


-
乳腺癌在女性癌症中位居首位,与性成熟期提前、肥胖、不良情绪、生活作息不规律及膳食结构异常等因素有关,患病后无典型症状,部分病人就诊时疾病已发展至中晚期,不利于女性身心健康,甚至危及生命[1]。现今临床主要采取的疗法为手术切除法、内分泌法、放化疗法,又以改良根治术最为关键,但术后受多因素影响,伤口或术区的腔隙内积聚大量液体,出现区域积液,发生皮瓣波动的皮下积液现象等常见的并发症,发生率为6% ~40%,未及时处理可能引起伤口裂开、皮瓣坏死及肩关节活动障碍等。早期探寻影响皮下积液的因素很重要,便于提
-
收集我院2016-2019年接收的66例乳腺癌改良根治术病人,根据术式的不同,分为对照组(n=40)、干预组(n=26)。对照组年龄33~75岁,体质量指数18~30 kg/m2;伴有糖尿病9例,腋窝淋巴结阳性15例。干预组年龄37~76岁,体质量指数19~26 kg/m2;伴有糖尿病6例,腋窝淋巴结阳性11例。2组病人一般资料具有可比性。纳入标准:询问病人病史,结合体格检查、乳腺超声及病理检查,明确诊断为乳腺癌,符合手术指征者;术前向病人讲解手术方式,争取到病人同意,并于“知情同意书”上进行书面确认;经医院伦理委员会审核后,得到其准可。排除标准:并发其他恶性肿瘤;关键脏器机能障碍;免疫系统异常或凝血机能障碍;伤口大量出血;有手术禁忌证;术中或术后早期大出血;认知、精神障碍;中途退出研究者。
-
研究对象均由同一手术组完成手术操作,行规范性乳腺癌改良根治术,2组在处理腋窝、皮瓣方面存有显著差异。根据肿瘤情况在乳腺部位选择切口,距离肿瘤边缘≥3 cm,借助电刀在皮下层及乳腺浅筋膜间行皮瓣游离操作,留有薄层脂肪组织在皮瓣,将乳腺腺体、胸大肌筋膜切除至腋窝位置[5-6]。
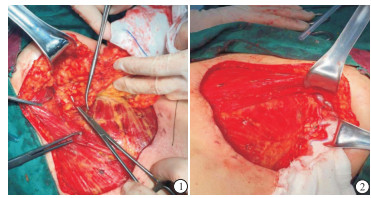
对照组:对腋窝Ⅰ、Ⅱ及Ⅲ组淋巴结行常规清扫操作,严格规范手术操作,钝性分离各组淋巴管道以及小血管,牢固结扎,减少淋巴漏及小血管出血,留存胸背、肩胛下与胸长神经处的神经与血管,随机选取部分病人在腋窝处填塞明胶海绵,交叉放置腋窝、胸壁引流管[7](见图 1~2)。
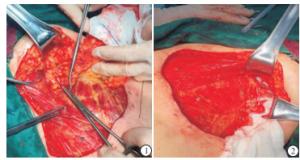
图 1~2 改良乳腺癌根治术(对照组)
干预组:行改进术,待完成对腋窝淋巴结的清扫,在对照组方法的基础上利用7号丝线缝合固定腋窝处皮瓣及胸壁,缝合点之间的距离是3~4 cm;在距皮肤创缘两侧中央部位皮瓣上,做减张性小切口,切开皮肤长0.5~1.0 cm多处小切口。根据皮缘张力大小,小切口可设计每侧3~5处(见图 3-4)。需要注意的是,不能将2根放置的引流管与创面边缘靠近,保持引流管长度适宜,确保引流通畅,预防术后发生包裹性积液的现象[8]。

图 3~4 腋下多点皮瓣固定及胸壁小切口减张(干预组)
术后对2组病人的皮瓣表面采用纱布块覆盖,接着通过弹力绷带实施加压包扎操作,引流管连通负压引流球,以此保障可顺畅引流。术后实时监测病人的病情,24 h内引出液体≤20 mL,将引流管拔除即可[9-10]。
-
临床指标:测定2组引流量、引流天数、皮下积液、切口感染、缺血坏死发生率。统计双方皮下积液发生数量,皮下积液Tejler标准如下:术后第5天起每日的胸壁或腋窝皮下引流量依然在30 mL以上,或者拔除引流管后第2天触摸手术部位皮下见波动感,抽出的穿刺液量在5 mL以上[4];引流管放置时间:自手术当日至最后一根引流管拔除的时间间隔;5 d引流量:是指术后5 d腋窝、胸壁2根引流管引流量之和;病人引流管拔出后无皮下积液、切口感染、缺血坏死等即可办理出院。
-
采用t检验、χ2检验和Fisher确切概率法。
-
干预组病人引流量、留管时间和住院时间均显著低于对照组(P < 0.01)(见表 1)。
分组 n 引流量/mL 留管时间/d 住院时间/d 干预组 26 353.42±130.86 8.81±1.96 11.77±2.18 对照组 40 511.98±170.38 10.65±2.86 13.10±2.67 t — 4.03 3.10* 2.12 P — < 0.01 < 0.01 < 0.05 *示t′值 表 1 2组5 d引流量、置管时间、住院时间比较(x±s)
-
干预组皮下积液发生率11.53%,低于对照组的37.50%(P < 0.05)(见表 2)。
分组 n 皮下积液 切口感染 缺血坏死 干预组 26 3(11.53) 2(7.69) 1(3.85) 对照组 40 15(37.50) 6(15.00) 3(5.00) χ2 — 5.35 0.25* 0.01* P — < 0.05 >0.05 >0.05 *示矫正χ2值 表 2 皮下积液、切口感染、缺血坏死发生率[n;百分率(%)]
-
对照组不同腋窝淋巴结情况、是否合并糖尿病的因素、是否应用明胶海绵术后发生皮下积液发生率差异均有统计学意义(P < 0.05);不同年龄段和体质量指数术后发生皮下积液发生率差异无统计学意义(P>0.05)(见表 3)。
临床因素 n 积液发生 χ2 P 腋窝淋巴结情况 阳性 15 9(60.00) 5.18 < 0.05 阳性阴性 25 6(24.00) 体质量指数/(kg/m2) < 25 29 10(34.48) 0.08* >0.05 ≥25 11 5(45.45) 合并糖尿病 是 9 7(77.78) 5.97* < 0.05 否 31 8(25.81) 年龄/岁 < 60 33 11(40.00) 0.57* >0.05 ≥60 7 4(16.67) 应用明胶海绵 是 22 5(22.73) 4.55 < 0.05 否 18 10(55.57) *示矫正χ2值 表 3 对照组乳腺癌临床因素与皮下积液发生的关系[n;百分率(%)]
-
干预组高危因素病人皮下积液发生率低于对照组(P < 0.05)(见表 4)。
高危因素 干预组 对照组 P 腋窝淋巴结阳性 9.09(1/11) 60.00(9/15) < 0.05* 合并糖尿病 16.67(1/6) 77.78(7/9) < 0.05* 未使用明胶海绵 15.38(2/13) 55.57(10/18) < 0.05* *示Fisher确切概率法 表 4 高危因素病人皮下积液发生率(%)
-
乳腺癌改良根治术后,病人发生皮下积液是指皮瓣与胸壁间并未完全愈合,存有腔隙导致液体蓄积, 具有较高发病率[11]。积液长期存在导致病人身心疼痛感增加,增加病人的痛苦,影响术后进一步治疗,对术后病情康复产生消极影响[12]。WATT-BOOLSEN等[13-14]通过分析积液中的成分后认为术后早期引流液体主要因为创面的炎性渗出, 而术后1周以后主要为淋巴液渗漏所致。ZIELINSKI等[15]指出年龄、腋窝淋巴结状态、是否合并糖尿病、体质量指数、是否术前化疗、切口类型、真皮下层组织厚度、是否电刀分离、是否弹力绷带加压包扎、是否使用生物胶等可能为术后皮下积液的高危因素。其中电刀使用情况、腋窝清扫对皮下积液影响较大,前哨淋巴结活检可减少皮下积液。
本研究采用腋下多点皮瓣固定及胸壁小切口减张方法处理腋窝及胸壁皮瓣,术中谨慎使用电刀,对淋巴管行规范结扎处理,避免淋巴漏的发生,结果显示干预组引流量较对照组少,引流时间较对照组短,皮下积液发生率低于对照组;对照组病人术后发生皮下积液与腋窝淋巴结情况、是否合并糖尿病及是否应用明胶海绵的因素有关,可能是腋窝淋巴结阳性病人,出现淋巴结转移后,阻碍淋巴液回流,由机体新增数量可观的淋巴管代偿导致;患有糖尿病时,病人伤口愈合能力不佳,血管收缩力下降,同样存在提高皮下积液发生率的可能性;医院明胶海绵具有多孔性,可吸收腋窝处积血积液,形成机械屏障,可减少渗出[16-18]。本研究发现皮下积液与年龄、体质量指数差异无统计学意义,与一些研究结果并不一致,一般来说体质量更大的病人,易发生脂肪液化的现象,对伤口愈合不利,血液循环障碍、血管功能差及伤口愈合缓慢等因素引起皮下积液[15],而本文病例数较少,病人年龄段多集中在50岁左右,体质量差异同样较小,后期我们需要做更多的研究。
本文结果还显示干预组高危因素病人皮下积液发生率亦明显低于对照组,说明干预组改进手术方式,将腋窝处皮瓣与胸壁缝合固定,创缘两侧皮肤做减张性小切口,是一种有效地降低皮下积液发生率,缩短拔管时间、住院时间的途径[19-20]。此外,进行手术时,应规范实施无菌操作,利用明胶海绵填塞腋窝,交叉放置腋窝胸壁淋巴管,弹力绷带加压操作,但应合理控制包扎松紧度,不可过紧,避免引起病人发生呼吸困难。由于淋巴管漏及术后皮瓣移动,导致创面渗出液体增多,若术后仅借助弹力绷带、制动等措施对淋巴漏及皮瓣移动并不能发挥预防措施,而腋窝皮瓣固定及明胶海绵填塞可有效封闭死腔,减少渗出,减张性小切口可减少皮肤张力,促进皮瓣与胸壁之间贴合,有效减少胸壁下积液,预防皮肤切缘坏死减少等风险,因此改进手术方式对降低皮下积液发生率具有积极重要的意义,具有临床可适应性,值得推广及应用。
腋下多点皮瓣固定及胸壁小切口减张改善乳腺癌改良根治术后皮下积液的有效性及安全性研究
Study on the efficacy and safety of multi-point axillary flap fixation and small incision reduction of chest wall in the improvement of subcutaneous hydrops after modified radical mastectomy
-
摘要:
目的探讨乳腺癌改良根治术中应用腋下多点皮瓣固定及胸壁小切口减张改善术后皮下积液的有效性及安全性,并对皮下积液相关致因进行分析。 方法收集66例乳腺癌改良根治术病人,根据手术方式的不同,分为对照组(n=40)和干预组(n=26)。对照组行常规腋窝淋巴结清扫,留置腋窝、胸壁2根引流管;干预组除了对照组所行治疗,增加缝合固定腋窝处皮瓣和胸壁,创缘两侧皮肤做减张性小切口。比较2组病人置管时间、住院时间及皮下积液等指标。 结果干预组病人引流量、留管时间、住院时间、皮下积液发生率及高危因素病人皮下积液发生率均显著低于对照组(P < 0.05~P < 0.01)。对照组不同腋窝淋巴结情况、是否合并糖尿病的因素、是否应用明胶海绵术后皮下积液发生率差异均有统计学意义(P < 0.05);不同年龄段和体质量指数术后发生皮下积液发生率差异均无统计学意义(P>0.05)。 结论乳腺癌改良根治术后发生皮下积液的因素包括腋窝淋巴结阳性、是否合并糖尿病及是否应用明胶海绵。改进手术方式对减少腋窝、胸壁皮下积液具有重要的意义。 Abstract:ObjectiveTo investigate the effectiveness and safety of multi-point axillary flap fixation and small incision reduction of chest wall in the improvement of subcutaneous hydrops after modified radical mastectomy, and analyze the related risk factors of subcutaneous effusion. MethodsA total of 66 patients treated with modified radical mastectomy were divided into the control group(n=40) and intervention group(n=26) according to the surgical methods.The control group was treated with the routine axillary lymph node dissection combined with retained two drainage tubes in the axillary and chest wall.The intervention group was treated with strengthening the suturing and fixing the axillary skin flap with chest wall combined with subtensive incision on both sides of the border on the basis of the control group.The time of catheterization, length of stay and subcutaneous effusion were compared between two groups. ResultsThe volume of drainage, indwelling catheter time, length of stay and incidence rate of subcutaneous hydrops in intervention group were significantly lower than those in control group(P < 0.05 to P < 0.01).In the control group, the differences of the incidence rates of subcutaneous hydrops in patients with different axillary lymph nodes, diabetes mellitus and gelfoam application were statistically significant(P < 0.05).After surgery, there was no statistical significance in the incidence rate of subcutaneous hydrops in different age and body mass index in control group(P>0.05). ConclusionsThe positive axillary lymph nodes, diabetes mellitus and gelatin spongee use are the influencing factors of subcutaneous hydrops.The improved surgical method is of great significance to reduce subcutaneous effusion in axillary and chest wall. -
Key words:
- breast neoplasms /
- modified radical mastectomy /
- subcutaneous effusion /
- small incision /
- flap fixation
-
表 1 2组5 d引流量、置管时间、住院时间比较(x±s)
分组 n 引流量/mL 留管时间/d 住院时间/d 干预组 26 353.42±130.86 8.81±1.96 11.77±2.18 对照组 40 511.98±170.38 10.65±2.86 13.10±2.67 t — 4.03 3.10* 2.12 P — < 0.01 < 0.01 < 0.05 *示t′值  下载: 导出CSV
下载: 导出CSV
表 2 皮下积液、切口感染、缺血坏死发生率[n;百分率(%)]
分组 n 皮下积液 切口感染 缺血坏死 干预组 26 3(11.53) 2(7.69) 1(3.85) 对照组 40 15(37.50) 6(15.00) 3(5.00) χ2 — 5.35 0.25* 0.01* P — < 0.05 >0.05 >0.05 *示矫正χ2值
下载: 导出CSV
表 3 对照组乳腺癌临床因素与皮下积液发生的关系[n;百分率(%)]
临床因素 n 积液发生 χ2 P 腋窝淋巴结情况 阳性 15 9(60.00) 5.18 < 0.05 阳性阴性 25 6(24.00) 体质量指数/(kg/m2) < 25 29 10(34.48) 0.08* >0.05 ≥25 11 5(45.45) 合并糖尿病 是 9 7(77.78) 5.97* < 0.05 否 31 8(25.81) 年龄/岁 < 60 33 11(40.00) 0.57* >0.05 ≥60 7 4(16.67) 应用明胶海绵 是 22 5(22.73) 4.55 < 0.05 否 18 10(55.57) *示矫正χ2值
下载: 导出CSV
表 4 高危因素病人皮下积液发生率(%)
高危因素 干预组 对照组 P 腋窝淋巴结阳性 9.09(1/11) 60.00(9/15) < 0.05* 合并糖尿病 16.67(1/6) 77.78(7/9) < 0.05* 未使用明胶海绵 15.38(2/13) 55.57(10/18) < 0.05* *示Fisher确切概率法
下载: 导出CSV
-
[1] 中国抗癌协会乳腺癌专业委员会.中国抗癌协会乳腺癌诊治指南与规范(2017年版)[J].中国癌症杂志, 2017, 27(9):695. [2] 黄婷, 张超杰, 谢敬雄, 等.乳腺癌术后皮下积液的危险因素分析及相关防治方法[J].国际外科学杂志, 2017, 44(9):607. [3] 梅俊, 易茂林, 彭程程.超声刀联合腋窝处皮肤外固定预防乳腺癌改良根治术后皮下积液的效果分析[J].安徽医药, 2018, 22(11):2162. [4] TJLER G, ASPEGREN K.Complications andhospital stayaftersurgery for breast cancer:a prospective studyof 385 patients[J]. Br J Surg, 1985, 72(7):542. doi: 10.1002/bjs.1800720714 [5] MADDOX WA, CARPENTER JT, LAWS HL, et al. A randomized prospective trial ofradical(Halsted) mastectomyversus modified radical mastectomy in 311 breast cancer patients[J]. Ann Surg, 1983, 198(2):207. doi: 10.1097/00000658-198308000-00016 [6] TURNER L, SWINDELL R, BELL WG, et al.Radical versus modified radical mastectomy for breast cancer[J]. Ann R Coll Surg Engl, 1981, 63(4):239. [7] 周志升, 朱大江, 陈金桃, 等.双管持续中心负压引流能有效防止乳腺癌改良根治术后皮下积液[J].华夏医学, 2019, 32(2):90. [8] 国长军, 黄宣东.减张性小切口预防乳腺癌术后创缘皮肤坏死(附15例报告)[J].中国临床医生, 2001, 29(4):34. [9] 朱辉琴.浅论行乳腺癌根治术的病人发生术后皮下积液的原因及治疗方法[J].当代医药论丛, 2017, 15(22):157. [10] 刘祥伟, 曲延玉, 陈德滇.乳腺癌病人术后并发淋巴水肿的危险因素分析[J].国际肿瘤学杂志, 2018, 45(5):262. [11] 何玲, 胡玲嘉, 仇爱峰.复合护理干预对乳腺癌病人术后淋巴水肿发生率及生活质量的影响[J].徐州医科大学学报, 2018, 40(12):845. [12] 邵静涛, 方仁桂, 王学军, 等.术后有氧运动和心理干预对乳腺癌病人术后康复的临床价值[J].中国基层医药, 2017, 24(5):771. [13] WATT-BOOLSEN VB, NIELSEN J, JENSEN S.Postmastectomyseroma.A study of the nature and origin of seroma after mastectomy[J]. Dan Med Bull, 1989, 36(5):487. [14] TADYCH K, DONEGAN WL.Postmastectomy seromas and wound drainage[J]. Surg Gynecol Obstet, 1987, 165(6):483. [15] ZIELINSKI J, JAWORSKI R, IRGA N, et al.Analysis of selected factors influencing seroma formation in breast cancer patients undergoing mastectomy[J]. Archives of Med Sci, 2013, 9(1):86. [16] SAKKARY MA.The value of mastectomy flap fixation in reducing fluid drainage and seroma formation in breast cancer patients[J]. World J Surg Oncol, 2012, 10:8. doi: 10.1186/1477-7819-10-8 [17] ZHOU Y, ZHANG X, GU C.et al.Influence of diabetes mellitus on mortality in breast cnacer patients[J]. ANZ J Sury, 2015, 85(12):972. doi: 10.1111/ans.12877 [18] 张彦武, 李庆辉, 严文君, 等.明胶海绵在预防乳腺癌术后腋窝淋巴瘘中的应用[J].中国普通外科杂志, 2015, 24(5):763. [19] 齐小梅, 苏小君, 梁燕, 等.外科方法处理乳腺癌合并糖尿病病人术后皮下积液的临床效果[J].局解手术学杂志, 2019, 28(4):332. [20] TEN WOLDE B, VAN DEN WILDENBERG FJH, KEEMERS-GELS ME, et al.Quilting prevents seroma formation following breast cancer surgery:closing the dead space by quilting prevents seroma following axillary lymph node dissection and mastectomy[J]. Ann Surg Oncol, 2014, 21(3):802. doi: 10.1245/s10434-013-3359-x -

 点击查看大图
点击查看大图
图(2)表(4)
计量
- 文章访问数: 4663
- HTML全文浏览量: 2469
- PDF下载量: 37
- 被引次数: 0
