

-
新型冠状病毒肺炎(COVID-19)是2019年12月起在我国湖北省武汉市陆续发现的一种新型冠状病毒引发的急性下呼吸道疾病[1-2]。截至投稿时间,COVID-19已经累及全国大多数省市以及世界范围内25个国家。目前对于COVID-19的分子基因学、流行病学、临床病理及影像学的研究尚处于初步探索阶段。影像学特征在COVID-19早期诊断和病情评估中的价值已经得到广泛认可和重视,因此,深入了解COVID-19肺炎的影像学特征及其演变具有重要意义和临床价值,我们回顾性分析46例COVID-19肺炎病人的临床资料,旨在探讨其首诊时的临床特征和影像学特征,以期为临床诊断和治疗提供参考。现作报道。
-
回顾性分析2020年1月16日至2月17日凤阳县人民医院及蚌埠医学院第一附属医院确诊为COVID-19病人的临床资料及影像学资料。纳入标准:(1)符合国家卫生健康委员会颁布《新型冠状病毒感染的肺炎诊疗方案(试行第五版)》中的诊断标准;(2)入组病人均行薄层CT检查。最终纳入46例COVID-19病人,其中男22例,女24例;年龄1~83岁;有直接或间接武汉接触史45例。临床症状表现为咳嗽28例,发热40例,咽痛1例,少量痰液6例,乏力3例,肌肉酸痛7例,头痛4例,胸闷/呼吸困难3例,纳差1例,呕吐3例,腹泻1例。发热病人中低热(<37.3 ℃)6例,中热(37.3~38 ℃)12例,中高热(38.1~39 ℃)17例,高热(>39.0 ℃)5例。首次症状发生至第一次CT检查间隔时间为0~11 d,平均(5.1±3.4)d。
-
所有病人均进行薄层CT扫描,采用GE(Optima 680)64排螺旋CT和GE(LightSpeed)64排螺旋CT,扫描范围自胸廓入口至肺底。管电压120 kV,自动管电流,螺距0.984,常规扫描层厚和层间距均为5 mm;然后行0.625和1.25 mm薄层重建。CT纵隔窗宽350 Hu,窗位40 Hu;肺窗窗宽1 500 Hu,窗位-450 Hu。
-
由2名高年资放射科医生(包括1位高年资主治医生及1位副主任医生)在PACS图文处理工作站对病人肺部薄层CT图像进行分析,若所得结果不一致,则请第三名更高年资医生商讨后得出统一结论为最终结果。参考既往文献[3],分析指标包括:病灶分布累及肺段数目(≤3段、4~7段、>7段),累及肺叶(左肺、右肺、双肺),分布部位(胸膜下区、非胸膜下区、散在分布);单纯磨玻璃影、磨玻璃影伴实变、实变、小叶中心结节、铺路石征、晕征、反晕征、空泡或空腔、血管增粗影、支气管壁增厚、空气支气管征、马赛克征、胸膜增厚、胸腔积液、纵膈淋巴结增大等。并按照首次症状出现至第一次CT检查的时间间隔长短,将病人分为病程早期(≤3 d)、病程中期(4~7 d)和病程晚期(>7 d),对不同时期的影像学征象进行归纳分析。
-
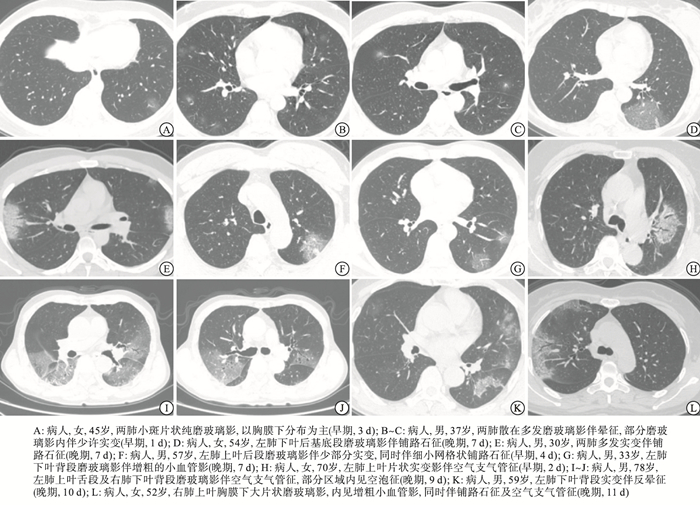
COVID-19病人病灶分布以同时累及双侧肺叶(39/46,84.8%)为主;以散在分布(27/46, 58.7%)为主,病灶以胸膜下区分布较中心区域多见,多分布于肺外带、沿支气管血管束走行;多数病人累及肺段达7个以上(27/46, 58.7%);在薄层CT征象方面,本组病人以单纯磨玻璃影(23/46,50.0%)、磨玻璃影伴实变(32/46,69.6%)、铺路石征(41/46,89.1%)、血管增粗影(41/46,89.1%)、晕征(34/46,73.9%)、空气支气管征(38/46,82.6%)较为常见,其他征象还包括实变、小叶中心结节、反晕征、空泡或空腔征、支气管壁增厚、马赛克征、胸膜增厚、胸腔积液、纵膈淋巴结增大等。典型病例见图 1。按照首次症状出现至第一次CT检查的时间间隔,将病人分为病程早期18例,病程中期14例, 病程晚期14例。与病程中期(42.9%)、晚期(14.3%)相比,病程早期病人单纯磨玻璃影多见(83.3%);病程晚期病人实变征象(71.4%)较病程早期(16.7%)、中期(35.7%)更为多见。就病灶分布而言,病程晚期病人累及>7个肺段比例(92.9%)高于病程早期(33.3%)和中期(57.1%)(见表 1)。
图 1 COVID-19病人影像学表现
指标 n 病程早期(n=18) 病程中期(n=14) 病程晚期(n=14) 累及肺段数 0~3 9 5(27.8) 4(28.6) 0(0.0) 4~7 10 7(38.9) 2(14.3) 1(7.1) > 7 27 6(33.3) 8(57.1) 13(92.9) 累及肺叶 左肺 6 4(22.2) 2(1.3) 0(0.0) 右肺 1 0(0.0) 1(7.1) 0(0.0) 双肺 39 14(77.8) 11(78.6) 14(100.0) 分布部位 非胸膜下区 4 2(11.1) 2(14.3) 0(0.0) 胸膜下区 15 6(33.3) 5(35.7) 4(28.6) 散在分布 27 10(55.6) 7(5.0) 10(71.4) 征象表现 单纯磨玻璃影 23 15(83.3) 6(42.9) 2(14.3) 实变 18 3(16.7) 5(35.7) 10(71.4) 磨玻璃影伴实变 32 11(61.1) 8(57.1) 13(92.9) 小叶中心结节 9 3(17.39) 4(28.6) 2(14.3) 铺路石征 41 14(77.8) 14(100.0) 13(92.9) 晕征 34 12(66.7) 8(57.1) 14(100.0) 反晕征 6 1(5.6) 2(14.3) 3(21.4) 空泡或空腔 9 2(11.1) 3(21.4) 4(28.6) 血管增粗影 41 15(83.3) 13(92.9) 13(92.9) 支气管壁增厚 12 4(22.2) 8(57.1) 4(28.6) 空气支气管征 38 14(77.8) 13(92.9) 11(78.6) 马赛克征 6 0(0.0) 3(21.4) 3(21.4) 胸膜增厚 17 4(22.2) 7 (50.0) 6(42.9) 胸腔积液 2 0(0.0) 0(0.0) 2(14.3) 纵隔淋巴结增大 6 2(11.1) 1(7.1) 3(21.4) 表 1 46例COVID-19病人影像学表现分析[n;百分率(%)]
-
COVID-19作为一种新型烈性传染性疾病迅速在国内蔓延,根据试行第五版《新型冠状病毒感染的肺炎诊疗方案》,COVID-19的诊断需要结合流行病学、临床表现、实验室指标和影像学表现进行综合诊断。而CT是一种十分快捷高效的检查方式,可以在短时间内筛查出大量疑似和/或发热病人,胸部影像诊断在COVID-19疑似病例及确诊病例诊断中具有重要价值,得到专家学者及一线临床医生的广泛认可。薄层胸部CT可以发现更多、更细致的病变表现,还可以通过后处理技术多平面、多方位、多角度地显示病灶细节。
由于COVID-19是首次出现、首次被诊断,该疾病的各方面特征尚处于逐步了解和探索阶段[4]。本研究中,97.8%(45/46)的发病病人都有直接或间接的武汉接触史,以中热或中高热及咳嗽为最常见症状,同时还有咽痛、少量痰液、乏力、肌肉酸痛、头痛、胸闷/呼吸困难、纳差、呕吐、腹泻等不同表现,与既往文献[2-3]报道基本一致。在病灶分布方面,本研究中COVID-19病人病灶多累及双侧肺叶,部分病人单侧肺发病,多见于早期病人;病灶多散在分布,常沿支气管血管束走行,病灶分布多位于肺外带,胸膜下区分布较中心区域多见;多数病人累及肺段达7个以上,与相关文献[4]报道结果大致相符。在CT征象方面,单纯磨玻璃影、磨玻璃影伴实变、铺路石征、空气支气管征、血管增粗影较为常见,多数征象常合并存在,本研究也出现了一些相对少见征象,如反晕征、空泡征、支气管壁增厚、马赛克征等。提示临床工作中,出现以上少见征象时仍需引起一线临床医生及放射诊断医生的注意。
此外,目前COVID-19的基本CT表现已经较为明确,但对于病人不同感染进程的CT表现尚无统一意见,目前多数研究集中于总体的COVID-19的影像学表现,对于病人不同时期的CT表现研究较少[5-7]。本研究根据病人首次症状发生至第一次CT检查的间隔时间,对病人病程进行初步分组,结果显示,病程早期病人单纯磨玻璃影较病程中、晚期多见;而病程晚期病人实变征象较病程早期、中期多见,累及>7个肺段比例高于病程早期和中期。与相关研究结论[8]基本一致。提示COVID-19的CT表现随疾病过程存在变化,可能是由于病人肺泡内浆液性炎性因子渗出的增多,肺泡壁增厚,间质炎症加重,逐步从早期的单纯局限性的磨玻璃影发展为大片的磨玻璃影和/或实变征象。此外,研究[8]显示,病程2 d以内病人的CT表现可以为阴性,而此时的RT-PCR为阳性。本组病例中虽然早期病人CT征象较轻且局限,但尚无完全阴性病例,可能由于样本量限制导致结果差异性。识别基于感染时间变化的CT变化模型不仅对了解疾病的病理、生理过程至关重要,对预测病人的病程进展和潜在并发症的发生也有重要意义。随着样本量的进一步扩大,应进一步细化间隔时间,同时纳入治疗后的随访结果,进行更具广度的COVID-19影像学特征分析。综上,COVID-19的临床和影像学特征多变,但总体具有一定的特征性,CT征象具有一定的动态演变规律,及时的胸部薄层CT检查可为病人早期诊断提供临床参考。
新型冠状病毒肺炎首诊的影像学特征分析
Analysis of the imaging characteristics of COVID-19 at the first diagnosis
-
摘要:
目的 分析新型冠状病毒肺炎(COVID-19)首诊的临床特征及影像学特征。 方法 回顾性分析46例确诊COVID-19病人的临床资料,均进行薄层CT扫描,分析病人病灶分布累及肺段数、累及肺叶情况、分布情况和征象表现,并按照首次症状出现至第一次CT检查的时间间隔长短,将病人分为病程早期(≤3 d)18例、病程中期(4~7 d)14例和病程晚期(>7 d)14例,对影像学表现进行归纳分析。 结果 46例COVID-19病人中,45例(97.8%)有直接或间接武汉接触史,临床症状以咳嗽(28/46,68.6%)和发热(40/46,87.0%)最为常见。影像学方面,COVID-19病人病灶分布以同时累及双侧肺叶(39/46,84.8%)为主,以散在分布(27/46,58.7%)为主,多数累及肺段达7个以上(27/46,58.7%);在CT征象方面,以单纯磨玻璃影(23/46,50.0%)、磨玻璃影伴实变(32/46,69.6%)、铺路石征(41/46,89.1%)、血管增粗影(41/46,89.1%)、晕征(34/46,73.9%)、空气支气管征(38/46,82.6%)较为常见。病程早期病人单纯磨玻璃影较病程中、晚期多见;而病程晚期病人实变征象较病程早期、中期多见,累及>7个肺段比例高于病程早期和中期。 结论 COVID-19病人的临床症状及影像学征象表现多样,但具有一定特征性,CT征象具有一定的演变规律,CT检查结合临床症状对COVID-19的早期诊断有重要价值。 Abstract:Objective To analyze the initial clinical features and imaging finding of corona virus disease 2019 (COVID-19). Methods The clinical data of 46 patients with COVID-19 were retrospectively analyzed.The thin-slice CT scan in all cases were performed to analyze the number of pulmonary segments and lobes, distribution and signs of lesion involvement.According to the time interval between the first symptom and CT examination, the course of disease was divided into the early stage(18 cases, ≤ 3d), middle stage(14 cases, 4-7d) and advanced stage (14 cases, >7d), and the imaging findings were analyzed. Results Among 46 cases with COVID-19, the history of direct or indirect exposure to Wuhan in 45 cases(97.8%) were identified, and the most common clinical symptoms were cough(28/46, 68.6%) and fever (40/46, 87.0%).In terms of clinical symptoms, the lesions were mainly distributed in bilateral lungs(39/46, 84.8%), the diffused distribution was main, and the number of involved lung segments was more than 7(27/46, 58.7%).The thin-section CT images were mainly characterized by pure ground grass opacity (23/46, 50.0%), ground grass opacity complicated with glass grinding consolidation(32/46, 69.6%), paving stone sign(41/46, 89.1%), vascular thickening(41/46, 89.1%), halo sign(34/46, 73.9%) and air bronchogram(38/46, 82.6%).In the early stage of disease, the patients with pure ground grass opacity were more common compared with patients at the middle or late stage of disease.The signs of consolidation in the advanced patients were more common compared with patients at the early and middle stages of disease, and the proportion of the involve lung segment more than 7 in the advanced patients was higher than that in the early and middle stages of disease. Conclusions The clinical and imaging signs of COVID-19 patients are complex and changeable, but which has the certain characteristics, and the CT signs have a certain evolution law.The CT examination combined with clinical symptoms has important clinical significance and value in the early diagnosis of COVID-19. -
Key words:
- corona virus disease 2019 /
- thin-section CT /
- pure ground grass opacity /
- consolidation
-
表 1 46例COVID-19病人影像学表现分析[n;百分率(%)]
指标 n 病程早期(n=18) 病程中期(n=14) 病程晚期(n=14) 累及肺段数 0~3 9 5(27.8) 4(28.6) 0(0.0) 4~7 10 7(38.9) 2(14.3) 1(7.1) > 7 27 6(33.3) 8(57.1) 13(92.9) 累及肺叶 左肺 6 4(22.2) 2(1.3) 0(0.0) 右肺 1 0(0.0) 1(7.1) 0(0.0) 双肺 39 14(77.8) 11(78.6) 14(100.0) 分布部位 非胸膜下区 4 2(11.1) 2(14.3) 0(0.0) 胸膜下区 15 6(33.3) 5(35.7) 4(28.6) 散在分布 27 10(55.6) 7(5.0) 10(71.4) 征象表现 单纯磨玻璃影 23 15(83.3) 6(42.9) 2(14.3) 实变 18 3(16.7) 5(35.7) 10(71.4) 磨玻璃影伴实变 32 11(61.1) 8(57.1) 13(92.9) 小叶中心结节 9 3(17.39) 4(28.6) 2(14.3) 铺路石征 41 14(77.8) 14(100.0) 13(92.9) 晕征 34 12(66.7) 8(57.1) 14(100.0) 反晕征 6 1(5.6) 2(14.3) 3(21.4) 空泡或空腔 9 2(11.1) 3(21.4) 4(28.6) 血管增粗影 41 15(83.3) 13(92.9) 13(92.9) 支气管壁增厚 12 4(22.2) 8(57.1) 4(28.6) 空气支气管征 38 14(77.8) 13(92.9) 11(78.6) 马赛克征 6 0(0.0) 3(21.4) 3(21.4) 胸膜增厚 17 4(22.2) 7 (50.0) 6(42.9) 胸腔积液 2 0(0.0) 0(0.0) 2(14.3) 纵隔淋巴结增大 6 2(11.1) 1(7.1) 3(21.4)  下载: 导出CSV
下载: 导出CSV
-
[1] HUANG C, WANG Y, LI X, et al.Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China[J].Lancet, 2020, 395(10223):497. doi: 10.1016/S0140-6736(20)30183-5 [2] ZHU N, ZHANG D, WANG W, et al.A Novel coronavirus from patients with pneumonia in China, 2019[J].New Engl J Med, 2020, 382(8):727. doi: 10.1056/NEJMoa2001017 [3] SONG F, SHI N, SHAN F, et al.Emerging coronavirus 2019-nCoV pneumonia[J].Radiology, 2020, 295(1):200274. doi: 10.1148/radiol.2020200274 [4] LU R, ZHAO X, LI J, et al.Genomic characterisation and epidemiology of 2019 novel coronavirus:implications for virus origins and receptor binding[J].Lancet, 2020, 395(10224):565. doi: 10.1016/S0140-6736(20)30251-8 [5] LEI J, LI J, LI X, et al.CT Imaging of the 2019 Novel Coronavirus (2019-nCoV) Pneumonia[J].Radiology, 2020, 295(1):18. doi: 10.1148/radiol.2020200236 [6] LIU P, TAN X.2019 Novel Coronavirus (2019-nCoV) Pneumonia[J].Radiology, 2020, 295(1):200257. doi: 10.1148/radiol.2020200257 [7] PAN F, YE T, SUN P, et al.Time course of lung changes on chest CT during recovery from 2019 Novel Coronavirus (COVID-19) Pneumonia[J].Radiology, 2020.DOI:10.1148/radiol.2020200370. [8] BERNHEIM A, MEI X, HUANG M, et al.Chest CT findings in Coronavirus Disease-19(COVID-19):relationship to duration of infection[J].Radiology, 2020.DOI:10.1148/radiol.2020200463. -
 20200404.pdf
20200404.pdf
-

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 4340
- HTML全文浏览量: 2145
- PDF下载量: 14
- 被引次数: 0
