

-
胃癌在我国较为高发,是临床常见的消化系统恶性肿瘤。由于早期缺乏典型的临床症状,多数病人在获得确诊时已失去最佳治疗时机。即便接受手术治疗,5年生存期仍然不理想[1-3]。近年来,针对肿瘤分子病理学的研究在临床诊断、预后判断和发病机制上均显示出较大价值[4]。Enah属于Ena/VASP 蛋白家族中的一员,广泛表达于哺乳动物细胞之中,主要参与细胞塑形、迁移及黏附等生物学过程[5-6]。近年来Enah被证实高表达于结直肠肿瘤及肝癌等消化系统恶性肿瘤组织中,且其表达量增高提示预后不良[7-8]。然而,Enah在胃癌组织中的表达情况以及是否具有潜在临床意义尚需进一步研究。本文拟分析Enah在胃癌组织中的表达情况,分析其与相关临床、病理参数之间的联系,及其对术后生存期的影响。现作报道。
-
选取2012年2月至2013年10月我院行胃癌根治术病人。入选标准:明确诊断为原发性胃癌;成功施行胃癌根治术并实现R0切除。排除标准:合并其他组织起源的恶性肿瘤;死于除胃癌以外的其他原因。通过电子病历系统采集病人临床资料信息;通过电话随访采集术后5年生存情况。依据纳入及排除标准最终入选97例。
-
原发性胃癌的临床及病理诊断依据胃癌诊断及分期系统(AJCC)[9]。回顾病人手术标本蜡块,采用免疫组织化学标记Enah,并采用Image-Pro Plus6.0软件计算目标蛋白光密度值(integrated option density,IOD),以癌旁组织Enah光密度值为基线计算癌组织和癌旁组织Enah的相对表达量[10]。通过电话随访获取病人术后5年生存情况。分析影响胃癌病人术后生存的影响因素。
-
采用Mann-Whitney U检验、Kaplan-Meier(K-M)曲线、生存分析(Log-rank χ2检验)和Cox多元回归模型。
-
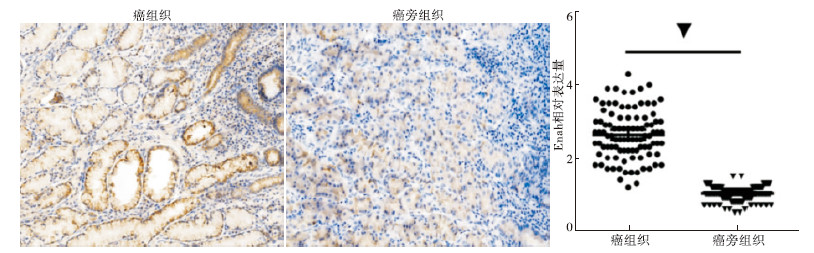
Enah在癌组织中表达水平较高,定位于癌细胞细胞质;其在癌旁组织中表达量微弱,细胞定位为胞质(见图 1A)。胃癌组织中Enah相对表达量明显高于癌旁组织(2.63, 95%CI:2.493~2.767 vs 1.00, 95%CI:0.976~1.06;Mann-Whitney U=27.500,P<0.01)(见图 1B)。
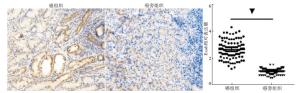
图 1 胃癌组织中Enah表达情况
-
以胃癌组织中Enah相对表达量的中位数(2.5)为界,分为Enah低表达组(n=48)和高表达组(n=49)。2组年龄、性别、病理类型、肿瘤大小、T分期及N分期差异均无统计学意义(P>0.05)。Enah高表达组在病理分级为G3~G4、CEA≥5 μg/L及CA19-9≥37 kU/L的比例均高于Enah低表达组(P<0.05)(见表 1)。
因素 n Enah χ2 P 低表达(n=48) 高表达(n=49) 年龄/岁 <60 35 19(54.3) 16(45.7) 0.51 <0.05 ≥60 62 29(46.8) 33(53.2) 性别 男 6631 36(54.5) 30(45.5) 2.126 <0.05 女 31 12(38.7) 19(61.3) 病理分级 G1~G2 48 29(60.4) 19(39.6) 4.54 <0.05 G3~G4 49 19(38.8) 30(61.2) 病理类型 腺癌 82 41(50.0) 41(50.0) 0.06 >0.05 其他△ 15 7(46.7) 8(53.3) 肿瘤大小/cm <5 58 29(50.0) 29(50.0) 0.02 <0.05 ≥5 39 19(48.7) 20(51.3) T分期 1~2期 10 6(60.0) 4(40.0) 0.12 >0.05 3~4期 87 42(48.3) 45(51.7) N分期 0~1期 49 27(55.1) 22(44.9) 1.25 >0.05 2~3期 48 21(43.8) 27(56.3) CEA水平/(μg/L) <5 70 39(55.7) 31(44.3) 3.90 <0.05 ≥5 27 9(33.3) 18(66.7) CA19-9/ (kU/L) <37 74 42(56.8) 32(43.2) 6.60 <0.05 ≥37 23 6(26.1) 17(73.9) △示其他病理类型包括黏液腺癌和印戒细胞癌 表 1 Enah在胃癌组织中的表达与临床病理指标间的关系[n;构成比(%)]
-
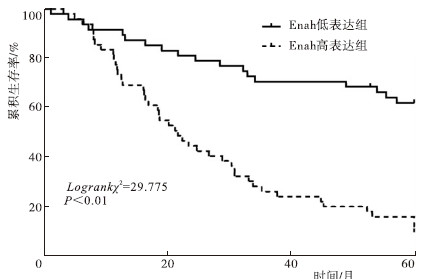
Enah高表达组术后5年生存率10.2%(5/49),明显低于Enah低表达组的 62.5%(30/48)(Log-rank χ2=29.78,P<0.01)(见图 2)。

图 2 Enah高表达组与低表达组术后5年生存率比较
-
单因素分析显示,病理分级、N分期、Enah表达量、CEA及CA19-9可能影响胃癌术后5年生存率(P<0.01)。将单因素分析所得阳性结果纳入Cox多元回归模型分析得出:病理分级为G3~G4、Enah高表达及CA19-9≥37kU/L是影响胃癌术后5年生存率的独立危险因素(P<0.05~P<0.01)(见表 2)。
因素 单因素分析 多因素分析 Log-rank χ2 P HR 95%CI P 性别(男 vs 女) 0.139 >0.05 — — — 年龄(<60 vs ≥60) 2.092 >0.05 — — — 病理分级(G1~G2 vs G3~G4) 29.653 <0.01 2.632 1.386~4.996 <0.01 癌细胞类型(腺癌vs其他) 2.364 >0.05 — — — 肿瘤大小(<5 cm vs ≥5 cm) 1.017 >0.05 — — — T分期(T1~T2 vs T3~T4) 2.15 >0.05 — — — N分期(N0~N1 vs N2~N3) 9.229 <0.01 1.215 0.705~2.093 >0.05 Enah表达(高表达 vs 低表达) 29.775 <0.01 3.180 1.751~5.777 <0.01 CEA水平(5μg/L vs ≥5μg/L) 13.421 <0.01 1.559 0.894~2.719 >0.05 CA19-9(37kU/L vs≥37kU/L) 41.395 <0.01 2.248 1.198~4.219 <0.05 表 2 胃癌组织中Enah的表达对术后5年生存影响的Cox回归分析
-
胃癌是一种严重威胁人类健康的恶性肿瘤,最新全球癌症调查报告显示其居于癌性致死的第二位[11]。虽以手术为主的综合治疗显著改善了多种恶性肿瘤的远期生存率,但胃癌的远期预后仍然不佳,可能主要源于难以早期诊断和早期即可发生血行、淋巴管转移等因素有关[12-13]。事实上,人类对胃癌细胞本身的生物学行为和代谢机制不明确也是限制其诊疗水平提高的因素之一。肿瘤分子病理学领域的探索有望为胃癌的临床诊疗提供线索和思路。
Enah蛋白可表达于正常细胞内,主要调控细胞的运动等生物学行为;而其在多种实体瘤中的异常高表达被证实与肿瘤的进展和预后相关,特别是高转移性实体肿瘤中[5, 7-8]。我们受此启发,针对胃癌也存在早期易转移的特征,采用免疫组织化学标记了Enah。结果显示,与癌旁组织比较Enah在胃癌组织中呈现显著高表达,Enah高表达的病人具有更高的病理分级及T分期,同时此类病人具有更高水平的外周血CEA及CA19-9。病理分级提示肿瘤的恶性程度、T分期提示肿瘤的浸润深度,而CEA和CA19-9是临床上经典的肿瘤进展和预后判断指标[14-15]。提示Enah的高表达可一定程度反映胃癌病人的肿瘤侵袭性和进展情况。为明确Enah是否为影响胃癌远期预后的独立风险因素,我们采用Cox回归模型分析发现Enah联同CA19-9及病理分级同属于影响胃癌远期生存率的独立风险因素,提示Enah对于胃癌的预后判断具有一定参考价值。
综上,Enah在胃癌组织中呈现高表达并与肿瘤进展相关,对预后判断具有一定价值。但由于样本量有限,所得结论仍需进一步扩大样本量或采用多中心研究的方式予以证实。
Enah在胃癌组织中的表达及临床价值研究
Study on the expression and clinical value of Enah in gastric cancer tissues
-
摘要:
目的分析Enah蛋白在胃癌中的表达及临床价值,以期为胃癌的诊疗提供参考。 方法纳入行胃癌根治术病人97例,使用免疫组化标记胃癌组织和癌旁组织内的Enah,并计算目标蛋白光密度值,分析2种组织中Enah的表达差异。以胃癌组织内Enah表达量的中位数为界,将病人分为Enah高表达组(n=48)和低表达组(n=49),比较2组临床病理学参数及术后5年生存率。采用Cox回归模型分析Enah是否为胃癌术后5年死亡的独立危险因素。 结果胃癌组织中Enah相对表达量高于癌旁组织(P<0.01)。Enah高表达组在病理分级为G3~G4、T分期为3~4期、CEA≥5μg/L及CA19-9≥37kU/L的比例均高于Enah低表达组(P<0.05)。Enah高表达组术后5年生存率明显低于Enah低表达组(P<0.01)。Cox多元回归模型分析得出:病理分级为G3~G4、Enah高表达及CA19-9≥37kU/L是影响胃癌术后5年生存率的独立危险因素(P<0.05~P<0.01)。 结论Enah在胃癌组织中呈现高表达,并与肿瘤进展相关,对预后判断具有一定价值。 Abstract:ObjectiveTo analyze the expression and clinical value of Enah in gastric cancer tissues in order to provide reference for the diagnosis and treatment of gastric cancer. MethodsEnah in gastric and paracancer tissues of 97 patients treated with radical gastrectomy were stained using immunohistochemistry to calculate the target protein integrated option density(IOD) for comparing the expression differences of Enah between two tissues.All patients were divided into the high expression of Enah group(n=48) and low expression of Enah group(n=49) according to the median number of Enah expression in gastric cancer tissues.The clinical pathological parameters and 5-year survival rate were compared between two groups.The Cox regression model was used to analyze whether Enah was an independent risk factor of 5-year mortality after gastric cancer surgery. ResultsThe relative expression level of Enah in gastric cancer tissues was significantly higher than that in adjacent tissues(P<0.01).The ratios of patients with pathological grades for G3-G4, T stage 3-4, CEA≥5μg/L and CA19-9≥37kU/L in high expression of Enah group were higher those in low expression of Enah group(P<0.05).The postoperative 5-year survival rate in high expression of Enah group were significantly lower those in low expression of Enah group(P<0.01).The results of Cox multiple regression model analysis showed that the pathological grade for G3-G4, high expression of Enah and CA19-9≥37kU/L were the independent risk factors of 5-year survival rate after gastric cancer surgery. ConclusionsThe expression level of Enah in gastric cancer tissues is high, which is associated with the tumor progression, and has certain diagnostic value for prognosis. -
Key words:
- gastric neoplasms /
- Enah /
- molecular pathology /
- 5-year survival rate
-
表 1 Enah在胃癌组织中的表达与临床病理指标间的关系[n;构成比(%)]
因素 n Enah χ2 P 低表达(n=48) 高表达(n=49) 年龄/岁 <60 35 19(54.3) 16(45.7) 0.51 <0.05 ≥60 62 29(46.8) 33(53.2) 性别 男 6631 36(54.5) 30(45.5) 2.126 <0.05 女 31 12(38.7) 19(61.3) 病理分级 G1~G2 48 29(60.4) 19(39.6) 4.54 <0.05 G3~G4 49 19(38.8) 30(61.2) 病理类型 腺癌 82 41(50.0) 41(50.0) 0.06 >0.05 其他△ 15 7(46.7) 8(53.3) 肿瘤大小/cm <5 58 29(50.0) 29(50.0) 0.02 <0.05 ≥5 39 19(48.7) 20(51.3) T分期 1~2期 10 6(60.0) 4(40.0) 0.12 >0.05 3~4期 87 42(48.3) 45(51.7) N分期 0~1期 49 27(55.1) 22(44.9) 1.25 >0.05 2~3期 48 21(43.8) 27(56.3) CEA水平/(μg/L) <5 70 39(55.7) 31(44.3) 3.90 <0.05 ≥5 27 9(33.3) 18(66.7) CA19-9/ (kU/L) <37 74 42(56.8) 32(43.2) 6.60 <0.05 ≥37 23 6(26.1) 17(73.9) △示其他病理类型包括黏液腺癌和印戒细胞癌  下载: 导出CSV
下载: 导出CSV
表 2 胃癌组织中Enah的表达对术后5年生存影响的Cox回归分析
因素 单因素分析 多因素分析 Log-rank χ2 P HR 95%CI P 性别(男 vs 女) 0.139 >0.05 — — — 年龄(<60 vs ≥60) 2.092 >0.05 — — — 病理分级(G1~G2 vs G3~G4) 29.653 <0.01 2.632 1.386~4.996 <0.01 癌细胞类型(腺癌vs其他) 2.364 >0.05 — — — 肿瘤大小(<5 cm vs ≥5 cm) 1.017 >0.05 — — — T分期(T1~T2 vs T3~T4) 2.15 >0.05 — — — N分期(N0~N1 vs N2~N3) 9.229 <0.01 1.215 0.705~2.093 >0.05 Enah表达(高表达 vs 低表达) 29.775 <0.01 3.180 1.751~5.777 <0.01 CEA水平(5μg/L vs ≥5μg/L) 13.421 <0.01 1.559 0.894~2.719 >0.05 CA19-9(37kU/L vs≥37kU/L) 41.395 <0.01 2.248 1.198~4.219 <0.05
下载: 导出CSV
-
[1] 许可葵,王静,刘湘国,等.2009~2014年湖南省肿瘤登记地区恶性肿瘤发病与死亡分析[J].中国肿瘤,2018,27(10):738. doi: 10.11735/j.issn.1004-0242.2018.10.A002 [2] 陈万青,李贺,孙可欣,等.2014年中国恶性肿瘤发病和死亡分析[J].中华肿瘤杂志,2018,40(1):5. [3] 陈万青,孙可欣,郑荣寿,等.2014年中国分地区恶性肿瘤发病和死亡分析[J].中国肿瘤,2018,27(1):1. [4] MA N,XU H,ZHOU Y,et al.Analyzing the molecular mechanism of the tissue specificity of gastrointestinal stromal tumors by using bioinformatics approaches[J].J Buon,2018,23(4):1149. [5] JANG DG,SIM HJ,SONG EK,et al.A thioredoxin fold protein Sh3bgr regulates Enah and is necessary for proper sarcomere formation[J].Dev Biol,2015,405(1):1. [6] GUO F,REN X,DONG Y,et al.Constitutive expression of PPARγ inhibits proliferation and migration of gastric cancer cells and down-regulates Wnt/β-Catenin signaling pathway downstream target genes TERT and ENAH[J].Gene,2016,584(1):31. doi: 10.1016/j.gene.2016.03.003 [7] TOYODA A,KAWANA H,AZUHATA K,et al.Aberrant expression of human ortholog of mammalian enabled (hMena) in human colorectal carcinomas:implications for its role in tumor progression[J].Int J Oncol,2009,34(1):53. [8] HU K,WANG J,YAO Z,et al.Expression of cytoskeleton regulatory protein Mena in human hepatocellular carcinoma and its prognostic significance[J].Med Oncol,2014,31(5):939. doi: 10.1007/s12032-014-0939-y [9] WASHINGTON K.7th edition of the AJCC cancer staging manual:stomach[J].Ann Surg Oncol,2010,17(12):3077. doi: 10.1245/s10434-010-1362-z [10] GE Y,LI Y,CHEN Q,et al.Adipokine apelin ameliorates chronic colitis in Il-10-/-mice by promoting intestinal lymphatic functions[J].Biochem Pharmacol,2018,148(2):202. [11] BRAY F,FERLAY J,SOERJOMATARAM I,et al.Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J].CA Cancer J Clin,2018,68(6):394. doi: 10.3322/caac.21492 [12] 闵丛丛.胃癌淋巴结转移分子标志物的研究进展[J].中国微创外科杂志,2018,18(1):68. doi: 10.3969/j.issn.1009-6604.2018.01.018 [13] 徐惠绵.胃癌转移规律及亚临床转移的基础和临床研究[J].消化肿瘤杂志(电子版),2015,7(1):48. doi: 10.3969/j.issn.1674-7402.2015.01.012 [14] 郑南翔,单廷.胃癌根治术患者术后早期复发转移的相关危险因素[J].中国老年学杂志,2017,37(17):4301. doi: 10.3969/j.issn.1005-9202.2017.17.063 [15] 黑涛.胃癌患者术后检测CEA和CA19-9的临床意义[J].实用癌症杂志,2018,33(6):965. doi: 10.3969/j.issn.1001-5930.2018.06.029 -

 点击查看大图
点击查看大图
图(2)表(2)
计量
- 文章访问数: 5253
- HTML全文浏览量: 2726
- PDF下载量: 12
- 被引次数: 0
