

-
卵巢癌是女性生殖系统中较为常见的一种恶性肿瘤,其发病率仅次于宫颈癌、子宫体癌,此病具有疾病隐匿、早期症状不明显的特点,且目前临床上对于卵巢癌无特异性的诊断指标,大多数病人在疾病诊断时已经处于晚期,错过了最佳的治疗时机,病人预后较差,病死率较高[1]。因此寻找有效的诊断卵巢癌的敏感指标,对病人的早期诊断及治疗具有重要的意义。有研究[2]采用人附睾蛋白4(HE4)、糖类抗原125(CA125)、人溶血磷脂酸(LPA)对上皮性卵巢癌病人进行联合诊断,其研究结果中认为HE4在卵巢癌组织中高表达,与卵巢癌细胞所分泌的LPA升高共同参与此病的发生。亦有研究[3]认为,HE4与糖类抗原199(CA199)相关,共同参与卵巢癌的发生,可作为卵巢癌的早期诊断指标。另外有研究[4]发现,LPA、CA199与上皮性卵巢癌病人治疗效果相关,可作为病人病情诊断指标。基于上述研究,本文旨在探讨HE4、CA199及LPA在卵巢癌中的表达及与临床病理特征的相关性,以期为临床上卵巢癌的早期诊治提供参考。
-
选择2018年1月至2019年4月于唐山市妇幼保健院就诊的卵巢癌病人140例作为卵巢癌组,年龄34~65岁,平均年龄(49.5±2.5)岁;FIGO临床分期:Ⅰ期15例,Ⅱ期21例,Ⅲ期45例,Ⅳ期59例;病理类型:浆液性囊腺癌76例,黏液性囊腺癌32例,卵巢子宫内膜样癌32例;分化程度:低分化53例,中分化46例,高分化41例;肿瘤直径:≥5 cm 59例, < 5 cm 81例;有淋巴结转移62例,无淋巴结转移78例。同期选取唐山市妇幼保健院因卵巢良性病变而行手术切除的病人120例作为卵巢良性病变组,年龄30~65岁,平均年龄(48.6±2.6)岁。另外同期选取在唐山市妇幼保健院行健康体检女性100名作为健康对照组,年龄35~60岁,平均年龄(48.9±2.5)岁。3组研究对象年龄差异无统计学意义(P>0.05),具有可比性。本次研究所有研究及其家属均知情,并签署了知情同意书,且经过医院伦理委员会批准。
-
纳入标准:卵巢癌组病人均经临床、组织病理、免疫组织化学、影像学等手段确诊。卵巢良性病变组病人经病理证实为卵巢良性病变。健康对照组肝肾功能正常,妇科检查无异常,无家族肿瘤史。排除标准:其他肿瘤病人;严重内科基础疾患如冠心病、心力衰竭等;肝肾功能不全者;合并其他器官恶性肿瘤存在者。
-
取3组研究对象清晨空腹静脉血5 mL,在取血1 h内分离出血清、血浆,在-80 ℃环境下保存。取卵巢癌组、卵巢良性病变组病人手术切除的卵巢组织,在10%中性甲醛中固定,固定处理24 h后行常规的石蜡包埋处理,制作组织切片,厚度为4 μm,用于后续免疫组织化学(免疫组化)染色。
-
血清HE4表达水平采用ELISA法检测,血清CA199表达水平采用电化学发光法检测,血浆LPA表达水平采用无机定磷法检测。
-
将所制备的卵巢癌组、卵巢良性病变组卵巢组织石蜡切片在二甲苯中重复脱蜡处理10 min,行梯度乙醇水化,将蛋白酶修复液加入在37 ℃的恒温冰箱中行孵化30 min,去除抗原修复液,将所制备的切片转移至内含3% H2O2的湿盒中,去过氧化物酶封闭液密封,在37 ℃的恒温冰箱中行孵化10 min,PBS清洗。清洗完成后将山羊血清加入,在室温下封闭处理30 min,用滤纸将封闭液吸处除,加入一抗,放入至适合后加入二抗,在室温下孵育处理1 h,PBS清洗,DAB显色处理10 min,梯度乙醇脱水,二甲苯冲洗片3次一直到透明,采用中性树脂封片处理,显微镜下观察免疫组化染色情况。每份标本在镜头下随机选择5个视野,所有病理切片均由2位以上经验丰富的医师采用双盲法进行确诊。根据染色程度和染色细胞百分比进行评分:不着色0分,淡黄色1分,黄色2分,棕黄色3分;着色细胞数≤5% 0分,6%~25% 1分,26%~50% 2分,≥51% 3分。得分≤1分为阴性(-),2~3分为弱阳性(+);4~5分为中度阳性(2+);≥6分为强阳性(3+)。
-
采用t检验、方差分析、q检验、χ2检验和Pearson相关性分析。
-
血清HE4、CA199、血浆LPA水平,卵巢癌组血清均高于卵巢良性病变组和健康对照组,卵巢良性病变组均高于健康对照组(P < 0.05)(见表 1)。
分组 n HE4/(pmol/mL) CA199/(U/mL) LPA/(μmol/L) 健康对照组 100 44.23±5.46 13.12±1.13 2.03±0.24 卵巢良性病变组 120 59.68±10.24* 16.24±3.46* 2.29±0.98* 卵巢癌组 140 316.25±49.68*# 134.25±46.58*# 5.16±1.12*# F — 2 966.33 718.87 465.51 P — < 0.01 < 0.01 < 0.01 MS组内 — 1 004.189 849.128 0.825 q检验:与健康对照组比较*P < 0.05;与卵巢良性病变组比较#P < 0.05 表 1 3组研究对象血清HE4、CA199、血浆LPA水平的比较(x±s)
-
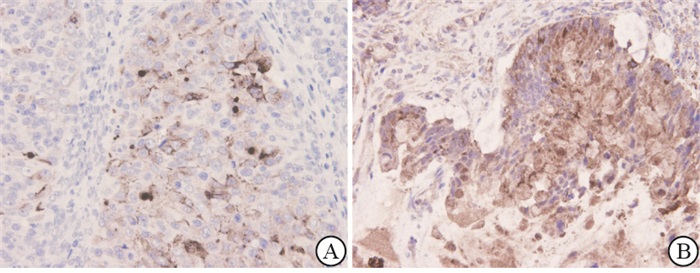
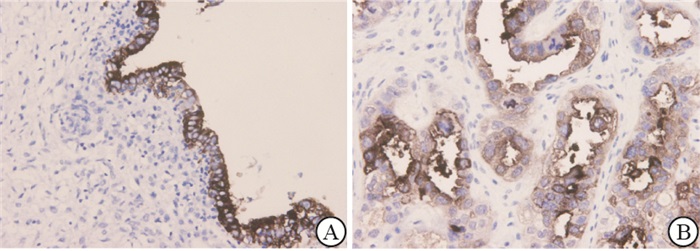
HE4、CA199、LPA在卵巢癌组卵巢组织中的阳性表达率均显著高于卵巢良性病变组(P < 0.01)(见表 2、图 1~3)。
分组 n HE4 CA199 LPA 卵巢良性病变组 120 32(26.67) 28(23.33) 42(35.00) 卵巢癌组 140 129(92.14) 131(93.57) 118(84.29) χ2 — 117.49 134.19 66.31 P — < 0.01 < 0.01 < 0.01 表 2 HE4、CA199、LPA在卵巢良性病变组与卵巢癌组卵巢组织中的阳性表达情况比较[n;百分率(%)]
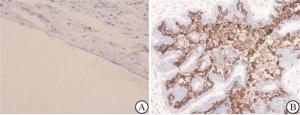
图 1 HE4在卵巢组织中的表达免疫组化图(DAB染色)

图 2 CA199在卵巢组织中的表达免疫组化图(DAB染色)

图 3 LPA在卵巢组织中的表达免疫组化图(DAB染色)
-
HE4、CA199、LPA表达与卵巢癌病人病理类型、肿瘤直径无相关性(P>0.05),与卵巢癌病人临床分期、分化程度、有无淋巴结转移有相关性(P < 0.01);其中临床分期Ⅲ~Ⅳ期、低分化程度、有淋巴结转移的卵巢癌病人HE4、CA199、LPA表达较高(见表 3)。
指标 n HE4/(pmol/mL) CA199/(U/mL) LPA/(μmol/L) 临床分期 Ⅰ~Ⅱ期 36 246.38±68.59 48.62±9.65 3.46±0.24 Ⅲ~Ⅳ期 104 459.68±124.25 124.26±32.15 5.16±1.02 t — 9.78 13.87 9.88 P — < 0.01 < 0.01 < 0.01 分化程度 高 41 182.46±24.15 76.35±12.04 3.10±0.10 中 46 235.56±50.69△ 110.23±45.23△ 3.21±0.23△ 低 53 462.25±126.35△▲ 134.25±68.59△▲ 5.63±1.10△▲ F — 151.825 15.51 210.09 P — < 0.01 < 0.01 < 0.01 MS组内 — 7 073.723 2 499.970 0.480 病理类型 浆液性 76 245.26±42.25 124.25±35.26 4.13±0.65 非浆液性 64 252.25±43.26 125.26±35.49 4.16±0.68 t — 0.96 0.17 0.27 P — >0.05 >0.05 >0.05 淋巴结转移 有 62 398.56±102.12 135.49±58.25 5.86±1.10 无 78 265.35±53.27 109.58±23.58 3.45±0.24 t — 9.95 3.58 18.81 P — < 0.01 < 0.01 < 0.01 肿瘤直径/cm ≥5 59 232.16±68.59 124.25±15.36 4.10±0.21 < 5 81 231.25±72.16 126.35±16.69 4.13±0.20 t — 0.08 0.76 0.86 P — >0.05 >0.05 >0.05 q检验:与高分化相比较△P < 0.05;与中分化相比较▲P < 0.05 表 3 HE4、CA199、LPA水平与卵巢癌病人临床病理特征的相关性分析(x±s)
-
HE4、CA199、LPA之间进行Pearson相关性分析,HE4与CA199呈现显著正相关关系(r=0.183, P < 0.05),HE4与LPA呈显著正相关关系(r=0.216, P < 0.05),CA199与LPA之间呈正相关(r=0.209, P < 0.05)。
-
卵巢癌具有发病隐匿的特点,早期无特异性症状,加之临床上缺乏早期诊断的指标,导致多数病人预后大多不良,因此提高卵巢癌的早期诊断对病人预后治疗具有重要的作用。
HE4最早在1991年被KIRCHOFF等发现于附睾远端的上皮细胞中,属于核心表位蛋白2基因的编码产物,其全长为12 kb,是由4个内含子和5个外显子所组成的,在多种剪切方式中所存在,对含有乳清酸型4个二硫键核心域的蛋白质具有编码作用[5-6]。HELLSTROM等在2003年最先将HE4应用于诊断卵巢癌,认为HE4在卵巢癌病人中呈现为异常高表达,使得HE4这一新型肿瘤标志物成为卵巢癌诊断的热点。目前研究[7-8]认为,HE4在多种恶性肿瘤中均出现异常高表达,与病人疾病进展具有一定的相关性。贺帅等[9]研究认为HE4在卵巢癌病人血清中、癌组织中均呈现为高表达。本文研究结果显示,与卵巢良性病变病人和健康女性相比,卵巢癌病人血清中HE4水平均较高;与卵巢良性病变病人相比,卵巢癌病人卵巢组织中HE4阳性表达率较高,与上述研究结果一致。另外本文进一步分析HE4与卵巢癌病人临床病理特征的相关性,结果显示,HE4与卵巢癌病人临床分期、分化程度、有无淋巴结转移相关,此结果说明,HE4参与卵巢癌的发生和发展。马书丽等[10]研究认为,HE4的异常表达与病人临床分期为Ⅲ~Ⅳ期、组织学分级为中、低分化、有淋巴结转移、死亡有关,本文与其研究结果一致。
CA199属于一种糖抗原,是与胆囊癌、胰腺癌、结肠癌、胃癌等肿瘤相关的肿瘤标志物,在临床上又被称为胃肠癌相关抗原,是一种由单克隆抗体116NS19-9所识别的抗原成分,在健康人血清中CA199值为0~37 U/mL[11]。李炜等[12]研究认为CA199可用于卵巢癌的诊断。李丹妍等[13]在其研究中认为CA199在卵巢癌病人中为高表达。本文结果显示,CA199在卵巢癌病人中高表达,且与病人疾病分期、分化程度以及是否存在淋巴结转移相关,与上述研究结果中认为CA199可作为卵巢癌淋巴结转移的血清标志物的结果一致。
LPA属于一类脂类小分子,其结构较为简单,具有多种信号转导的作用,被临床上称为“磷脂信使”,在机体处于正常生理条件下,其在血浆中的表达较低,当机体细胞癌变,恶性肿瘤形成后病人血浆中LPA表达显著升高,目前研究[15-16]认为,LPA参与癌细胞的生物学行为过程,LPA表达的高低与肿瘤病人预后情况不良或者良好相关。已有研究[17-19]发现,LPA在卵巢癌的发生发展过程中具有重要的作用,可通过G蛋白所介导的不同种信号通路而发挥其自身生物学效应;LPA参与卵巢癌发生发展的途径包括两方面,一方面在机体血小板被活化后会产生较多不同种的溶血磷脂,此时的溶血磷脂会转换为LPA,使其高表达;另一方面当癌细胞中的磷脂酶A2活性增强后会促进LPA的过量分泌,在卵巢组织中聚集,而卵巢组织中过量的LPA会重复产生LPA,形成恶性循环,介导卵巢癌的发生。本文结果显示,LPA在卵巢癌病人中高表达,且与病人疾病分期、分化程度以及是否存在淋巴结转移相关,此结果提示着,LPA参与卵巢癌的形成,可作为此类病人早期诊断的敏感指标。
本研究通过对HE4、CA199、LPA进行相关性分析,结果显示,HE4、CA199、LPA三者之间均呈现为正相关。说明HE4、CA199、LPA在卵巢癌的发展中起到重要的调控作用,可以作为卵巢癌早期诊治的敏感指标。
综上所述,HE4、CA199、LPA在卵巢癌病人中为高表达,且与病人临床分期、分化程度、有无淋巴结转移相关。
人附睾蛋白4、CA199、LPA在卵巢癌中的表达及与临床病理特征的相关性
Expression of human epididymal protein 4, CA199 and LPA in ovarian cancer, and its correlation with clinicopathological features
-
摘要:
目的探究人附睾蛋白4(HE4)、糖类抗原199(CA199)、人溶血磷脂酸(LPA)在卵巢癌中的表达及与临床病理特征的相关性。 方法选择卵巢癌病人140例作为卵巢癌组,同期选取因卵巢良性病变而行手术切除的病人120例作为卵巢良性病变组,并择同期行健康体检女性100名作为健康对照组。检测3组研究对象HE4、CA199、LPA水平,比较HE4、CA199、LPA在卵巢良性病变组与卵巢癌组卵巢组织中的阳性表达情况,分析HE4、CA199、LPA与卵巢癌病人临床病理特征的相关性,HE4、CA199、LPA之间的相关性。 结果血清HE4、CA199、血浆LPA水平,卵巢癌组血清均高于卵巢良性病变组和健康对照组,卵巢良性病变组均高于健康对照组(P < 0.05);HE4、CA199、LPA在卵巢癌组卵巢组织中的阳性表达率均高于卵巢良性病变组(P < 0.01)。HE4、CA199、LPA表达与卵巢癌病人病理类型、肿瘤直径无相关性(P>0.05);与卵巢癌病人临床分期、分化程度、有无淋巴结转移有相关性(P < 0.01),其中临床分期Ⅲ~Ⅳ期、低分化程度、有淋巴结转移的病人HE4、CA199、LPA表达水平较高。HE4与CA199之间呈正相关(r=0.183, P < 0.05),HE4与LPA之间呈正相关(r=0.216, P < 0.05),CA199与LPA之间呈正相关(r=0.209, P < 0.05)。 结论HE4、CA199、LPA在卵巢癌病人中为高表达,且与病人临床分期、分化程度、有无淋巴结转移相关。 Abstract:ObjectiveTo study the correlations among the expression levels of human epididymal protein 4(HE4), carbohydrate antigen 199(CA199) and human lysophosphatidic acid(LPA) in ovarian cancer, and its clinicopathological features. MethodsOne hundred and forty patients with ovarian cancer, 120 ovarian benign lesions patients treated with operation and 100 healthy women were divided into the ovarian cancer group, ovarian benign lesion group and healthy control group, respectively.The expression levels of HE4, CA199 and LPA in three groups were detected, the positive expression of HE4, CA199 and LPA between ovarian benign lesion group and ovarian cancer group were compared.The correlation of the HE4, CA199 and LPA with clinicopathological characteristics of ovarian cancer patients, and correlation among the expression of HE4, CA199 and LPA were analyzed. ResultsThe serum levels of HE4, CA199 and plasma LPA in ovarian cancer group were higher than those in benign ovarian lesion group and healthy control group(P < 0.05), and the positive rates of HE4, CA199 and LPA in ovarian cancer group were higher than those in benign ovarian lesion group(P < 0.01).The expression levels of HE4, CA199 and LPA were not correlated with the pathological type and diameter of ovarian cancer(P>0.05), but which were related to the clinical stage, differentiation degree and lymph node metastasis of ovarian cancer patients(P < 0.01).The expression levels of HE4, CA199 and LPA in patients with stage Ⅲ-Ⅳ, low differentiation and lymph node metastasis were higher.The HE4 level was positively correlated with CA199(r=0.183, P < 0.05), the HE4 level was positively correlated with LPA(r=0.216, P < 0.05), and the CA199 level was positively correlated with LPA(r=0.209, P < 0.05). ConclusionsThe expression levels of HE4, CA199 and LPA in ovarian cancer patients are high, which are related to the clinical stage, differentiation degree and lymph node metastasis. -
表 1 3组研究对象血清HE4、CA199、血浆LPA水平的比较(x±s)
分组 n HE4/(pmol/mL) CA199/(U/mL) LPA/(μmol/L) 健康对照组 100 44.23±5.46 13.12±1.13 2.03±0.24 卵巢良性病变组 120 59.68±10.24* 16.24±3.46* 2.29±0.98* 卵巢癌组 140 316.25±49.68*# 134.25±46.58*# 5.16±1.12*# F — 2 966.33 718.87 465.51 P — < 0.01 < 0.01 < 0.01 MS组内 — 1 004.189 849.128 0.825 q检验:与健康对照组比较*P < 0.05;与卵巢良性病变组比较#P < 0.05  下载: 导出CSV
下载: 导出CSV
表 2 HE4、CA199、LPA在卵巢良性病变组与卵巢癌组卵巢组织中的阳性表达情况比较[n;百分率(%)]
分组 n HE4 CA199 LPA 卵巢良性病变组 120 32(26.67) 28(23.33) 42(35.00) 卵巢癌组 140 129(92.14) 131(93.57) 118(84.29) χ2 — 117.49 134.19 66.31 P — < 0.01 < 0.01 < 0.01
下载: 导出CSV
表 3 HE4、CA199、LPA水平与卵巢癌病人临床病理特征的相关性分析(x±s)
指标 n HE4/(pmol/mL) CA199/(U/mL) LPA/(μmol/L) 临床分期 Ⅰ~Ⅱ期 36 246.38±68.59 48.62±9.65 3.46±0.24 Ⅲ~Ⅳ期 104 459.68±124.25 124.26±32.15 5.16±1.02 t — 9.78 13.87 9.88 P — < 0.01 < 0.01 < 0.01 分化程度 高 41 182.46±24.15 76.35±12.04 3.10±0.10 中 46 235.56±50.69△ 110.23±45.23△ 3.21±0.23△ 低 53 462.25±126.35△▲ 134.25±68.59△▲ 5.63±1.10△▲ F — 151.825 15.51 210.09 P — < 0.01 < 0.01 < 0.01 MS组内 — 7 073.723 2 499.970 0.480 病理类型 浆液性 76 245.26±42.25 124.25±35.26 4.13±0.65 非浆液性 64 252.25±43.26 125.26±35.49 4.16±0.68 t — 0.96 0.17 0.27 P — >0.05 >0.05 >0.05 淋巴结转移 有 62 398.56±102.12 135.49±58.25 5.86±1.10 无 78 265.35±53.27 109.58±23.58 3.45±0.24 t — 9.95 3.58 18.81 P — < 0.01 < 0.01 < 0.01 肿瘤直径/cm ≥5 59 232.16±68.59 124.25±15.36 4.10±0.21 < 5 81 231.25±72.16 126.35±16.69 4.13±0.20 t — 0.08 0.76 0.86 P — >0.05 >0.05 >0.05 q检验:与高分化相比较△P < 0.05;与中分化相比较▲P < 0.05
下载: 导出CSV
-
[1] 蒋绍艳, 常宏, 樊丹怡, 等. 淫羊藿苷对人卵巢癌细胞株的肿瘤恶性行为的抑制作用研究[J]. 四川大学学报(医学版), 2018, 49(4): 530. [2] 沈慧敏, 梁武凤, 杨君, 等. 人附睾蛋白4、溶血磷脂酸和糖类抗原125联合检测在上皮性卵巢癌诊断中的价值[J]. 新乡医学院学报, 2014, 31(11): 922. [3] 郑红云, 于奇, 申复进, 等. 血清HE4、CA125和CA199联合检测对卵巢癌早期诊断的临床研究[J]. 国际检验医学杂志, 2017, 38(19): 2680. doi: 10.3969/j.issn.1673-4130.2017.19.009 [4] 王婉, 胡倩倩, 杨文静, 等. 多西他赛联合奈达铂对上皮性卵巢癌患者血清LPA、CA199、CEA、白细胞介素及免疫功能的影响[J]. 海南医学院学报, 2016, 22(20): 2478. [5] 黄汉陵, 徐航, 向安琳. HE4、AFP、CA125和CEA在卵巢癌中的诊断意义[J]. 中国免疫学杂志, 2018, 34(11): 1712. doi: 10.3969/j.issn.1000-484X.2018.11.023 [6] 郭润梅, 杜蓉, 王丹, 等. 血清HE4、CA125浓度水平在预测上皮性卵巢癌预后中的价值[J]. 临床检验杂志, 2019, 37(2): 117. [7] 石慧, 胡建国. HE4、CA125联合D-二聚体检测对卵巢癌的诊断价值[J]. 蚌埠医学院学报, 2020, 45(4): 523. [8] KARACAN T, OZYUREK E, YESIRALIOGLU S, et al. Endometriomas with low-risk malignancy potential in ultrasonography with high human epididymis protein 4 and risk of ovarian malignancy algorithm: a cases series[J]. Gynecol Endocrinol, 2020, 36(2): 117. doi: 10.1080/09513590.2019.1653842 [9] 贺帅, 马黎明, 来艳君. HE4、CA125、SMRP检测联合ROMA在卵巢癌诊断中的应用[J]. 实用癌症杂志, 2019, 34(3): 362. doi: 10.3969/j.issn.1001-5930.2019.03.004 [10] 马书丽, 李静, 袁媛, 等. 卵巢上皮癌患者CA125和HE4水平及其临床意义分析[J]. 国际检验医学杂志, 2019, 40(14): 1759. doi: 10.3969/j.issn.1673-4130.2019.14.023 [11] GUO J, YU J, SONG X, et al. Serum CA125, CA199 and CEA combined detection for epithelial ovarian cancer diagnosis: a meta-analysis[J]. Open Med(Wars), 2017, 12: 131. doi: 10.1515/med-2017-0020 [12] 李炜, 智明春, 李贞爱, 等. CA125、CA199、CEA联合彩色多普勒超声诊断卵巢癌的临床价值[J]. 解放军预防医学杂志, 2018, 36(10): 1312. [13] 李丹妍, 王銮虹, 邱小华, 等. 血清CA125、CA199、AFP和CEA联合检测在卵巢癌诊断中的临床价值[J]. 中国妇幼保健, 2018, 33(8): 1731. [14] 林莉, 王金华. 肿瘤相关因子在卵巢癌中的表达及其与淋巴结转移相关性研究[J]. 中国临床药理学杂志, 2015, 31(22): 2211. [15] JESIONOWSKA A, CECERSKA-HERYC E, MATOSZKA N, et al. Lysophosphatidic acid signaling in ovarian cancer[J]. J Recept Signal Transduct Res, 2015, 35(6): 578. doi: 10.3109/10799893.2015.1026444 [16] 吴瑜霞, 杨秀华, 曾瑞兰, 等. LPA对比CA125在卵巢癌不同临床分期中表达水平分析[J]. 热带医学杂志, 2015, 15(6): 760. [17] SEO EJ, KWON YW, JANG IH, et al. Autotaxin regulates maintenance of ovarian cancer stem cells through lysophosphatidic acid-mediated autocrine mechanism[J]. Stem Cells, 2016, 34(3): 551. doi: 10.1002/stem.2279 [18] MINIS E, HOLCOMB K, SISTI G, et al. Evaluation of lysophosphatidic acid in vaginal fluid as a biomarker for ovarian cancer: a pilot study[J]. Eur J Obstet Gynecol Reprod Biol X, 2019, 2: 100012. doi: 10.1016/j.eurox.2019.100012 [19] JEONG KJ, PARK SY, CHO KH, et al. Correction: The Rho/ROCK pathway for lysophosphatidic acid-induced proteolytic enzyme expression and ovarian cancer cell invasion[J]. Oncogene, 2019, 38(25): 5108. doi: 10.1038/s41388-019-0769-7 -

 点击查看大图
点击查看大图

图(3)表(3)
计量
- 文章访问数: 4436
- HTML全文浏览量: 2181
- PDF下载量: 11
- 被引次数: 0
