


-
在所有常见的恶性肿瘤中,结直肠癌在男性病人中排名第三,女性病人中排名第二[1]。由于结直肠癌的初期病症并不是很明显,病人常常难以发觉,就诊时已经是中晚期,严重影响病人的预后, 结直肠癌已经成为严重影响我国人民健康的主要恶性肿瘤之一[2]。影响结直肠癌预后的因素有很多,例如TNM分期、肿瘤生长部位、术前肠梗阻情况等,其中结直肠癌分化程度也是影响病人预后的重要因素[3]。能谱CT采用最新的软硬件及技术,在大肠癌的TNM分期等方面已有不少研究,并且在临床诊疗中发挥极大的作用,具有不可估量的潜力[4-6], 但是在大肠癌分化程度中却很少有人探究。本研究旨在利用能谱CT分析不同分化程度结直肠癌中各能谱参数间的差异,从而可以术前评估结直肠癌病人的分化程度,帮助临床提供更精准的医学信息,更好地评价及预测病人的预后情况。
-
收集蚌埠医学院第一附属医院2019年11月至2020年6月经肠镜及病理活检证实的大肠癌病人50例,均在术前进行能谱CT检查,在进行GSI扫描前均未进行手术及放化疗等相关治疗,且无碘剂及654-2过敏史,并于检查后1周内进行手术。其中男26例,女24例;年龄33~90岁;中高分化腺癌32例,低分化腺癌18例。
-
检查前均禁食8~12 h,于检查前一晚泡服番泻叶20 g清洁肠道,检查前30 min嘱病人饮水800 mL左右,并适时注射654-2 10 mg,训练病人做屏气训练以改善肠道蠕动,提高图像的清晰度。然后采取256排Revolution能谱CT对病人进行全腹平扫和双期增强扫描,扫描参数:GSI能谱扫描模式,速度158.75 mm/s,螺距0.992,探测器宽度0.625 mm×64 mm,管电流600 mA,管电压80 kVp、140 kVp间0.5 ms瞬时切换,经肘静脉注射造影剂碘普罗胺,流率3.5 mL/s,剂量1.0 mL/kg,采取智能追踪技术对腹主动脉进行CT值的监测,监测的阈值为120 HU,之后开始进行动脉期扫描,约30 s后进行静脉期扫描。
-
将图像重建为薄层图像,并传至ADW4.7后处理工作站,打开GSI Viewer软件General板块进行观察,并选取合适的感兴趣区(region of interest,ROI),勾画ROI时要尽可能地避免坏死、囊变、钙化区域,同时采用复制、粘贴的方法保持ROI的面积、形状、位置一致。由3名有经验的放射科医生互盲分别进行ROI的画取,每位医生在感兴趣病灶的最优层面及其上下层面分别进行测量并取平均值,在自动生成的相关能谱图像中获取病灶的碘基值(IC)、水浓度、有效原子序数(Eff-Z), 同时在画取ROI最佳层面上测量主动脉及髂血管的单能量IC作为标准参照值,并且手动计算该病灶的标准化碘浓度(NIC), NIC=病灶碘浓度/同层面主动脉或髂血管的碘浓度,以及能谱曲线斜率(K), K=[CT(40 keV)-CT(100 keV)]/(100 keV-40 keV)。
-
采用t检验、χ2检验和ROC曲线分析。
-
2组性别、年龄、肿瘤生长部位、T分期差异均无统计学意义(P>0.05),低分化组肿瘤的淋巴结转移高于中高分化组(P < 0.05)(见表 1)。2组动脉期IC、NIC、水浓度、Eff-Z、K及静脉期水浓度、Eff-Z差异均无统计学意义(P>0.05), 低分化组静脉期IC、NIC、K均高于中高分化组(P < 0.05)(见表 2、3)。
分组 n 男 女 年龄/岁 部位 T分期 淋巴结转移 ≥65 < 65 左半结肠 右半结肠 直肠 T1+T2 T3+T4 是 否 低分化组 18 10 8 8 10 5 7 6 2 16 12 6 中高分化组 32 16 16 19 13 9 11 12 7 25 11 21 χ2 — 0.14 1.03 0.12 0.32 4.84 P — >0.05 >0.05 >0.05 >0.05 < 0.05 表 1 结直肠癌低分化组与中高分化组临床病理特征比较(n)
分组 n IC/(100 μg/mL) NIC 水浓度/(mg/mL) Eff-Z K 低分化组 18 16.28 ±2.45 0.19 ±0.04 1 032.33±4.87 8.51 ±0.23 1.97±0.44 中高分化组 32 15.54 ±3.92 0.17±0.04 1 033.49±10.91 8.50 ±0.2 1.83±0.48 t — 0.72 1.77 0.43 0.10 1.01 P — >0.05 >0.05 >0.05 >0.05 >0.05 表 2 动脉期结直肠癌低分化组与中高分化组能谱参数比较(x±s)
分组 n IC/(100 μg/mL) NIC 水浓度/(mg/mL) Eff-Z K 低分化组 18 20.02±2.09 0.62 ±0.82 1 035.16±4.39 8.7 ±0.17 2.37±0.27 中高分化组 20 18.87 ±3.59 0.50±0.11 1 033.89±5.27 8.66±0.21 2.04±0.46 t — 2.32 4.01 0.87 0.55 2.58 P — < 0.05 < 0.05 >0.05 >0.05 < 0.05 表 3 静脉期结直肠癌低分化组与中高分化组能谱参数比较(x±s)
-
静脉期IC、NIC、K诊断结直肠癌分化程度的曲线下面积(AUC)(95%CI)分别为0.77(0.64~0.90)、0.81(0.69~0.93)、0.79(0.66~0.92),当静脉期IC的阈值为18.31(100 μg/mL)时,敏感度和特异度分别为88.3%、62.5%;当静脉期NIC诊断临界值为0.56时,敏感度和特异度分别为83.3%、75.0%;当静脉期K阈值为2.07,敏感性和特异度为88.9%、68.7%。
-
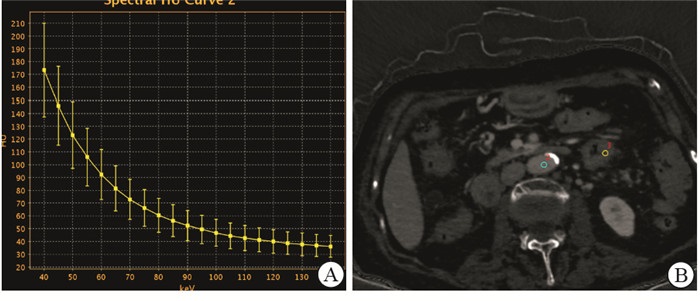
病例1,男,45岁,乙状结肠低分化腺癌(见图 1);病例2,女,68岁,左半结肠中分化腺癌(见图 2)。

图 1 乙状结肠低分化腺癌能谱图像

图 2 左半结肠中分化腺癌能谱图像
-
随着全球人口的快速增长和老龄化的增加,癌症作为主要死因的地位日益突出,且在最近十年间,中国的癌症发病率和死亡率还在继续增加[1]。目前,结直肠癌的治疗首选手术切除,并辅以化疗、放疗、靶向药物治疗等[7],但是大多数病人发现已经是中晚期,因此提高术前诊断率,改善病人预后至关重要。结直肠癌的术前检查有结肠镜、CT、MRI等,但是上述手段仅能定性提供形态解剖学上的信息,无法更深层次地定量挖掘肿瘤内部的分子运动、化学性质、甚至病理学方面的信息,近几年出现的能谱CT正好可以一定程度地弥补这一缺陷。能谱CT采用瞬时(< 0.05 ms)切换技术,使球管和探测器同时采集能谱数据成为可能[8]。具有快速千伏开关的能谱CT可以同时同角度进行高低(40/140 keV)能量转换,在提高影像质量的同时获取101幅单能量图像、基物质图、有效原子序数图、能谱曲线图等[9-10]。
能谱CT常采用碘、水这两种基物质,因为碘和水密度差别较大,基本包含了医学中不同组织结构的密度范围。同时保持在不同结直肠癌分化程度之间水的差异不明显,以水作为参照,更加有利于评估肿瘤的碘浓度[11]。本研究就Revolution CT定量参数是否有助于辨别结直肠癌的病理类型进行了探索。结果显示,低分化结直肠癌静脉期IC、NIC、K均高于中高分化结直肠癌。分化程度越低,IC、NIC、K的值越高,这与GONG等[12-13]的研究结果相似。由于能谱CT成像主要是根据病灶内碘的浓度而间接反映肿瘤的生物特性,对于富血供的病灶,其碘浓度就会相对较高,而乏血供的病灶情况相反。病灶碘的含量不同,其能谱的衰减曲线也会有所不同,也可以一定程度地反映病灶的血供情况。分化程度可以间接反映肿瘤的生物学行为,分化程度高的肿瘤,则生物学行为越接近正常组织,异型性较小,分化程度低的肿瘤,肿瘤组织的异型性较大,其恶性程度也就比较高[14],且恶性程度越高,肿瘤血管的生长就更加迅速,微血管密度就越丰富,血管内皮细胞也更加不完整,血供就更加丰富,瘤灶摄取碘的能力就越强,最后病灶的碘浓度也就比中高分化组的值高[15]。本研究结果显示,静脉期NIC的诊断效能最高,而静脉期IC诊断效能相对较低。其原因可能是由于个体差异的影响,及对比剂注射速率、剂量的不同,导致所测得的碘浓度也有一定的差异,所以对碘浓度进行标准化,以排除这些因素的影响,可以更加精确地评价病灶的血流状态。本研究中发现动脉期NIC、IC、K在低分化组与中高分化组之间差异无统计学意义,可能是因为动脉期时间设置得比较早,病灶内碘浓度分布不均或者没有达到峰值有关;也可能是病人样本量不够,且2组之间样本量有一定的差异,或者ROI的选择具有一定的主观性,导致测得的值可能存在一定的误差。物质衰减曲线取决于光电效应和康普顿效应,并反映了物质的射线吸收系数与能量变化有关,且射线吸收系数与原子序数、密度等也有密切联系,因此,不同CT单能量条件下以及不同的物质吸收系数不同,从而在此基础上绘制出能谱曲线,定量区分不同的物质[16]。本研究还发现低分化结直肠癌组的K值较中高分化组高,证实了低分化大肠癌与中高分化结直肠癌内部物质组成不同。
此外,本研究还对低分化和中高分化结直肠癌的临床病理之间的关系进行了研究,发现低分化的结直肠癌更容易发生转移。肿瘤的分化程度低,意味着更早地侵犯肌层,侵袭性也就比较高,淋巴结的转移概率就越高[17]。所以分化程度越低,晚期组(T3、T4)的数量就比早期组(T1、T2)越多,在本研究中,结直肠癌早期组与晚期组之间差异无统计学意义,但是可以看到低分化组的早期癌的比例(2/18)要低于中高分化组(7/32)。有研究[3]证实不同肿瘤部位的预后不同,且左半结直肠与右半结直肠之间分化程度也有一定的差异。但本研究中肿瘤部位与结直肠癌分化程度没有明显关系,可能与病人数量较少有关,需要扩大样本量、进行多中心探究。
Revolution CT能谱CT参数IC、NIC以及K在结直肠癌分化程度中有较高的应用价值, 可以在术前对结直肠癌的分化程度做出预测,以帮助临床制定诊疗方案。
能谱CT在结直肠癌分化程度中的应用价值研究
Aapplication value of spectral CT in the evaluation of the differentiation degree of colorectal cancer
-
摘要:
目的研究256排Revolution能谱CT各参数在结直肠癌分化程度中的应用价值。 方法选取50例通过肠镜或病理确诊的结直肠癌病人,于手术前行GSI能谱CT平扫及双期扫描,通过GSI Viewer软件获得相关能谱图像,并在病灶内勾画出合适的感兴趣区,测量病灶的碘基值(IC)、水浓度、有效原子序数(Eff-Z)、标准化碘浓度(NIC)及能谱曲线斜率(K)。根据病理结果,将50例病人分为低分化组与中高分化组,比较2组各能谱参数,并采用ROC曲线分析各能谱参数的诊断能力。 结果50例病人中高分化组32例,低分化组18例。低分化组肿瘤的淋巴结转移高于中高分化组(P < 0.05)。2组动脉期IC、NIC、水浓度、Eff-Z、K及静脉期水浓度、Eff-Z差异均无统计学意义(P>0.05),低分化组静脉期IC、NIC、K均高于中高分化组(P < 0.05)。静脉期IC、NIC、K诊断结直肠癌分化程度的曲线下面积分别为0.77、0.81、0.79,诊断阈值分别为18.31、0.56、2.07,敏感性分别为88.3%、83.3%、88.9%,特异性分别为62.5%、75.0%、68.7%。 结论能谱CT参数IC、NIC以及K在结直肠癌分化程度中有较高的应用价值。 -
关键词:
- 结直肠肿瘤 /
- 体层摄影术,X线计算机 /
- 能谱成像 /
- 病理分级
Abstract:ObjectiveTo investigate the application value of each parameter of 256-row Revolution spectral CT in evaluating the differentiation degree of colorectal cancer. MethodsFifty patients with colorectal cancer diagnosed by colonoscopy or pathology were selected, and detected using the GSI spectral CT plain scan and dual-phase scan before surgery.The relevant spectral images were obtained through GSI Viewer software, the appropriate region of interest was delineated in the lesion, and the iodine base value(IC), water concentration, effective atomic number(Eff-Z), normalized iodine concentration(NIC) and energy spectral slope(K) of the lesion were measured.According to the pathological results, 50 patients were divided into the low differentiation group and middle-high differentiation group.The spectral parameters were compared between two groups, and the diagnostic ability of each spectral parameter were analyzed using the receiver operating characteristic curve. ResultsAmong 50 patients, 32 cases in middle-high differentiation group and 18 cases in low differentiation group were identified.The lymph node metastasis in low differentiation group was higher than that in middle-high differentiation group(P < 0.05).There was no statistical significance in the IC, NIC, water concentration, Eff-Z and K of arterial phase, and water concentration and Eff-Z of venous phase between two groups(P>0.05).The IC, NIC and K of venous phase in low differentiation group were higher than those in middle-high differentiation group(P < 0.05).The area under the curve, diagnostic threshold, sensitivity and specificity of venous phase IC, NIC, and K were (0.77, 0.81 and 0.79), (18.31, 0.56 and 2.07), (88.3%, 83.3% and 88.9%) and (62.5%, 75.0% and 68.7%), respectively. ConclusionsThe parameters IC, NIC and K of spectral CT have high values in evaluating the differentiation of colorectal cancer. -
表 1 结直肠癌低分化组与中高分化组临床病理特征比较(n)
分组 n 男 女 年龄/岁 部位 T分期 淋巴结转移 ≥65 < 65 左半结肠 右半结肠 直肠 T1+T2 T3+T4 是 否 低分化组 18 10 8 8 10 5 7 6 2 16 12 6 中高分化组 32 16 16 19 13 9 11 12 7 25 11 21 χ2 — 0.14 1.03 0.12 0.32 4.84 P — >0.05 >0.05 >0.05 >0.05 < 0.05  下载: 导出CSV
下载: 导出CSV
表 2 动脉期结直肠癌低分化组与中高分化组能谱参数比较(x±s)
分组 n IC/(100 μg/mL) NIC 水浓度/(mg/mL) Eff-Z K 低分化组 18 16.28 ±2.45 0.19 ±0.04 1 032.33±4.87 8.51 ±0.23 1.97±0.44 中高分化组 32 15.54 ±3.92 0.17±0.04 1 033.49±10.91 8.50 ±0.2 1.83±0.48 t — 0.72 1.77 0.43 0.10 1.01 P — >0.05 >0.05 >0.05 >0.05 >0.05
下载: 导出CSV
表 3 静脉期结直肠癌低分化组与中高分化组能谱参数比较(x±s)
分组 n IC/(100 μg/mL) NIC 水浓度/(mg/mL) Eff-Z K 低分化组 18 20.02±2.09 0.62 ±0.82 1 035.16±4.39 8.7 ±0.17 2.37±0.27 中高分化组 20 18.87 ±3.59 0.50±0.11 1 033.89±5.27 8.66±0.21 2.04±0.46 t — 2.32 4.01 0.87 0.55 2.58 P — < 0.05 < 0.05 >0.05 >0.05 < 0.05
下载: 导出CSV
-
[1] BRAY F, FERLAY J, S0ER JOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394. doi: 10.3322/caac.21492 [2] 黄陈, 戎泽印. 结直肠癌诊治新进展[J]. 蚌埠医学院学报, 2018, 43(10): 40. [3] 韩晶, 王贵英, 张难, 等, 肿瘤部位及临床病理特征对不同TNM分期行结直肠癌根治性切除术患者预后的影响研究[J]. 中国全科医学, 2020, 23(18): 2275. doi: 10.12114/j.issn.1007-9572.2020.00.336 [4] 王传彬, 程涛. 能谱CT等渗甘露醇胃肠低张造影诊断直肠癌分期[J]. 中国医学影像学杂志, 2015, 23(11): 839. doi: 10.3969/j.issn.1005-5185.2015.11.011 [5] 冯长明, 徐慧慧, 霍英杰, 等. 双能量CT能谱图像对结直肠癌的诊断及术前分期中的运用价值[J]. 湖南师范大学学报(医学版), 2019, 16(1): 165. [6] KATO T, UEHARA K, ISHIGAKI S, et al. Clinical significance of dual-energy CT-derived iodine quantification in the diagnosis of metastatic LN in colorectal cancer[J]. Eur J Surg Oncol, 2015, 41(11): 1464. doi: 10.1016/j.ejso.2015.08.154 [7] ZHANG L, ZHAO Y, DAI Y, et al. Immune landscape of colorectal cancer tumor microenvironment from different primary tumor location[J]. Front Immunol, 2018, 9: 1578. doi: 10.3389/fimmu.2018.01578 [8] WU X. Monocromatic CT image representation via fast switching dual kVp[J]. Proc Spie, 2009, 72(58): 725. [9] MATSUMOTO K, JINZAKI M, TANAMI Y, et al. Virtual monochromatic spectral imaging with fast kilovoltage switching: improved image quality as compared with that obtained with conventional 120-kVp CT[J]. Radiology, 2011, 259(1): 257. doi: 10.1148/radiol.11100978 [10] PEREZ-LARA A, FORGHANI R. Spectral computed tomography: Technique and applications for head and neck cancer[J]. Magn Reson Imaging Clin N Am, 2018, 26(1): 1. doi: 10.1016/j.mric.2017.08.001 [11] 陈丽红, 薛蕴菁, 段青, 等. 能谱成像定量评估胃癌分化程度[J]. 中国医学影像技术, 2013, 29(2): 225. [12] GONG HX, ZHANG KB, WU LM, et al. Dual energy spectral CT imaging for colorectal cancer grading: A preliminary study[J]. PLoS One, 2016, 11(2): 1. [13] 王传彬, 韦树华, 张萍, 等. 能谱CT术前定量评估直肠腺癌分化程度的应用价值值[J]. 实用放射学杂志, 2017, 33(3): 451. doi: 10.3969/j.issn.1002-1671.2017.03.033 [14] ZHANG J, TIAN ZL, ZHANG WT, et al. Clinicopathological and prognostic significance of miR-4317 expression in gastric cancer patients[J]. Eur Rev Med Pharmacol Sci, 2019, 23(7): 2803. [15] DU JR, JIANG Y, ZHANG YM, et al. Vascular endothelial growth factor and microvascular density in esophageal and gastric carcinomas[J]. World J Gastroenterol, 2003, 9(7): 1604. doi: 10.3748/wjg.v9.i7.1604 [16] 唐琪, 谢东, 苏丹柯, 等. 能谱CT定量参数鉴别诊断原发性胃淋巴瘤和胃癌[J]. 中国医学影像技术, 2017, 33(2): 221. [17] 曹立强, 杨国军, 刘思达, 等. 结直肠癌术前淋巴结转移相关危险因素分析[J]. 世界最新医学信息文摘, 2019, 19(99): 25. -

 点击查看大图
点击查看大图
图(2)表(3)
计量
- 文章访问数: 3410
- HTML全文浏览量: 2105
- PDF下载量: 14
- 被引次数: 0
