

-
自2019年12月,新型冠状病毒肺炎自湖北省武汉市爆发,随后很快蔓延至全国各省,严重危害了人民的健康,极大影响了人民的生活和社会的安定。其病原体是一种先前未在人类体内发现的新型冠状病毒(SARS-CoV-2),世界卫生组织于2020年2月11日将其命名为COVID-19(Corona Virus Disease 2019)。COVID-19初期主要表现为发热、干咳、乏力,进而出现呼吸困难,严重者可进展为急性呼吸窘迫综合征或脓毒性休克,甚至死亡[1]。截至2020年3月10日,全国累计确诊病例80 967例(其中湖北省67773例),死亡3 162例(其中湖北省3 046例)。安徽省累计确诊990例,死亡6例[2]。蚌埠医学院第一附属医院作为安徽省COVID-19定点收治医院,同时为安徽省重症及危重症定点救治基地之一,承担着蚌埠市及周边城市重症及危重症COVID-19病人的救治。本研究旨在分析COVID-19的临床特征,尤其是普通型及(危)重型病人临床特性的对比分析,期望能够给广大医务工作者提供经验和依据,及早发现(危)重症倾向的病人,及早提供干预。
-
2020年1月22日至2020年3月4日,蚌埠医学院第一附属医院共收治74例COVID-19确诊病人。在充分保障病人隐私的情况下,本研究收集和使用了病人相关信息。
-
根据国家卫生健康委员会颁布的《新型冠状病毒肺炎诊疗方案(试行第七版)》中,COVID-19的诊断标准[3],所有病例符合疑似病例的标准,同时咽拭子和/或下呼吸道分泌物等标本实时荧光RT-PCR检测SARS-CoV-2核酸阳性。
-
所有病人入院后详细询问既往病史、流行病学病史、临床症状等,记录入院时体征,详细记录实验室检查,包括:血常规、肝肾功能、降钙素原(PCT)、C反应蛋白(CRP)、白细胞介素6(IL-6)、肌酸激酶等指标。所有病人入院均行胸部高分辨率CT(HRCT)。对比分析普通型及(危)重型病人的临床特性结果。
-
采用t(或t′)检验、χ2检验、Fisher′s确切概率法和秩和检验。
-
74例病人中普通型35例(47.3%),重症型36例(48.6%),危重型3例(4.1%);年龄21~83岁,平均年龄(56.11±12.66)岁,其中普通型(51.63±10.97)岁, (危)重型(57.90±11.98)岁;男41例(55.4%),女33例(44.6%),男女比例1.24: 1;在基础疾病方面,44.6%的病人合并其他基础性疾病,14.9%的病人合并2种及2种以上的基础疾病,25.7%的(危)重型病人合并2种及2种以上基础疾病;(危)重型病人的年龄、合并其他基础性疾病率以及合并2种及2种以上基础疾病率均高于普通型病人(P < 0.05~P < 0.01)。在所合并的基础疾病中,高血压占24.3%,最为常见,其次为2型糖尿病(17.6%),其他还包括冠心病(4.1%)、脑梗死(5.4%)、慢性阻塞性肺疾病(COPD)(2.7%)等。其中蚌埠地区病人中,有武汉及其他疫区接触史16例(21.6%),聚集性发病37例(50.0%),其中家族聚集性发病36例(48.6%),1例(1.4%)为蚌埠元素健身房聚集感染,家族聚集性发病的病例一共涉及蚌埠市全部22起聚集性发病中的12个家庭(族),其中1户发生9例病例,1户发生6例,4户发生3例,5户发生2例。37例聚集性病例中普通型20例,(危)重型17例(见表 1)。
项目 普通型
(n=35)(危)重型
(n=39)合计
(n=74)χ2 P 年龄(x±s)/岁 51.63±10.97 57.90±11.98 54.93±11.78 2.34* < 0.05 性别 男 20(57.1) 21(53.8) 41(55.4) 0.08 > 0.05 女 15(42.9) 18(46.2) 33(44.6) 武汉及其他疫区接触史 9(25.7) 9(23.1) 18(24.3) 0.07 > 0.05 聚集性病例 20(57.1) 17(43.6) 37(50.0) 1.36 > 0.05 基础疾病 12(34.3) 23(59.0) 33(44.6) 4.51 < 0.05 高血压 4(11.4) 14(35.9) 18(24.3) — — 2型糖尿病 3(8.6) 10(25.6) 13(17.6) — — 冠心病 1(2.9) 2(5.1) 3(4.1) — — 脑梗死 1(2.9) 3(7.7) 4(5.4) — — 肾脏疾病 0(0.0) 2(5.1) 2(2.7) — — 支气管扩张 0(0.0) 1(2.6) 1(1.4) — — COPD 1(2.9) 1(2.6) 2(2.7) — — 甲状腺炎 0(0.0) 1(2.6) 1(1.4) — — 痛风 1(2.9) 1(2.6) 2(2.7) — — 房颤 1(2.9) 0(0.0) 1(1.4) — — 心肌缺血 1(2.9) 0(0.0) 1(1.4) — — 乙肝 1(2.9) 0(0.0) 1(1.4) — — 髂软骨瘤 0(0.0) 1(2.6) 1(1.4) — — 合并2种或2种以上基础病 1(2.9) 10(25.7) 11(14.9) 7.57 < 0.01 *示t值 表 1 一般资料的比较[n;百分率(%)]
-
临床表现方面,(危)重型病人发病至就诊的时间较普通型病人长,最高体温、胸闷发生率、呼吸困难发生率较普通型病人高(P < 0.05~P < 0.01);观察其临床症状,病人普遍出现发热(98.6%),37~37.9℃、38~38.9℃、≥39℃三个体温范围所占比例分别为15例(20.3%)、36例(48.6%)、22例(29.7%),普通型病人中分别为8例(22.9%)、21例(60.0%)、6例(17.1%),(危)重病人中分别为7例(17.9%)、15例(38.5%)、16例(41.0%);大部分病人出现咳嗽(70.3%),而咳痰仅占31.1%,说明以干咳多见;另外,胸闷(52.7%)、呼吸困难(10.8%)、腹泻(13.5%)也是COVID-19病人常见的症状,偶见纳差(4.1%)、恶心呕吐(1.1%)(见表 2)。
项目 普通型
(n=35)(危)重型
(n=39)合计
(n=74)χ2 P 发病到就诊时间/d 4.00(3.00~7.00) 7.00(3.00~9.00) 6.00(3.00-8.00) 2.01* < 0.05 临床症状 发热 35(100.0) 38(97.4) 73(98.6) — > 0.05 # 最高体温(x±s)/℃ 38.24±0.56 38.58±0.73 38.42±0.67 2.23△ < 0.05 37~37.9 8(22.9) 7(17.9) 15(20.3) — — 38~38.9 21(60.0) 15(38.5) 36(48.6) — — ≥39 6(17.1) 16(41.0) 22(29.7) — — 咳嗽 21(60.0) 31(79.5) 52(70.3) 3.35 > 0.05 咳痰 10(28.6) 13(33.3) 23(31.1) 0.20 > 0.05 胸闷 8(22.9) 31(79.5) 39(52.7) 23.73 < 0.01 呼吸困难 0(0.0) 8(20.5) 8(10.8) 6.06 < 0.01 腹泻 2(5.7) 8(20.5) 10(13.5) 3.46 > 0.05 纳差 2(5.7) 1(2.6) 3(4.1) 0.47 > 0.05 恶心呕吐 0(0.0) 1(2.6) 1(1.4) — > 0.05# *示zc值; #示Fisher′s确切概率法; △示t值 表 2 临床表现的比较[n;百分率(%)]
-
从COVID-19病人入院时各项实验室检查中可以看出,血常规中,分别有7例(9.5%)、10例(13.5%)和18例(24.3%)白细胞、中性粒细胞绝对值和中性粒细胞百分比升高;40例(54.1%)、32例(43.2%)和9例(12.2%)淋巴细胞绝对值、淋巴细胞百分比和血小板下降。肝肾功能及其他各项检查中,有46例(62.2%)、36例(48.6%)和14例(19.0%)CRP、IL-6和丙氨酸氨基转移酶(ALT)升高,55例(74.3%)白蛋白下降。(危)重型和普通型相比较,白细胞、中性粒细胞绝对值、中性粒细胞百分比、CRP以及IL-6较高,淋巴细胞绝对值、淋巴细胞百分比和白蛋白较低(P < 0.05~P < 0.01)。而血小板、ALT、PCT、肌酸激酶等差异无统计学意义(P>0.05)(见表 3)。
项目 普通型(n=35) (危)重型(n=39) zc P 白细胞(x±s)/(×109/L) 5.03±1.47 6.52±2.98 2.77* < 0.01 中性粒细胞绝对值/(×109) 3.35(2.30, 4.17) 4.11(2.86, 6.41) 2.34 < 0.05 中性粒细胞百分比/% 64.70(59.70, 72.30) 64.70(59.70, 72.30) 3.33 < 0.01 淋巴细胞绝对值/(×109) 1.21(0.80, 1.61) 0.72(0.6, 1.5) 2.25 < 0.05 淋巴细胞百分比/% 25.50(17.70, 29.70) 16.60(10.95, 23.93) 2.99 < 0.01 血小板/(×109) 170.00(137.00, 284.00) 233.00(141.5, 303.00) 0.92 > 0.05 ALT/(U/L) 20.00(13.00, 40.00) 33.50(13.00, 51.25) 0.99 > 0.05 PCT/(ng/mL) 0.10(0.10, 0.15) 0.11(0.10, 0.19) 0.70 > 0.05 IL-6/(pg/mL) 2.32(1.50.9.17) 8.50(2.54, 21.96) 2.74 < 0.01 CRP/(mg/L) 7.80(3.70, 34.90) 26.70(4.90, 74.10) 2.11 < 0.05 肌酸激酶/(U/L) 57.00(40.00, 75.00) 40.00(29.00, 65.00) 1.79 > 0.05 白蛋白(x±s)/(g/L) 39.70±4.28 35.94±4.43 3.70# < 0.01 *示t′值; #示t值 表 3 入院时实验室检查的比较[P50(P25, P75)]
-
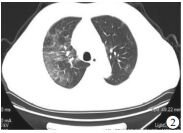
74例病人在入院时均行胸部HRCT检查,73例(98.6%)出现典型病灶,普通型34例(97.1%),(危)重型39例(100.0%),2组病人之间差异无统计学意义(P>0.05)。病人CT表现为多发斑片状磨玻璃密度影,部分出现支气管充气征、实变影等,多见于肺外缘近胸膜处,(危)重症可出现病灶快速进展,胸腔积液少见。典型病例胸部HRCT检查结果见图 1~2。
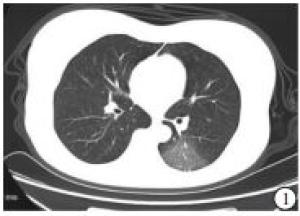
图 1 女性,30岁,诊断为NCP普通型

图 2 男性,51岁,诊断为NCP重型
-
据流行病学调查[3]发现,COVID-19具有明显的传染性,经呼吸道飞沫和密切接触传播是主要传播途径,人群普遍易感。CHAN等[4]通过对一个旅居武汉的家庭6人聚集性发病的流行病学调查,证实了SARS-CoV-2可在家庭环境中发生人际传播。在本研究中,我院收治的蚌埠地区74例病人以聚集性发病,尤其是家族聚集性发病多见,原因可能与春节期间聚餐、聚会有关,也与密闭空间(如家中、健身房、餐厅等)内疾病传染概率可能增加有关,这也侧面证明了无症状携带者传播COVID-19的风险,对于疾病的预防具有很大挑战。另外,聚集性发病病人中普通型与(危)重型所占的比例无明显差异。在病人基础资料中,我们发现,(危)重症病人的年龄更大,合并的基础疾病更多,合并2种及2种以上基础病的病人例数明显高于普通型组,这与目前已有的研究[5]相似,结果意味着,年龄大、基础病多的病人更易发展为(危)重症;在统计的基础疾病中,高血压、2型糖尿病、心脑血管疾病占据较高的比例,提示这些疾病可能是(危)重病人的危险因素。另外,从本研究结果看,性别差异在易感因素及(危)重症的危险因素中差异不大。
一些研究[6-8]显示, COVID-19病人多以发热、干咳、肌肉酸痛等为主要临床表现。从本研究中的临床特征来看,发热(98.6%)、咳嗽(70.3%)仍为主要临床表现,数据分析表明,普通型组体温多集中在38~38.5℃,很少超过39℃,而(危)重型组的体温较普通型组高,近半数超过39℃,说明高热也是COVID-19病人重症的危险因素之一。大部分病人出现咳嗽,但咳痰比例不高,佐证了COVID-19的临床特征以干咳为主,而(危)重症病人更多出现胸闷、呼吸困难等表现。腹泻、纳差及恶心呕吐等胃肠道症状发生率不高,是与COVID-19直接相关,还是与炎症反应、饮食、环境等其他因素有关还需进一步取证研究。值得提出的是,(危)重症病人发病到确诊的时间长于普通型病人,提示疑似病例的早发现、早诊断、早治疗在疾病的转归上有很大的影响,一定程度上避免因为诊疗延迟而导致疾病重症化的可能,给疾病防控提出了一些启发。
在实验室检查中,我们发现,对于COVID-19的病人,普遍存在淋巴细胞绝对值和百分比下降、CRP升高等特点,而ALT、肌酸激酶等指标异常的例数不多,肝脏、心肌损害的程度不够明显,但在一些其他地区的研究[9-10]中提示COVID-19对于肝脏、心肌、凝血功能可能有一定程度的损伤,那么COVID-19是否除了肺以外还对其他脏器,如肝脏、肾脏、心肌、血液系统等产生全面损伤,还需收集更多的样本病例进行进一步的分析。普通型与(危)重型相比较发现,(危)重型病人中白细胞、中性粒细胞绝对值、中性粒细胞百分比、CRP及IL-6较普通组明显升高,可能与细胞免疫受损、细胞炎症因子风暴等因素有关,而在入院时的实验室检查中,(危)重组淋巴细胞绝对值、淋巴细胞百分比及白蛋白较普通组明显下降,提示在COVID-19的治疗中需动态观察如上指标,警惕疾病的重症化倾向。
影像学方面,普通组和(危)重组无明显特殊差异,除普通型1例未表现明显病灶外,其他病人均出现斑片状磨玻璃影的典型病灶,多位于肺外侧带近胸膜处[11],(危)重症病人肺部病灶进展快,范围大,容易出现支气管充气征、实变、纤维化等改变。可见COVID-19在早期即可对肺部造成病理性损害,肺部影像学检查对于早期COVID-19的诊断有很大的帮助。
综上,COVID-19是一种新发传染病,还有很多方面需要进一步探讨,本文通过回顾性研究分析了COVID-19一些特征性的临床特性,比较普通型及(危)重型病人在基本背景、一般资料、临床症状、实验室检查等方面的差异,期望能早期识别危险因素,提早干预,从而阻止疾病重症化发展。
新型冠状病毒肺炎74例临床特性分析
Analysis of the clinical characteristics of 74 cases with Corona Virus Disease 2019
-
摘要:
目的 对新型冠状病毒肺炎确诊病人的临床特性进行分析并总结。 方法 回顾性分析蚌埠医学院第一附属医院2020年1月22日至3月4日收治的74例新型冠状病毒肺炎的临床特性,重点对比普通型及(危)重型病人临床特性的区别。 结果 74例病人中普通型35例,重型及危重型39例;家族聚集性发病的病人较多(37例,50.0%);一般资料方面,(危)重型病人的年龄、合并其他基础性疾病率以及合并2种及2种以上基础疾病率均高于普通型病人(P < 0.05~P < 0.01);临床症状方面,(危)重型病人发病至就诊的时间较普通型长,最高体温、胸闷发生率、呼吸困难发生率较普通型高(P < 0.05~P < 0.01);实验室检查方面,(危)重型和普通型相比较,白细胞、中性粒细胞绝对值、中性粒细胞百分比、C反应蛋白以及白细胞介素-6较高,而淋巴细胞绝对值、淋巴细胞百分比和白蛋白较低(P < 0.05~P < 0.01);胸部高分辨率CT检查均出现斑片状磨玻璃影。 结论 蚌埠地区病人聚集性病例较多;(危)重症病人以年龄偏大、合并基础病多、全身炎症反应大为特点。 Abstract:Objective To analyze the clinical characteristics of 74 patients with corona virus disease 2019(COVID-19). Methods The clinical characteristics of 74 pateints with COVID-19 from January 22 to March 4, 2020 from the First Affiliated Hospital of Bengbu Medical College were retrospectively analyzed, and the clinical characteristics were compared between common type and severe type patients. Results Among 74 patients, 35 cases were the common type, and 39 cases were severe/critical type cases.There were high number of familial cluster(37 cases, 50.0%).The age, and rates of complicated with other basic diseases and complicated with two or more basic diseases in severe/critical patients were higher than those in common patients(P < 0.05 to P < 0.01).In terms of clinical symptoms, the time from onset to see doctor in severe/critical patients was longer than that in common patients, and the highest body temperature, incidence rates of chest tightness and dyspnea in severe/critical patients were higher than those in common patients(P < 0.05 to P < 0.01).In terms of laboratory examination, the absolute value of leucocyte and neutrophil, percentage of neutrophil, C-reactive protein and interleukin-6 in severe/critical patients were higher compared with those in common patients, and the absolute value of lymphocyte, percentage of lymphocyte and albumin in severe/critical patients were lower compared with those in common patients(P < 0.05 to P < 0.01).The patchy ground glass opacity in chest CT of all cases were found. Conclusions The number of familial clustering cases of COVID-19 in Bengbu city is more, and the elderly complicated with more basic diseases and systemic inflammatory response are the clinical characteristics of severe/critical patients. -
Key words:
- coroma virus disease 2019 /
- clinical characteristics
-
表 1 一般资料的比较[n;百分率(%)]
项目 普通型
(n=35)(危)重型
(n=39)合计
(n=74)χ2 P 年龄(x±s)/岁 51.63±10.97 57.90±11.98 54.93±11.78 2.34* < 0.05 性别 男 20(57.1) 21(53.8) 41(55.4) 0.08 > 0.05 女 15(42.9) 18(46.2) 33(44.6) 武汉及其他疫区接触史 9(25.7) 9(23.1) 18(24.3) 0.07 > 0.05 聚集性病例 20(57.1) 17(43.6) 37(50.0) 1.36 > 0.05 基础疾病 12(34.3) 23(59.0) 33(44.6) 4.51 < 0.05 高血压 4(11.4) 14(35.9) 18(24.3) — — 2型糖尿病 3(8.6) 10(25.6) 13(17.6) — — 冠心病 1(2.9) 2(5.1) 3(4.1) — — 脑梗死 1(2.9) 3(7.7) 4(5.4) — — 肾脏疾病 0(0.0) 2(5.1) 2(2.7) — — 支气管扩张 0(0.0) 1(2.6) 1(1.4) — — COPD 1(2.9) 1(2.6) 2(2.7) — — 甲状腺炎 0(0.0) 1(2.6) 1(1.4) — — 痛风 1(2.9) 1(2.6) 2(2.7) — — 房颤 1(2.9) 0(0.0) 1(1.4) — — 心肌缺血 1(2.9) 0(0.0) 1(1.4) — — 乙肝 1(2.9) 0(0.0) 1(1.4) — — 髂软骨瘤 0(0.0) 1(2.6) 1(1.4) — — 合并2种或2种以上基础病 1(2.9) 10(25.7) 11(14.9) 7.57 < 0.01 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 临床表现的比较[n;百分率(%)]
项目 普通型
(n=35)(危)重型
(n=39)合计
(n=74)χ2 P 发病到就诊时间/d 4.00(3.00~7.00) 7.00(3.00~9.00) 6.00(3.00-8.00) 2.01* < 0.05 临床症状 发热 35(100.0) 38(97.4) 73(98.6) — > 0.05 # 最高体温(x±s)/℃ 38.24±0.56 38.58±0.73 38.42±0.67 2.23△ < 0.05 37~37.9 8(22.9) 7(17.9) 15(20.3) — — 38~38.9 21(60.0) 15(38.5) 36(48.6) — — ≥39 6(17.1) 16(41.0) 22(29.7) — — 咳嗽 21(60.0) 31(79.5) 52(70.3) 3.35 > 0.05 咳痰 10(28.6) 13(33.3) 23(31.1) 0.20 > 0.05 胸闷 8(22.9) 31(79.5) 39(52.7) 23.73 < 0.01 呼吸困难 0(0.0) 8(20.5) 8(10.8) 6.06 < 0.01 腹泻 2(5.7) 8(20.5) 10(13.5) 3.46 > 0.05 纳差 2(5.7) 1(2.6) 3(4.1) 0.47 > 0.05 恶心呕吐 0(0.0) 1(2.6) 1(1.4) — > 0.05# *示zc值; #示Fisher′s确切概率法; △示t值
下载: 导出CSV
表 3 入院时实验室检查的比较[P50(P25, P75)]
项目 普通型(n=35) (危)重型(n=39) zc P 白细胞(x±s)/(×109/L) 5.03±1.47 6.52±2.98 2.77* < 0.01 中性粒细胞绝对值/(×109) 3.35(2.30, 4.17) 4.11(2.86, 6.41) 2.34 < 0.05 中性粒细胞百分比/% 64.70(59.70, 72.30) 64.70(59.70, 72.30) 3.33 < 0.01 淋巴细胞绝对值/(×109) 1.21(0.80, 1.61) 0.72(0.6, 1.5) 2.25 < 0.05 淋巴细胞百分比/% 25.50(17.70, 29.70) 16.60(10.95, 23.93) 2.99 < 0.01 血小板/(×109) 170.00(137.00, 284.00) 233.00(141.5, 303.00) 0.92 > 0.05 ALT/(U/L) 20.00(13.00, 40.00) 33.50(13.00, 51.25) 0.99 > 0.05 PCT/(ng/mL) 0.10(0.10, 0.15) 0.11(0.10, 0.19) 0.70 > 0.05 IL-6/(pg/mL) 2.32(1.50.9.17) 8.50(2.54, 21.96) 2.74 < 0.01 CRP/(mg/L) 7.80(3.70, 34.90) 26.70(4.90, 74.10) 2.11 < 0.05 肌酸激酶/(U/L) 57.00(40.00, 75.00) 40.00(29.00, 65.00) 1.79 > 0.05 白蛋白(x±s)/(g/L) 39.70±4.28 35.94±4.43 3.70# < 0.01 *示t′值; #示t值
下载: 导出CSV
-
[1] 华中科技大学同济医学院附属同济医院救治医疗专家组.新型冠状病毒感染的肺炎诊疗快速指南(第三版)[J].医药导报, 2020, 39(3):305 [2] 中华人民共和国国家卫生委员会.截至3月10日24时新型冠状病毒肺炎疫情最新情况[EB/OL].(2020-03-11)http://www.nhc.gov.cn/xcs/yqtb/202003/c588ee20113b4136b27f2a07faa7075b.shtml [3] 中华人民共和国国家卫生健康委员会.新型冠状病毒肺炎诊疗方案(试行第七版)[J].江苏中医药, 2020, 52(4):1 [4] CHAN JF, YUAN S, KOK KH, et al.A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission:a study of a family cluster[J].Lancet, 2020.DOI:10.1016/S0140-6736(20)30154-9 [5] WANG DW, HU B, HU C, et al.Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China[J].JAMA, 2020, 323(11):1061. doi: 10.1001/jama.2020.1585 [6] HUANG CL, WANG YM, LI XW, et al.Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China[J].The Lancet, 2020.DOI:10.1016/S0140-6736(20):30183-5 [7] 庄英杰, 陈竹, 李进, 等.26例新型冠状病毒肺炎确诊病例临床和流行病学特征[J].中华医院感染学杂志, 2020, 30(6):817. [8] 向天新, 刘家明, 许飞, 等.江西地区49例新型冠状病毒肺炎患者临床特征分析[J].中国呼吸与危重监护杂志, 2020, 19(2):1. [9] 房晓伟, 梅清, 杨田军, 等.2019新型冠状病毒感染的肺炎79例临床特征及治疗分析[J].中国药理学通报, 2020, 36(4):12. [10] TANG N, LI DJ, WANG X, et al.Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia[J].JTH, 2020, 18(4):844. doi: 10.1111/jth.14768 [11] LIN C, DING YX, XIE B, et al.Asymptomatic novel coronavirus pneumonia patient outside WuHan:the value of CT images in the course of the disease[J].Clin Imag, 2020, 63:7. doi: 10.1016/j.clinimag.2020.02.008 [12] CHEN NS, ZHOU M, DONG X, et al.Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China:a descriptive study[J].The Lancet, 2020.DOI:10.1016/S0140-6736(20)30211-7 -
 20200403.pdf
20200403.pdf
-

 点击查看大图
点击查看大图

图(2)表(3)
计量
- 文章访问数: 3876
- HTML全文浏览量: 1986
- PDF下载量: 18
- 被引次数: 0
