

-
牙槽嵴裂是由于胚胎发育期球状突和上颌突融合障碍所致。其常表现为牙弓的连续性消失、颌骨骨质缺损、口鼻瘘、牙齿的缺失或异位萌出、鼻翼塌陷等[1]。牙槽嵴裂的存在也严重影响到了唇腭裂术后恢复的效果,造成牙齿的萌出及修复障碍,阻碍了后期正畸及正颌的治疗[2]。牙槽嵴裂手术是通过植骨恢复牙槽突的骨质的连续性和关闭软组织间隙。本文对改良式牙槽嵴裂植骨术及常规牙槽嵴裂植骨术病人术后植骨成功率及影像学资料进行分析,对2种术式术后恢复情况进行评价。现作报道。
-
选取2016年1月至2017年8月在蚌埠医学院第一附属医院口腔科就诊并进行牙槽嵴裂植骨术修复的病人,年龄9~14岁。将病人随机分为2组,各22例。行改良式牙槽嵴裂植骨术的单侧牙槽嵴裂病人为改良式植骨术组(A组),其中男12例,女10例;年龄9~14岁。行常规牙槽嵴裂植骨术的病人为常规植骨术组(B组),其中男11例,女11例;年龄9~14岁。2组病人年龄、裂隙宽度等一般资料均具有可比性。本研究为蚌埠医学院第一附属医院高新技术项目,本课题已获得伦理审批。
-
利用ABYHOLM等[3]描述的唇侧单切口术式。即在唇侧黏膜转折处做单一切口,并增加2个水平切口,将裂隙内黏膜分为颊侧瓣和腭瓣, 严密缝合,分别关闭腭侧裂隙及鼻底裂隙(见图 1)。

图 1 常规牙槽嵴裂植骨术
-
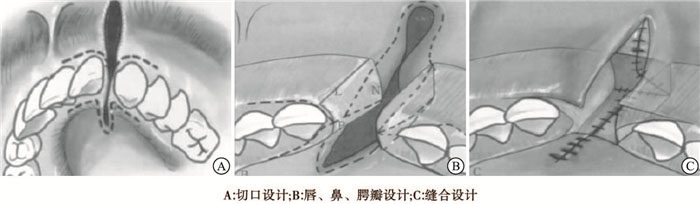
利用杨超等[4]所述的改良式牙槽嵴裂植骨术的手术方式进行手术。即在腭侧裂隙两侧作纵行切口,再从牙槽嵴顶沿两侧龈乳头作水平切口,在裂隙两侧形成两个蒂在后的腭瓣。如果腭侧裂隙较宽,腭侧裂隙缘切口线可适当向唇侧上移,以确保腭部裂隙能够关闭。然后沿唇侧裂隙附着龈向两侧作水平切开约2个牙位,近中端切口线至患侧中切牙的远中,原则上不超过唇系带,保留牙龈乳头。并将唇侧切口与腭侧切口在牙槽突顶联通。在牙槽突裂隙断端侧壁,作自前下至后上的切开,形成2个蒂在后的裂隙鼻腔瓣。对位严密缝合各黏膜瓣,形成植骨床(见图 2)。

图 2 手术切口设计示意图
-
在术前对病人缺损区域拍摄锥形束CT(CBCT),进行术前骨量缺损的评估;对病人术后第3、6、12个月进行随访,拍摄CBCT用于统计缺损区域骨量恢复情况,于术后第12个月拍摄全景片用于统计改良式牙槽嵴裂植骨术手术成功率,以BERGLAND[5]牙槽嵴裂植骨分级标准进行统计, 以裂隙侧骨高度与正常侧牙槽嵴高度比例为标准,共分为4型:Ⅰ型,裂隙处牙槽骨高度基本正常;Ⅱ型,裂隙侧牙槽骨高度至少为正常牙槽嵴高度的3/4;Ⅲ型,裂隙侧牙槽骨高度少于正常高度的3/4;Ⅳ型,裂隙部位没有连续的骨桥。在此标准中,Ⅰ型和Ⅱ型为临床治疗成功;Ⅲ型和Ⅳ型为临床治疗失败。统计不同术式病人与术后第12个月的手术成功率。
术前拍摄CBCT,确定缺损处骨体积;术后第3、6、12个月利用CBCT进行随访,获取三维图像,利用Planmaeca remix 3.8.3对牙槽嵴裂的骨质缺损处进行处理,利用鼠标沿骨质缺损边缘画出缺损体积轮廓,而后计算机自动生成牙槽嵴裂缺损的三维图像并自动计算牙槽嵴裂缺损处的体积数值,通过计算不同时点的骨量存活比,以此判断缺损处骨量恢复情况[6 ]。
-
采用χ2检验、t检验、重复测量方差分析和q检验。
-
A组术后成功率为82.8%(18例),B组术后成功率为50.0%(11例),A组高于B组(χ2=4.96,P < 0.05)。
-
术后第3、6、12个月时缺损区域植骨存活比A组均高于B组(P < 0.05)。2组病人第3个月时植骨存活比均高于第6个月和第12个月(P < 0.01);第6个月和第12个月植骨存活比差异无统计学意义(P>0.05)(见表 1)。
分组 n 3个月 6个月 12个月 F P A组 22 69.67±7.63 52.45±9.17** 49.43±8.28** 46.37 < 0.01 B组 22 64.32±8.96 46.73±9.07** 43.81±8.58** 40.35 < 0.01 t — 2.13 2.08 2.21 — — P — < 0.05 < 0.05 < 0.05 — — q检验:与3个月时比较**P < 0.01 表 1 2组病人不同时点植骨存活比比较(x±s;%)
-
牙槽嵴裂植骨术目的在于重建上颌骨的完整性,关闭口鼻瘘,并为唇部及鼻底提供骨质支撑[7]。而对于牙槽嵴裂植骨术而言,手术难点常包括:(1)牙槽突裂是三维立体结构内的发育异常,不仅包括牙槽突、颌骨及鼻底部的三维立体骨组织缺损,还包括局部软组织黏膜的异位,难以同时恢复两者外形;(2)手术操作过程中因手术空间狭窄而带来的手术难度的增加;(3)不同软组织瓣的性质及张力不同,易造成软组织穿孔。而牙槽嵴裂的裂隙宽度、裂隙类型,术者、植骨时机、移植骨密度、植骨区黏膜封闭情况、口腔卫生等均对牙槽嵴裂植骨效果有一定影响[8]。故而牙槽嵴裂植骨术常难取得良好而稳定的术后效果,且有研究发现植骨术后骨量吸收情况严重,不同个体间存在差异较大[9-13]。若想获得良好的术后效果,切口设计需做到既可充分暴露腭侧骨面及鼻底平面的植骨盲点,又可在无张力的状态下关闭创面。因此如何设计植骨瓣、如何在无张力状态下关闭创面及创面的严密缝合是手术成功的关键[14-15]。
于常规牙槽嵴裂植骨术而言,常于唇侧做单侧切口,易造成腭侧及鼻底处植骨床暴露不佳,导致术中植入骨量减少;且易造成腭侧剩余黏膜过多,造成腭侧黏膜堆积,创缘愈合不良,瘢痕形成,压迫植入骨粉造成植入骨吸收。而改良式牙槽嵴裂植骨术将切口下降至腭侧黏膜转折处,同时利用骨断端裂隙侧黏膜做三角形黏膜瓣向上翻转关闭鼻底平面,既避免了唇侧及牙槽嵴顶处黏膜剩余过少,又减少了腭侧黏膜组织的剩余,充分暴露了腭侧骨断端及牙槽骨鼻底平面,使植骨床暴露充分,增加术中植入骨量,同时避免了腭侧黏膜组织剩余过多植入骨粉造成的挤压。杨超等[16]经过测量后发现,术后1周裂隙处总体骨量占入比可达88%,腭侧骨量占入比率为84%,唇侧骨量占入比为93%,均明显高于KINDELAN等[2]评价标准中>75%为优秀的标准。故而笔者认为改良式牙槽嵴裂通过切口设计的改良可使手术视野暴露良好、软组织关闭效果变好,使手术成功率明显增加。
目前国内外已有一些学者[9-11]运用CBCT对牙槽突裂植骨术进行相关研究认为,常规牙槽嵴裂植骨术存在腭侧植入骨量不足而唇颊侧过度充填,前庭沟变浅和红唇内卷等缺陷。但主要集中在常规牙槽嵴裂植骨术后各类因素对移植骨吸收的影响,未针对改良式牙槽突裂植骨术及常规牙槽嵴裂植骨术植骨量及术后骨量恢复情况进行量化比较分析。本研究通过对常规牙槽嵴裂植骨术与改良式牙槽嵴裂植骨术的术后植骨量存活比及术后手术成功率进行对比,A组术后成功率高于B组(P < 0.05),术后第3、6、12个月时缺损区域植骨存活比A组均高于B组(P < 0.05)。笔者认为改良式牙槽嵴裂植骨术较常规牙槽嵴裂植骨术而言,术后成功率明显增加,术后存活骨量也明显增加。这与常规牙槽嵴裂植骨术切口线为唇侧黏膜转折处的单一切口有关,此切口易造成唇侧及牙槽嵴顶处剩余黏膜组织量较少,增加了唇侧裂隙关闭的难度,而腭侧黏膜组织过多,易造成软组织堆积,不利于创缘愈合,易造成黏膜穿孔,影响术后效果;且过多的腭侧黏膜组织剩余,常易形成瘢痕,对植入骨造成压迫,产生骨吸收。而改良式牙槽嵴裂植骨术将切口下降至骨断端腭侧黏膜转折处,充分暴露了牙槽突裂腭侧骨断端,较满意地暴露了植骨床,减少了植骨盲点,可于术中增加腭侧及鼻底的骨质植入量,同时牙槽突裂隙断端裂隙侧黏膜做三角形黏膜瓣做向上翻转关闭鼻底平面,以此可见增加唇侧黏膜剩余量,预留黏膜组织关闭唇侧裂隙,以达到在无张力的情况下关闭唇侧裂隙,同时减少了腭侧软组织的堆积造成的原本植骨空间的占据。且笔者认为,大量的腭侧黏膜的堆积对植骨后腭侧的移植骨粉会产生一定的压力,易造成植骨后移植骨的吸收,这也是术后第3个月常规牙槽嵴裂植骨术骨量恢复不佳的原因之一。同时,笔者发现,2组病人的术后骨量成活比变化主要发生在术后前6个月,而在术后6个月及12个月时,骨量存活比虽有变化,但差异无统计学意义(P>0.05)。故而,移植骨吸收主要发生于术后6个月以内,术后6个月后骨量虽有吸收,但趋于稳定,可进行术后正畸等进一步治疗。
综上所述,笔者认为改良式牙槽嵴裂植骨术较常规手术而言,通过术中充分暴露植骨床,增大植骨量,并有效减少增加手术成功率及术后骨量恢复,可获得较好的临床效果,有利于后期正畸修复等工作的进行。
改良式牙槽嵴裂植骨术后的植骨效果评价
Evaluation of bone graft effect after modified alveolar bone grafting
-
摘要:
目的对改良式牙槽嵴裂植骨术修复牙槽嵴裂的术后效果进行评价。 方法采用随机对照试验分析44例单侧牙槽嵴裂病人的临床资料,其中改良式牙槽嵴裂植骨术组(A组)22例和常规牙槽嵴裂植骨术组(B组)22例。术后第3、6、12个月进行随访,比较2组病人的术后植骨成功率及骨缺损处的体积变化。 结果A组术后成功率为82.8%(18例)高于B组的50.0%(11例)(P < 0.05);术后第3、6、12个月时缺损区域植骨存活比A组均高于B组(P < 0.05)。2组病人术后第3个月时植骨存活比均高于第6个月和第12个月(P < 0.01),第6个月和第12个月植骨存活比差异均无统计学意义(P>0.05)。 结论对于单侧牙槽嵴裂病人,改良式牙槽嵴裂植骨术可有效提高术后植骨存活率,术后骨量恢复明显增加;术后骨吸收主要发生于术后前6个月,6~12个月时基本稳定。 Abstract:ObjectiveTo estimate the bone graft effect after modified alveolar bone grafting(ABG). MethodsThe clinical data of 44 patients with unilateral alveolar cleft were retrospectively analyzed.The patients were divided into the modified ABG approach group(group A, 22 cases) and conventional ABG group(group B, 22 cases), and followed up for 12 months.The successful rate of bone graft and recovery of bone volumen between two groups after operation were compared. ResultsThe successful rate of operation in group A (82.8%) was higher than that in group B(50.0%) (P < 0.05).After 3, 6 and 12 month, the survival of graft in defect region in group A was higher than that in group B(P < 0.05).The survival of graft in defect region in two groups after 3 months were higher than that after 6 and 12 months(P < 0.01), and the difference of survival of graft in defect region bewteen 6 and 12 months in two groups were not statistically significant(P>0.05). ConclusionsFor patients with unilateral alveolar cleft, the modified alveolar bone grafting can effectively improve the survival rate of bone graft, and the recovery of bone mass obviously increases after operation.The postoperative bone resorption mainly occurs in the first 6 months of operation, and is basically stable at 6 to 12 months. -
表 1 2组病人不同时点植骨存活比比较(x±s;%)
分组 n 3个月 6个月 12个月 F P A组 22 69.67±7.63 52.45±9.17** 49.43±8.28** 46.37 < 0.01 B组 22 64.32±8.96 46.73±9.07** 43.81±8.58** 40.35 < 0.01 t — 2.13 2.08 2.21 — — P — < 0.05 < 0.05 < 0.05 — — q检验:与3个月时比较**P < 0.01  下载: 导出CSV
下载: 导出CSV
-
[1] 梁飞燕.齿槽嵴裂植骨术后植入骨位置的临床评价[J].现代口腔医学杂志, 2015, 29(2):90. [2] KINDELAN JD, NASHED RR, BROMIGE MR.Radiographic assessment of secondary autogenous alveolar bone grafting in cleft lip and palate patients[J].Cleft Palate Craniofac J, 1997, 34(3):195. [3] ABYHOLM FE, BERGLAND O, SEMB G.Secondary bone graffing of alveolar clefts.A surgical/orthodontic treatment enahling a non-prosthodontic.rehabilitation in cleft lip and palate patients[J].Scand J Plast Reconstr Surg, 1981, 15(2):127. [4] 杨超, 石冰.牙槽突裂植骨术的技术改进与初步评价[J].中国实用口腔科杂志, 2012, 5(6):327 [5] BERGLAND O.Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment[J].Cleft Palate J, 1986, 23(3):175. [6] BOYNE PJ, SANDS NR.Secondary bone grafting of residual alveolar and palatal clefts[J].J Oral Surg, 1972, 30(2):87. [7] 徐雪, 杨超, 刘坤.牙槽突裂治疗方法的研究进展[J].国际口腔医学杂志, 2016, 43(4):428. [8] 陈文革, 师坚强, 原杰.64层螺旋CT在先天性牙槽嵴裂植骨术中植骨量的临床研究[J].中国药物与临床, 2015, 15(6):799. [9] 倪国宇, 李红, 王义, 等.唇腭侧联合入路植骨术修复牙槽突裂的临床观察[J].中国美容整形外科杂志, 2017, 28(11):679. [10] 焦建军, 柴丛娜, 靳书滨, 等.先天性单侧完全性牙槽突裂患者植骨后上唇高度及鼻翼基底的改变[J].中国组织工程研究, 2017, 21(8):1246. [11] YANG CJ, PAN XG, QIAN YF.Impact of rapid maxillary expansion in unilateral cleft lip and palate patients after secondary alveolar bone grafting:review and case report[J].Oral Surg Oral Med Oral Pathol Oral Radiol, 2012, 114(1):e25. [12] VAN DER MEIJ VJ, BAART JA, PRAHL-ANDERSEN B, et al.Bone volume after secondary bone grafting in unilateral and bilateral clefts determined by computed tomography scans[J].Oral Surg Oral Med Oral Pathol Oral Radio Endod, 2001, 92(2):136. [13] SEMB G.Alveolar bone grafting[J].Front Oral Biol, 2012, 16:124. [14] 唐世杰, 石伦刚.牙槽突裂植骨吸收的原因及对策[J].中国实用口腔科杂志, 2012, 5(6):332. [15] 吴烨, 谢福平, 刘欢欢, 等.牙槽嵴裂手术修复技术改进的临床探讨[J].上海口腔医学, 2017, 26(3):281. [16] 杨超, 石冰, 刘坤.腭侧入路牙槽突裂植骨术的初步应用与评价[J].华西口腔杂志, 2013, 31(1):30. -

 点击查看大图
点击查看大图

图(2)表(1)
计量
- 文章访问数: 4488
- HTML全文浏览量: 2349
- PDF下载量: 12
- 被引次数: 0
