

-
肝硬化食管胃静脉曲张破裂出血(esophagogastric variceal bleeding, EVB)是肝硬化病人最为严重的并发症,发生率为30%~40%,死亡率高达40%,每年5%~10%的肝硬化病人发展为食管静脉曲张(esophageal varices, EV)[1]。电子胃镜是诊断EV的最直观及有效的检查,但该检查为侵入性检查,很多病人耐受性及依从性差,且指南推荐肝硬化病人定期复查胃镜[2],这无疑给病人带来了巨大的精神压力,因此探索发现非侵入性检查方法尤为迫切。本研究通过对血小板计数(platelet count, PC)、脾长径(spleen longitudinal diameter, SD)、血小板计数与脾长径比值(platelet count/spleen longitudinal diameter ratio,PC/SD)、FIB-4指数四项指标的综合评估,旨在探讨各指标对EV的诊断价值。现作报道。
-
选择2018年10月至2019年10月我科门诊及住院部接诊的肝硬化病人134例,男97例,女36例,年龄30~74岁,平均年龄(52.00±10.73)岁,均符合2019年《肝硬化诊治指南》的诊断标准[3];病因分布:乙型肝炎95例(70.9%)、酒精性肝炎10例(7.5%)、乙型肝炎合并酒精型肝炎13例(9.7%)、丙型肝炎2例(1.5%)、乙型肝炎合并丙型肝炎1例(0.7)、原发性胆汁性胆管炎4例(3.0%)、自身免疫性肝炎1例(0.7%),隐源性肝硬化8例(6.0%)。排除标准:(1)门静脉血栓形成;(2)既往使用β受体阻滞剂;(3)行脾切除手术;(4)行EV套扎或硬化或组织胶注射术;(5)经颈静脉肝内门体分流术;(6)消化道出血急性期。本研究经过我院伦理委员会批准实施,所有受试者均知情同意,并签署知情同意书。将134例病人按照是否合并EV分为2组,其中无EV组38例,男27例,女11例,年龄(50.84±11.38)岁;EV组96例,男70例,女25例,年龄(52.46±10.49)岁。2组间年龄、性别差异均无统计学意义(P>0.05)。EV组96例病人中,红色征(red color sign, RC)(+)59例,RC(-)37例。
-
受试者清晨空腹行肝脾彩色多普勒超声检查及采集外周静脉血,血清肝功能丙氨酸氨基转移酶(ALT)、天门冬氨酸氨基转移酶(AST)、白蛋白(ALB)采用BECKMAN COULTER AU5800型全自动生化分析仪进行检测,试剂由宁波瑞源生物有限公司提供;血白细胞(WBC)、PC使用日本Sysmex XE-5000型全自动血球分析仪检测,试剂为Sysmex配套试剂;凝血酶原时间(PT)、国际标准化比值(INR)使用Sysmex CS-5100型全自动凝血分析仪检测,试剂由上海希森美康医用电子有限公司提供;检测过程均严格按照说明书进行。胃镜检查使用PENTAX-EPK5000或OLYMPUS-CV290型号内镜由消化内镜室3年以上资质的医生执行,参照《肝硬化门静脉高压食管胃静脉曲张出血的防治指南》的诊断标准[2]作出诊断。入组病人血液学及彩色多普勒超声检查均在胃镜检查前后1周内进行,分别计算出Child-Pugh评分及FIB-4指数。
-
采用t(或t′)检验,以胃镜检查结果为金标准绘制受试者工作特征曲线(ROC曲线),计算曲线下面积(AUC)、最佳界值及相应的敏感度、特异度。AUC在0.5~0.7准确性较低,0.7~0.9有一定的准确性,0.9以上为准确性较高,以敏感度和特异度之和最大时为最佳临界值。
-
EV组PC、WBC、PC/SD均低于非EV组,SD、FIB-4、Child-Pugh评分、PT均高于非EV组,差异有统计学意义(P < 0.05~P < 0.01)(见表 1)。
指标 非EV组(n=38) EV组(n=96) t P ALT/(U/L) 94.87±176.78 39.56±26.96 1.92* >0.05 AST/(U/L) 82.39±113.31 53.70±35.06 1.53* >0.05 ALB/(g/L) 34.08±7.22 31.95±6.25 1.70 >0.05 CR/(mmol/L) 64.32±14.77 66.05±28.74 0.46* >0.05 PC/(×109/L) 122.00±53.80 70.39±45.53 5.61 < 0.01 WBC/(×109/L) 4.50±1.52 3.65±2.49 2.41* < 0.05 PT/s 14.36±2.39 15.50±2.92 2.06 < 0.05 INR 1.31±0.24 1.39±0.28 1.43 >0.05 SD/mm 117.58±26.20 154.50±35.11 6.64* < 0.01 Child-Pugh评分/分 7.19±2.05 7.96±1.98 1.99 < 0.05 FIB-4 4.73±3.41 8.88±9.49 3.73* < 0.01 PC/SD 1.15±0.63 0.51±0.43 5.74* < 0.01 *示t′值 表 1 临床指标的比较(x±s)
-
ROC曲线分析显示,PC、SD、PC/SD、FIB-4对EV预测的AUC均>0.7, PT、ALT对EV预测的AUC均 < 0.7。提示PC、SD、PC/SD、FIB-4对EV均有一定的诊断价值,PT、ALT对EV诊断的准确性较低;且SD、PC/SD值对预测EV具有相似的诊断效能(见表 2)。
指标 AUC 临界值 95%CI SE P 灵敏度 特异度 PC 0.781 96.50 0.692~0.871 0.046 < 0.01 0.833 0.711 SD 0.811 140.50 0.734~0.889 0.040 < 0.01 0.667 0.816 PC/SD 0.811 0.85 0.726~0.897 0.044 < 0.01 0.875 0.658 FIB-4 0.715 4.05 0.613~0.817 0.052 < 0.01 0.781 0.632 PT 0.611 14.75 0.497~0.725 0.058 >0.05 0.568 0.676 ALT 0.611 40.50 0.500~0.722 0.057 < 0.05 0.646 0.605 表 2 PC、SD、PC/SD、FIB-4单独预测EV的比较
-
PC/SD与SD联合对EV预测的AUC为0.822,灵敏度85.4%,特异度71.1%;PC/SD与PC联合对EV预测的AUC为0.811,灵敏度87.5%,特异度65.8%;PC/SD比值与FIB-4对EV预测的AUC为0.811,灵敏度87.5%,特异度65.8%(见表 3)。
指标 AUC 95%CI SE P 灵敏度 特异度 PC/SD+SD 0.822 0.743~0.900 0.040 < 0.01 0.854 0.711 PC/SD+PC 0.811 0.726~0.897 0.044 < 0.01 0.875 0.658 PC/SD+FIB-4 0.811 0.726~0.897 0.044 < 0.01 0.875 0.658 表 3 PC/SD分别与SD、PC、FIB-4联合预测EV的比较
-
EV组按是否合并RC分为RC(+)及RC(-)组,比较2组病人的临床资料,结果显示,RC(+)组年龄小于RC(-)组,SD大于RC(-)组,差异有统计学意义(P < 0.05和P < 0.01)(见表 4)。SD对预测EV组病人中RC(+)的AUC为0.705,临界值为151 min,灵敏度为66.1%,特异度为64.5%。SD对EV病人RC的预测有一定的准确性(见图 1)。
指标 RC(-)(n=59) RC(+)(n=37) t P 年龄/岁 55.14±9.97 50.78±10.54 2.04 < 0.05 ALT/(U/L) 45.22±36.39 36.02±18.31 1.64* >0.05 AST/(U/L) 60.19±38.38 49.63±32.48 1.44 >0.05 ALB/(g/L) 31.56±6.12 32.19±6.37 -0.47 >0.05 CR/(mmol/L) 62.81±11.76 68.10±35.48 -0.87 >0.05 PC/(×109/L) 71.11±43.91 69.93±46.88 0.12 >0.05 WBC/(×109/L) 3.13±1.35 3.97±2.96 -1.60 >0.05 PT/s 12.27±2.87 15.65±2.97 -0.61 >0.05 INR 1.38±0.28 1.39±0.29 -0.25 >0.05 SD/mm 139.22±29.98 164.08±34.91 -3.58 < 0.01 Child评分/分 8.00±2.32 7.93±1.76 0.16 >0.05 FIB-4 9.83±8.65 8.29±10.00 0.78 >0.05 PC/SD 0.56±0.41 0.48±0.45 0.95 >0.05 *示t′值 表 4 EV组病人有无RC的临床特征分析(x±s)
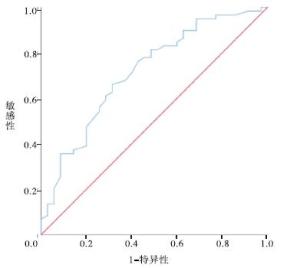
图 1 EV组RC(+)病人的ROC曲线
-
EVB是肝硬化病人的急危重症,严重威胁病人生命,因此早期发现EV是肝病科医生的基础工作,胃镜被临床广泛用于EV的筛查,但其接受度低,可重复性差,因此寻求非侵入性指标对EV的诊断具有十分重要的意义。
肝硬化EV的程度与门静脉高压程度呈正相关,国内外对EV非侵入性检查方法的研究多集中在门静脉高压相关指标。本研究显示PC与EV的发生呈负相关,SD与EV的发生呈正相关,这与MONTASSER等[4-5]的研究结果一致。肝硬化门静脉高压病人,脾静脉回流阻力增大,同时肠道抗原物质经门-体侧支循环,被脾摄取,刺激脾脏单核巨噬细胞增生,形成脾大和脾亢,因此PC、SD在理论上可反映门静脉高压的程度。本研究结果显示PC/SD、SD的诊断效能均优于PC,PC单独诊断EV的AUC为0.781。以往研究[5-7]结果显示,诊断EV的PC临界值不一致,且灵敏度均不高,提示PC对EV的诊断性能均不满意,考虑PC易受门静脉高压以外的因素影响,如肝硬化病因、感染、药物、血液系统疾患、血小板生成素的合成等,因此,PC独立预测EV的价值有限。
肝硬化病人PC/SD比值常降低,其原因为肝硬化病人脾脏增大,同时脾功能亢进,肝脏合成促血小板生成素减少以及血小板抗体增多等导致的血小板生成减少、破坏增多[8]。PC/SD最早在2003年首先提出用于预测肝硬化EV[9],目前,已有大量研究[10-12]证实,PC/SD可作为肝硬化病人EV发生情况的预测因子,但关于其最佳预测值、灵敏度、特异度的研究国内外报道不一,有研究[12]认为其原因可能与人种不同有关,国内目前也无统一的标准。本文提示PC/SD低于0.85时,对EV的预测具有较高的敏感性。FIB-4是预测肝纤维化的良好指标[13],近年也单独或与其他非侵入性模型联合用于EV的诊断。FIB-4与ALT、AST值相关,而不同病因及肝炎活动与否状态下ALT、AST值不尽相同,且常受采血前保肝降酶类药物使用的影响。有研究[14]认为FIB-4与EV的发生相关,但对EVB的预测价值较低。本文FIB-4预测EV的截断值为4.05,与王报等[6]的研究结果相似,但其相应的AUC、灵敏度、特异度均不高,提示FIB-4对EV的预测价值较低。
本研究中PC/SD、SD对EV预测的AUC均为0.811,提示二者的诊断效能相仿,而XU等[15]纳入236例血吸虫性肝硬化病人的研究提示PC/SD比单用SD诊断EV的准确性显著提高,屈淑平等[7]纳入均为乙肝肝硬化病人的研究中,PC/SD较SD对于预测EV也显示出较好的优越性,本文入组的病例病因学多样,分析可能原因为在不同病因下PC、SD变化的程度不同,因此,PC/SD及SD值对不同病因所致肝硬化的EV诊断效能仍需进一步分类探讨。本研究结果提示,PC/SD、SD对EV的诊断效能均优于PC及FIB-4,PC/SD分别与FIB-4、PC联合检测未能提高EV的诊断效能,而PC/SD与SD联合检测增加了EV的诊断效能,因此临床上PC/SD、SD二者联合检测可减少部分EV病人漏诊。
RC是相应的静脉压力较高,导致局部血管壁明显薄弱所致,与脾淤血性肿大同为门静脉高压的表现,EVB的主要危险因素之一是RC[16],而RC的相关危险因素目前报道不多。本研究结果提示,SD是EV病人RC的独立危险因素,SD>151 mm时,对EV病人RC预测的灵敏度为70.5%,有助于临床采取有效的药物干预或进一步行内镜治疗,并对EV病人可能的突发消化道出血事件作出预判,促进有效的医患沟通;但其预测RC的AUC、灵敏度及特异度均不高,且本研究为单中心研究,仍需多中心研究进一步证实。
综上所述,PC、SD、PC/SD、FIB-4对EV的诊断均有一定的价值,PC/SD、SD联合可增加EV的诊断效能,这些非侵入性指标虽不能取代胃镜,但有助于减少部分胃镜检查,值得临床推广,特别是对胃镜检查有心理障碍或禁忌的病人,通过上述指标的筛查,有望得到及时有效的预防和治疗。
PC、SD、PC/SD、FIB-4对肝硬化食管静脉曲张的诊断价值
Diagnostic value of PC, SD, PC/SD and FIB-4 in cirrhotic esophageal varices
-
摘要:
目的评估脾长径(SD)、血小板计数(PC)、血小板计数/脾长径比值(PC/SD)、FIB-4指数预测肝硬化食管静脉曲张(esophageal varices,EV)的临床价值。 方法收集134例肝硬化病人的临床资料,均行胃镜检查明确食管胃底静脉曲张情况,按有无EV分为EV组及非EV组,EV组病人按照是否合并红色征(RC)分为RC(+)组及RC(-)组,评价PC、SD、PC/SD、FIB-4等四项指标对EV的诊断效能及分析RC的影响因素。 结果EV组PC、白细胞计数、PC/SD均低于非EV组,SD、FIB-4、Child-Pugh评分、凝血酶原时间均高于非EV组,差异有统计学意义(P < 0.05~P < 0.01);PC、SD、PC/SD、FIB-4对EV预测的受试者工作曲线下面积分别为0.781、0.811、0.811、0.715;SD、PC/SD联合对于EV预测的曲线下面积为0.822,灵敏度为85.4%,特异度为71.1%;RC(+)组年龄小于RC(-)组,SD大于RC(-)组,差异有统计学意义(P < 0.05和P < 0.01);SD对预测EV组病人中RC的曲线下面积为0.705,临界值151,灵敏度66.1%,特异度64.5%。 结论PC、SD、PC/SD、FIB-4对EV的预测均有一定的临床价值,PC/SD、SD联合能较好地预测EV;SD是肝硬化EV病人RC的独立危险因素。 Abstract:ObjectiveTo investigate the clinical value of spleen longitudinal diameter(SD), platelet count(PC), PC/SD and FIB-4 index in predicting the cirrhotic esophageal varices(EV). MethodsThe clinical data of 134 patients with cirrhosis were collected.The esophageal varices in all patients were examined using gastroscopy.According to the presence or absence of EV, the patients were divided into the EV group and non-EV group, and the EV group was subdivided into the RC (+) group and RC (-) group according to the red color sign(RC) The diagnostic efficacy of PC, SD, PC/SD and FIB-4 in EV were evaluated, and the influencing factors of RC was analyzed. ResultsThe PC, WBC and PC/SD in EV group were lower than those in non-EV group, and the SD, FIB-4, Child-Pugh score and PT in EV group were higher than those in non-EV group(P < 0.05 to P < 0.01).The areas under the curve predicted by PC, SD, PC/SD and FIB-4 for EV were 0.781, 0.811, 0.811 and 0.715, respectively.The area under the curve predicted by SD and PC/SD for EV was 0.822, the sensitivity was 85.4%, and the specificity was 71.1%.The age in RC (+) group was less than that in RC (-) group, and the SD in RC (+) group was greater than that in RC (-) group(P < 0.05 and P < 0.01).The area under the curve of SD for predicting RC in EV group was 0.705, the cutoff value was 151, the sensitivity was 66.1% and the specificity was 64.5%. ConclusionsThe PC, SD, PC/SD and FIB-4 have certain clinical value in predicting EV.The combination of PC/SD and SD can better predict.The SD is an independent risk factor for RC in patients with cirrhotic EV. -
Key words:
- cirrhosis /
- esophageal varices /
- spleen longitudinal diameter /
- platelet count /
- FIB-4
-
表 1 临床指标的比较(x±s)
指标 非EV组(n=38) EV组(n=96) t P ALT/(U/L) 94.87±176.78 39.56±26.96 1.92* >0.05 AST/(U/L) 82.39±113.31 53.70±35.06 1.53* >0.05 ALB/(g/L) 34.08±7.22 31.95±6.25 1.70 >0.05 CR/(mmol/L) 64.32±14.77 66.05±28.74 0.46* >0.05 PC/(×109/L) 122.00±53.80 70.39±45.53 5.61 < 0.01 WBC/(×109/L) 4.50±1.52 3.65±2.49 2.41* < 0.05 PT/s 14.36±2.39 15.50±2.92 2.06 < 0.05 INR 1.31±0.24 1.39±0.28 1.43 >0.05 SD/mm 117.58±26.20 154.50±35.11 6.64* < 0.01 Child-Pugh评分/分 7.19±2.05 7.96±1.98 1.99 < 0.05 FIB-4 4.73±3.41 8.88±9.49 3.73* < 0.01 PC/SD 1.15±0.63 0.51±0.43 5.74* < 0.01 *示t′值  下载: 导出CSV
下载: 导出CSV
表 2 PC、SD、PC/SD、FIB-4单独预测EV的比较
指标 AUC 临界值 95%CI SE P 灵敏度 特异度 PC 0.781 96.50 0.692~0.871 0.046 < 0.01 0.833 0.711 SD 0.811 140.50 0.734~0.889 0.040 < 0.01 0.667 0.816 PC/SD 0.811 0.85 0.726~0.897 0.044 < 0.01 0.875 0.658 FIB-4 0.715 4.05 0.613~0.817 0.052 < 0.01 0.781 0.632 PT 0.611 14.75 0.497~0.725 0.058 >0.05 0.568 0.676 ALT 0.611 40.50 0.500~0.722 0.057 < 0.05 0.646 0.605
下载: 导出CSV
表 3 PC/SD分别与SD、PC、FIB-4联合预测EV的比较
指标 AUC 95%CI SE P 灵敏度 特异度 PC/SD+SD 0.822 0.743~0.900 0.040 < 0.01 0.854 0.711 PC/SD+PC 0.811 0.726~0.897 0.044 < 0.01 0.875 0.658 PC/SD+FIB-4 0.811 0.726~0.897 0.044 < 0.01 0.875 0.658
下载: 导出CSV
表 4 EV组病人有无RC的临床特征分析(x±s)
指标 RC(-)(n=59) RC(+)(n=37) t P 年龄/岁 55.14±9.97 50.78±10.54 2.04 < 0.05 ALT/(U/L) 45.22±36.39 36.02±18.31 1.64* >0.05 AST/(U/L) 60.19±38.38 49.63±32.48 1.44 >0.05 ALB/(g/L) 31.56±6.12 32.19±6.37 -0.47 >0.05 CR/(mmol/L) 62.81±11.76 68.10±35.48 -0.87 >0.05 PC/(×109/L) 71.11±43.91 69.93±46.88 0.12 >0.05 WBC/(×109/L) 3.13±1.35 3.97±2.96 -1.60 >0.05 PT/s 12.27±2.87 15.65±2.97 -0.61 >0.05 INR 1.38±0.28 1.39±0.29 -0.25 >0.05 SD/mm 139.22±29.98 164.08±34.91 -3.58 < 0.01 Child评分/分 8.00±2.32 7.93±1.76 0.16 >0.05 FIB-4 9.83±8.65 8.29±10.00 0.78 >0.05 PC/SD 0.56±0.41 0.48±0.45 0.95 >0.05 *示t′值
下载: 导出CSV
-
[1] NICOLÁS M, ANTONIO R, FRANCISCO T, et al.Liver stiffness predicts variceal bleeding in HIV/HCV-coinfected patients with compensated cirrhosis[J].AIDS (London, England), 2017, 31(4):493. doi: 10.1097/QAD.0000000000001358 [2] 徐小元, 丁惠国, 贾继东, 等.肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J].临床肝胆病杂志, 2016, 32(2):203. [3] 徐小元, 丁惠国, 李文刚, 等.肝硬化诊治指南[J].临床肝胆病杂志, 2019, 35(11):2408. [4] MONTASSER MF, ABDELLA HM, SAMY AH.Evaluation of venous ammonia level, splenic longitudinal diameter, portal vein and splenic vein diameters as non-invasive indicators for the presence of portosystemic collaterals in egyptian cirrhotic patients[J].O J Gas, 2014, 4(6):265. [5] 杨炜炜, 杨建华.血小板计数预测肝硬化病人食管静脉曲张发生风险的探讨[J].实用临床医药杂志, 2018, 22(19):101. [6] 王报, 牛俊奇.PLT计数、FIB-4、APRI与肝硬化食管静脉曲张发生及严重程度的相关性分析[J].临床肝胆病杂志, 2018, 34(1):84. [7] 屈淑平, 刘韵, 杨平华, 等.血小板/脾双径评估乙型肝炎肝硬化肝癌病人食管静脉曲张的研究[J].肝脏, 2015, 20(8):597. doi: 10.3969/j.issn.1008-1704.2015.08.006 [8] 孙强, 郑正.门静脉高压断流术后血小板计数变化与肝功能的关系[J].蚌埠医学院学报, 2014, 39(4):487. [9] GIANNINI E, BOTTA F, BORRO P, et al.Platelet count/spleen diameter ratio:proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis.[J].Gut, 2003, 52(8):1200. doi: 10.1136/gut.52.8.1200 [10] 李金辉, 陈翔, 颜秀娟, 等.血小板计数与脾脏长径比值预测慢性乙型肝炎肝硬化食管静脉曲张的临床研究[J].胃肠病学, 2017, 22(4):214. [11] GONZÁLEZ-OJEDA A, CERVANTES-GUEVARA G, CHÁVEZ-SÁNCHEZ M, et al.Platelet count/spleen diameter ratio to predict esophageal varices in Mexican patients with hepatic cirrhosis[J].World J Gastroentero, 2014, 20(8):207 [12] MAKAREM MAAE, SHATAT ME, SHAKER Y, et al.Platelet count/bipolar spleen diameter ratio for the prediction of esophageal varices:The special Egyptian situation:Noninvasive prediction of esophageal varices[J].Hepat Mon, 2011, 11(4):278. [13] YEN Y, KUO F, KEE K, et al.APRI and FIB-4 in the evaluation of liver fibrosis in chronic hepatitis C patients stratified by AST level[J].PLoS One, 2018, 13(6):e199760. [14] 王晓彤.无创肝纤维化指标对乙型肝炎肝硬化食管静脉曲张的评估[C].中国中西医结合学会传染病专业委员会.全国第6届中西医结合传染病学术会议论文汇编.中国中西医结合学会传染病专业委员会: 中国中西医结合学会, 2015: 113. [15] XU X, XU C, DAI J, et al.Ratio of platelet count/spleen diameter predicted the presence of esophageal varices in patients with schistosomiasis liver cirrhosis[J].Eur J Gastroen Hepat, 2016, 28(5):588. doi: 10.1097/MEG.0000000000000584 [16] 彭湃澜, 周翔禹.肝硬化食管胃底静脉曲张破裂出血的危险因素及预后分析[J].实用临床医药杂志, 2016, 20(9):171. -

 点击查看大图
点击查看大图

图(1)表(4)
计量
- 文章访问数: 4183
- HTML全文浏览量: 1922
- PDF下载量: 5
- 被引次数: 0
