeatures of patients infected with 2019 novel coronavirus in Wuhan, China[J].Lancet, 2020, 395(10223):497. doi: 10.1016/S0140-6736(20)30183-5 [3] WANG D, HU B, HU C, et al.Clinical characteristics of 138 hospitalized patients with 2019 Novel Coronavirus-infected pneumonia in Wuhan, China[J].JAMA, 2020.DOI:10.1001/jama.2020.1585. [4] CHAN JF, YUAN S, KOK KH, et al.A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission:a study of a family cluster[J].Lancet, 2020, 395(10223):514. doi: 10.1016/S0140-6736(20)30154-9 [5] REN LL, WANG YM, WU ZQ, et al.Identification of a novel coronavirus causing severe pneumonia in human:a descriptive study[J].Chinese Med J, 2020.DOI:10.1097/CM9.0000000000000722. [6] CHEN Y, LIU Q, GUO D, et al.Emerging coronaviruses:Genome structure, replication, and pathogenesis[J].J Med Virol, 2020, 92(4):418. doi: 10.1002/jmv.25681 [7] GRALINSKI LE, MENACHERY VD.Return of the Coronavirus:2019-nCoV[J].Viruses, 202012(2).DOI:10.3390/v12020135. [8] 华中科技大学同济医学院附属同济医院救治医疗专家组.新型冠状病毒感染的肺炎诊疗快速指南(第三版)(EB/OL).https://www.tjh.com.cn/html/2020/0128/28713.shtml#title.[2020-1-28]. [9] BENVENUTO D, GIOVANNETTI M, CICCOZZI A, et al.The 2019-new coronavirus epidemic:evidence for virus evolution[J].J Med Virol, 2020.DOI:10.1002/jmv.25688. [10] LI Q, GUAN X, WU P, et al.Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia[J].N Engl J Med, 2020.DOI:10.1056/NEJMoa2001316. [11] GUO L, WEI D, ZHANG X, et al.Clinical features predicting mortality risk in patients with viral pneumonia:the MuLBSTA score[J].Front Microbiol, 2019, 10:2752. doi: 10.3389/fmicb.2019.02752 [12] 陈蕾, 刘辉国, 刘威, 等.2019新型冠状病毒肺炎29例临床特征分析[J].中华结核和呼吸杂志, 2020, 43(3):203. doi: 10.3760/cma.j.issn.1001-0939.2020.03.013 [13] CASTRUCCI MR.Factors affecting immune responses to the influenza vaccine[J].Hum Vaccin Immunother, 2018, 14(3):637. [14] LA GRUTA NL, KEDZIERSKA K, STAMBAS J, et al.A question of self-preservation:immunopathology in influenza virus infection[J].Immunol Cell Biol, 2007, 85(2):85. doi: 10.1038/sj.icb.7100026 [15] YANG PH, ING YB, XU Z et al.Epidemiological and clinical features of COVID-19 patients with and without pneumonia in Beijing, China[J].Medrxiv, 2020.DOI:10.1101/2020.02.28.20028068 -
 20200401.pdf
20200401.pdf
-

 点击查看大图
点击查看大图

图(5)表(4)
计量
- 文章访问数: 4859
- HTML全文浏览量: 2662
- PDF下载量: 49
- 被引次数: 0
