

-
原发性甲状旁腺肿瘤主要包括甲状旁腺腺瘤、甲状旁腺囊肿和甲状旁腺癌。由于甲状旁腺在解剖位置上紧邻于甲状腺后方,且肿瘤生长速度缓慢,临床表现多样,常被误诊为甲状腺肿瘤从而延误治疗。超声检查是诊断及鉴别诊断甲状旁腺肿瘤的重要方法之一[1]。然而,受限于超声医生经验水平,甲状旁腺肿瘤彩色多普勒超声诊断和鉴别诊断准确率仍然有待提高。我们对80例甲状旁腺肿瘤病人的彩色多普勒超声图像特点和临床特征进行分析,以期为甲状旁腺肿瘤诊断和鉴别诊断提供参考。现作报道。
-
回顾性分析2005年1月至2020年4月我院手术治疗的甲状旁腺肿瘤病人80例,男25例,女55例;年龄18~77岁;均经病理诊断;甲状旁腺腺瘤69例(腺瘤组),甲状旁腺癌4例(癌组),甲状旁腺囊肿7例(囊肿组),其中3例甲状旁腺腺瘤病人为双侧甲状旁腺腺瘤。
-
采用Phlips IU-22型及Toshiba apolo 500型彩色多普勒超声诊断仪,线阵探头频率7~12 MHz。检查时病人头部后仰,充分显露颈部区域,上至下颌角,下至胸骨上窝,左右达颈总动脉两侧进行纵、横、斜多方位扫查,取肿块最大切面测量其长轴径和短轴径,观察并记录其形态、边界、边缘、内部回声和后方回声,多普勒彩超检测肿块内部及周边血流情况,保存图像。此外,收集研究对象临床病史及实验室检查指标结果,包括血钙、血磷、血清碱性磷酸酶(ALP)、血清甲状旁腺素(PTH)等。
-
采用方差分析、q检验、χ2检验及Fisher′s确切概率法。
-
3组病人年龄、性别间差异均无统计学意义(P>0.05)(见表 1)。
分组 n 年龄(x±s)/岁 男 女 腺瘤组 69 49.81±13.96 21(30.43) 48(69.57) 囊肿组 7 47.71±13.01 2(28.57) 5(71.43) 癌组 4 48.25±11.32 2(50.00) 2(50.00) F — 0.09 — P — >0.05 >0.05* MS组内 — 190.285 — *示Fisher′s确切概率法 表 1 不同类型甲状旁腺肿瘤病人年龄和性别比较[n; 百分率(%)]
-
腺瘤组病人临床症状以单纯肾结石居多(9/69,13.04%),其后依次为骨关节炎症状(8/69,11.59%)、骨关节炎症状合并肾结石(8/69,11.59%)、血钙异常升高(7/69,10.14%)、颈部包块(7/69,10.14%)、颈部包块合并肾结石(4/69,5.80%)、胃肠道症状(4/69,5.80%)、血钙异常升高及肾结石(2/69,2.90%)、胃肠道症状和肾结石(2/69,2.90%)、心脏疾病症状(2/69,2.90%)、同时伴有心脏疾病症状、血钙异常升高、骨关节炎症状及肾结石症状(2/69,2.90%)、低钾血症和肾结石(1/69,1.45%)、血钙异常升高和低钾血症(1/69,1.45%)、心脏疾病症状伴肾结石(1/69,1.45%)、呼吸系统症状(1/69,1.45%),其余10例为体检时发现,无明显临床症状。癌组病人4例,其中1例表现为颈部包块,1例表现为颈部包块和肾结石,2例表现为胃肠道症状和肾结石。囊肿组病人7例,临床表现均表现为颈部包块。
-
腺瘤组和癌组病人血磷水平均低于囊肿组(P < 0.05),腺瘤组病人血钙和ALP水平均高于囊肿组(P < 0.05)(见表 2)。此外,共有55例甲状旁腺腺瘤病人检测了血清中PTH水平,平均水平为380.00(165.52, 875.1) ng/L。
分组 n 钙/(mmol/L) 磷(mmol/L) ALP
[M50(M25, M75)]/(ng/L)腺瘤组 69 3.01±0.76 0.78±0.26 174.00(108.00, 427.00) 囊肿组 7 2.31±0.10* 1.24±0.20* 51.00(37.00, 69.00)* 癌组 4 2.71±0.38 0.64±0.09# — F — 3.22 11.65 3.97△ P — <0.05 <0.01 <0.01 MS组内 — 0.516 0.063 — q检验:与腺瘤组比较*P < 0.05;与囊肿组比较#P < 0.05;△示uc值 表 2 不同类型甲状旁腺肿瘤病人血钙、磷和ALP水平比较(x±s)
-
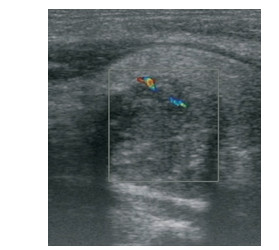
不同类型甲状旁腺肿瘤病人超声定位准确率差异有统计学意义(P < 0.01),以腺瘤组最高,为79.71%。不同类型甲状旁腺肿瘤病人肿瘤上下径、左右径、前后径间差异均有统计学意义(P < 0.01),其中腺瘤组和癌组病人上下径、前后径和左右径均小于囊肿组(P < 0.05)(见表 3及图 1~3)。
分组 n 大小 准确率
[n; 百分率(%)]上下径 左右径 前后径 腺瘤组 69 24.46±12.61 14.45±8.85 12.48±7.26 55(79.71) 囊肿组 7 48.71±12.89* 33.86±11.80* 31.17±11.91* 1(14.29) 癌组 4 26.50±13.18# 20.00±8.16# 17.00±2.83# 0(0.00) F — 11.67 14.82 19.42 — P — <0.01 <0.01 <0.01 <0.01△ MS组内 — 160.202 82.571 57.912 — q检验:与腺瘤组比较*P < 0.05;与囊肿组比较#P < 0.05;△示Fisher′s确切概率法 表 3 不同类型甲状旁腺肿瘤病人彩色多普勒超声检查参数比较(x±s; mm)
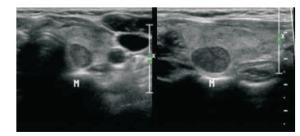
图 1 左侧甲状旁腺腺瘤,超声示甲状腺左叶后上方类圆形低回声结节,边界清晰
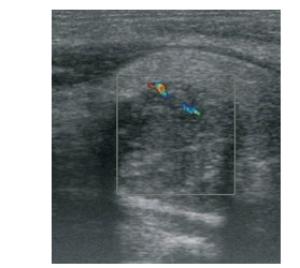
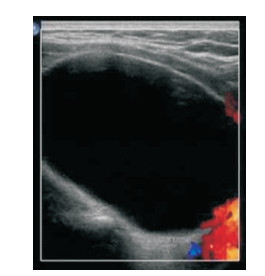
图 2 甲状腺旁癌,超声示甲状腺右叶腺体深层低回声区,边界不清

图 3 甲状旁腺囊肿,超声示甲状腺右叶椭圆形无回声区,边界清晰
-
共14例甲状旁腺腺瘤病人超声检查误诊为其他疾病,其中5例误诊为结节性甲状腺肿,5例误诊为甲状腺腺瘤(其中4例伴囊性变),1例误诊为甲状腺囊肿,1例误诊为甲状腺囊肿及结节性甲状腺肿,1例误诊为甲状腺癌,1例误诊为神经鞘瘤。3例甲状腺癌病人误诊,2例误诊为甲状腺癌,1例误诊为结节性甲状腺肿。5例甲状旁腺囊肿病人误诊,3例误诊为甲状腺囊肿,2例误诊为结节性甲状腺肿(其中1例伴囊性变)。
-
正常甲状旁腺体积较小,约5 mm×3 mm×1 mm,一般有4枚,分别紧贴于甲状腺左右叶背面,2%~3%甲状旁腺异位于纵隔、颈动脉或食管内[2]。目前正常甲状旁腺超声影像学检查仍然存在较大分歧[3],且因原发性甲状旁腺肿瘤发病率较低,超声医生诊断经验往往不足,所以甲状旁腺肿瘤超声影像学检查容易产生漏诊甚至误诊等情况[4]。
甲状旁腺腺瘤、增生、腺癌等原因均会引起甲状旁腺激素分泌过多,造成钙、磷和骨代谢紊乱,继而引起全身多脏器病变[5]。本研究也发现骨关节病变和泌尿系统结石是甲状旁腺腺瘤病人最主要的临床表现,这与既往研究[6]结果相一致,提示超声在鉴别诊断甲状旁腺腺瘤时,要综合考虑其临床表现,尤其表现出骨关节病变和泌尿系统结石的病人。甲状旁腺囊肿、甲状旁腺腺瘤和甲状旁腺癌病人的血磷水平依次下降,与国内研究[4]结果相一致,表明血磷水平在鉴别甲状旁腺肿瘤类型中有着重要作用。
骨型原发性甲状旁腺功能亢进症病人的PTH水平显著增高,导致成骨和破骨活动增加,骨转换率明显提高,会引起血清ALP水平增高[7]。本研究发现甲状旁腺腺瘤病人血清ALP水平高于甲状旁腺囊肿病人,这可能与甲状旁腺腺瘤病人PTH水平要显著高于甲状旁腺囊肿病人有关[4],也表明ALP在鉴别甲状旁腺腺瘤和甲状旁腺囊肿中有一定提示作用。
甲状旁腺肿瘤的术前准确定位十分重要,可以明确病变部位及肿瘤数量,精准指导手术,缩小探查范围,缩短手术时间,减低手术并发症,提高手术成功率。本次回顾性研究中各类甲状旁腺肿瘤定位准确率较其他研究[4]相对较低,这表明我院超声医生对甲状旁腺局部解剖欠熟悉及诊断经验不足,提示我们今后要加强科室超声医生甲状旁腺相关知识培训。本次研究还发现甲状旁腺肿瘤超声定位准确率与其肿瘤大小呈反向关系,甲状旁腺肿瘤越小,其定位准确性相对越高,这与既往研究[8]结果相似。这提示超声医生在遇到偏大的甲状旁腺肿瘤时,要注意辨别其界限,必要时应联合99Tcm-MIBI提高甲状旁腺肿瘤定位诊断准确率[9]。
既往研究[10]发现超声诊断甲状旁腺腺瘤准确率较高,但是甲状旁腺囊肿诊断准确率较低,本次研究结果与之一致,究其原因可能与甲状旁腺囊肿发病率较低导致超声医生对其认识不足有关。甲状旁腺腺瘤声像图主要表现为甲状腺腺体下缘、后方及下血管后方实性占位性病变[11],这导致其容易误诊为甲状腺来源。甲状旁腺癌声像图特点主要是瘤体体积较大,形态饱满,纵横比常≥1,内部回声不均匀,可伴有钙化或囊性变,常侵犯周围组织,表现为包膜增厚、粗糙或与周围组织分界不清,瘤体内部血管呈放射状,极易与甲状腺癌误诊[12]。因此,鉴别诊断时需结合其实验室检查指标。甲状旁腺囊肿声像图特点与甲状腺囊肿也极为相似,对于较大病变,超声难以鉴别,需进一步结合其他检查。
综上,彩色多普勒超声在筛查甲状旁腺肿瘤时,易误诊为甲状腺疾病。因此,在筛查甲状旁腺腺瘤时应综合考虑其临床表现、血磷和ALP等实验室检查相关指标,结合其超声声像图特点,进行鉴别诊断,必要时还需要联合99Tcm-MIBI检查。
原发性甲状旁腺肿瘤的超声与临床特征研究
Study on the ultrasound and clinical characteristics of primary parathyroid tumors
-
摘要:
目的分析甲状旁腺肿瘤病人临床特点和超声图像特点,为甲状旁腺肿瘤诊断和鉴别诊断提供参考。 方法回顾性分析经手术治疗的甲状旁腺肿瘤病人80例临床资料,其中甲状旁腺腺瘤69例(腺瘤组),甲状旁腺癌4例(癌组),甲状旁腺囊肿7例(囊肿组)。 结果腺瘤组病人以肾结石(9/69,13.04%)为主要临床表现。腺瘤组和癌组病人血磷水平均低囊肿组(P < 0.05),腺瘤组病人血钙和碱性磷酸酶水平均高于囊肿组(P < 0.05)。不同类型甲状旁腺肿瘤病人超声定位准确率差异有统计学意义(P < 0.01),以腺瘤组最高,为79.71%(55/69)。不同类型甲状旁腺肿瘤病人肿瘤上下径、左右径、前后径间差异均有统计学意义(P < 0.01),其中腺瘤组和癌组病人上下径、前后径和左右径均小于囊肿组(P < 0.05)。甲状旁腺腺瘤组病人误诊14例,以结节性甲状腺肿(5例)和甲状腺腺瘤(5例)最为常见。 结论甲状旁腺腺瘤诊断时应综合考虑其临床表现、血磷和碱性磷酸酶等实验室检查相关指标,并结合超声声像图特点,必要时还需要联合99Tcm-MIBI检查。 Abstract:ObjectiveTo analyze the clinical features and ultrasonographic features of patients with parathyroid tumors, and provide the reference for the diagnosis and differential diagnosis of parathyroid tumors. MethodsThe clinical data of 80 patients with parathyroid tumor treated with operation were retrospectively analyzed, The patients were divided into the adenoma group(69 cases with parathyroid adenom), cancer group(4 cases with parathyroid carcinoma) and cyst group(7 cases with parathyroid cyst). ResultsThe kidney stones were the main clinical manifestations in adenoma group(9/69, 13.04%).The serum phosphorus levels in cyst group were higher than that in adenoma group and cancer group(P < 0.05), and the serum levels of alcium and alkaline phosphatase in adenoma group were higher than those in cyst group(P < 0.05).The differences of the accuracy of ultrasound localization among patients with different types of parathyroid tumors were statistically significant(P < 0.01), and which in adenoma was the highest[79.71% (55/69)].The differences of the vertical, transverse and anteroposterior diameters in patients with different types of parathyroid tumors were statistically significant(P < 0.01), and the vertical, transverse and anteroposterior diameters in adenoma group and cancer group were less than those in cyst group(P < 0.05).Fourteen patients in the parathyroid adenoma group were misdiagnosed, and the nodular goiter(5 cases) and thyroid adenoma(5 cases) were the most common. ConclusionsIn the diagnosis of parathyroid adenoma, the clinical manifestations, blood phosphorus, ALP, other relevant indicators of laboratory examination and characteristics of ultrasonography should be taken into comprehensive consideration, , and the 99Tcm-MIBI examination should be combined when necessary. -
Key words:
- primary parathyroid tumor /
- ultrasonography /
- clinical feature
-
表 1 不同类型甲状旁腺肿瘤病人年龄和性别比较[n; 百分率(%)]
分组 n 年龄(x±s)/岁 男 女 腺瘤组 69 49.81±13.96 21(30.43) 48(69.57) 囊肿组 7 47.71±13.01 2(28.57) 5(71.43) 癌组 4 48.25±11.32 2(50.00) 2(50.00) F — 0.09 — P — >0.05 >0.05* MS组内 — 190.285 — *示Fisher′s确切概率法  下载: 导出CSV
下载: 导出CSV
表 2 不同类型甲状旁腺肿瘤病人血钙、磷和ALP水平比较(x±s)
分组 n 钙/(mmol/L) 磷(mmol/L) ALP
[M50(M25, M75)]/(ng/L)腺瘤组 69 3.01±0.76 0.78±0.26 174.00(108.00, 427.00) 囊肿组 7 2.31±0.10* 1.24±0.20* 51.00(37.00, 69.00)* 癌组 4 2.71±0.38 0.64±0.09# — F — 3.22 11.65 3.97△ P — <0.05 <0.01 <0.01 MS组内 — 0.516 0.063 — q检验:与腺瘤组比较*P < 0.05;与囊肿组比较#P < 0.05;△示uc值
下载: 导出CSV
表 3 不同类型甲状旁腺肿瘤病人彩色多普勒超声检查参数比较(x±s; mm)
分组 n 大小 准确率
[n; 百分率(%)]上下径 左右径 前后径 腺瘤组 69 24.46±12.61 14.45±8.85 12.48±7.26 55(79.71) 囊肿组 7 48.71±12.89* 33.86±11.80* 31.17±11.91* 1(14.29) 癌组 4 26.50±13.18# 20.00±8.16# 17.00±2.83# 0(0.00) F — 11.67 14.82 19.42 — P — <0.01 <0.01 <0.01 <0.01△ MS组内 — 160.202 82.571 57.912 — q检验:与腺瘤组比较*P < 0.05;与囊肿组比较#P < 0.05;△示Fisher′s确切概率法
下载: 导出CSV
-
[1] 邓艳华, 刘建民.甲状旁腺良恶性肿瘤的鉴别[J].诊断学理论与实践, 2010, 9(6):622. [2] 王寅, 薛改琴, 王宇翔, 等.正常甲状旁腺超声特点及其临床意义[J].肿瘤研究与临床, 2019, 31(10):690. doi: 10.3760/cma.j.issn.1006-9801.2019.10.010 [3] 章建全, 仇明.正常人甲状旁腺超声影像特征的筛查及验证[J].第二军医大学学报, 2013, 34(5):349. [4] 张俊花, 薛改琴.彩色多普勒超声对原发性甲状旁腺肿瘤的诊断价值[J].中国药物与临床, 2015, 15(4):507. [5] 谭屾, 崔爱民, 柏楠, 等.甲状旁腺癌8例的诊治及围手术期PTH、Ca水平分析[J].山西医科大学学报, 2017, 48(10):1066. [6] 周远.39例甲状旁腺腺瘤的临床特点及外科治疗分析[D].吉林: 吉林大学, 2018. [7] 张小会, 胡成进, 王延群.甲状旁腺激素及其他生化指标在继发性甲状旁腺功能亢进手术中的应用[J].国际检验医学杂志, 2019, 40(17):2128. doi: 10.3969/j.issn.1673-4130.2019.17.019 [8] 童传明, 郑荆州, 吴高松.原发性甲状旁腺功能亢进症115例诊治分析[J].中华内分泌外科杂志, 2016, 10(1):45. doi: 10.3760/cma.j.issn.1674-6090.2016.01.012 [9] MOURE D, LARRANAGA E, DOMINGUEZ GL, et al.99mTcsestamibi as sole technique in selection of primary hyperparathyroidism patients for unilateral neck exploration[J].Surgery, 2008, 144(3):454. doi: 10.1016/j.surg.2008.05.014 [10] NIECIECKI M, CACKO M, KROLICKI L.The role of ultrasound and nuclear medicine methods in thepreoperative diagnostics of primary hyperparathyroidism[J].J Ultrason, 2015, 63(15):398. [11] 张俊花.超声检查在甲状旁腺疾病诊疗中的临床应用[J].肿瘤影像学, 2019, 28(4):271. [12] FANG C, KONSTANTATOU E, MULHOLLAND NJ, et al.A retrospective review of the role of B-mode and color doppler ultrasonography in the investigation of primary hyperparathyroidism:features that differentiate benign from malignant lesions[J].J Ultrason, 2018, 26(2):110. -

 点击查看大图
点击查看大图

图(3)表(3)
计量
- 文章访问数: 3509
- HTML全文浏览量: 1848
- PDF下载量: 16
- 被引次数: 0
