

-
急性播散性脑脊髓炎(acute disseminated encephalomyelitis, ADEM)是一种中枢神经系统自身免疫性脱髓鞘性疾病,儿童为主要受累者。因本病临床症状非特异且缺乏有效的生化指标,故目前儿童ADEM的诊断缺乏金标准,预后判断困难;既往儿童ADEM的文献多是小样本量和短期随访,本文报道较大样本量和较长随访时间的研究结果,期望进一步阐释儿童ADEM的临床特点,并对随访到的患儿进行分组,对可能影响本病预后的多种因素进行分析。现作报道。
-
2012年1月至2018年7月我科收住确诊的ADEM患儿,共77例,其中男44例(57.1%),女33例(42.9%),男女比例4∶3;发病年龄4月14天至14岁。
-
参照国际儿童多发性硬化研究组(IPMSSG)儿童ADEM诊断标准[1],符合以下所有条件: (1)第1次多灶性临床中枢神经系统事件,推定原因为炎症性脱髓鞘。(2)不能用发热解释的脑病症状。(3)发病3个月或以上不出现新的临床或MRI病灶。(4)急性期(3月内)脑或脊髓MRI异常。(5)典型的脑MRI表现为:①弥散的、边界欠清晰的、较大的(>1~2 cm)病灶,主要累及脑白质;②脑白质区T1低信号病变少见;③深部灰质核团可存在病灶。(6)排除病原体直接感染疾病、遗传代谢疾病、结缔组织病及肿瘤等所致脑脊髓病。
-
回顾性分析患儿住院期间的临床资料,门诊及电话随访患儿情况。分组设计病例对照研究,分组依据[2]:痊愈组和不完全痊愈组,痊愈组随访时无症状,无治疗;不完全痊愈组遗留临床症状或病情反复(仍达不到其他免疫性疾病诊断指标),遗留症状包括:肢体不灵活或伴语言功能差,尿床,头痛,抽搐,包括死亡。对2组的性别、发病年龄、病前诱因、主要临床症状、脑脊液(CSF)白细胞及蛋白水平,四肢肌电图、头颅MRI进行统计分析。
-
采用χ2检验和Fisher′s精确概率法。
-
56例感染后发病,其中上呼吸道感染52例,肺炎3例(包括支原体肺炎1例),腹泻1例;3例有疫苗接种史无感染;4例同时有疫苗接种史及上呼吸道感染诱因;14例(18.2%)无明确诱因。
-
诱因:病前感染77.9%,疫苗接种9.1%;临床症状:发热39.0%,肢体活动障碍37.7%,惊厥33.8%,意识障碍24.7%,头痛头晕19.5%,二便障碍10.4%,口眼歪斜7.8%,视物不清5.2%,共济失调5.2%,精神行为异常3.9%;神经系统体征:肌肉减退37.7%,病理征23.4%,脑膜刺激征9.1%。
-
69例患儿入院后接受腰穿CSF检查,其中34例(49.3%)有核细胞数增高,16例(23.2 %)蛋白增高。15例CSF与血清同步送检寡克隆区带(OB)、碱性髓鞘蛋白(MBP),仅1例血清和CSF均OB阳性,该例患儿CSF常规、生化正常,其他14例血清和CSF的OB、MBP均为阴性,其中1例存在CSF的IgG鞘内合成。5例检测CSF及血清的髓鞘少突胶质细胞糖蛋白(MOG)抗体,CSF均阴性,2例血清阳性。16例检测血清支原体IgM抗体,其中10例阳性。6例检测CSF支原体IgM抗体,均为阴性。
-
55例入院后接受脑电图检查,36例(65.5%)异常,表现为轻重不等的背景慢波,偶见局灶性异常放电。29例接受肌电图检查,异常11例(37.9%),表现为双侧对称性CMAP波幅低,或运动感觉神经传导速度减慢,或F波波幅低或出波率低。15例患儿接受视觉诱发电位检查,7例(46.7%)有异常,表现为P100潜伏期延长或伴波形分化差。
-
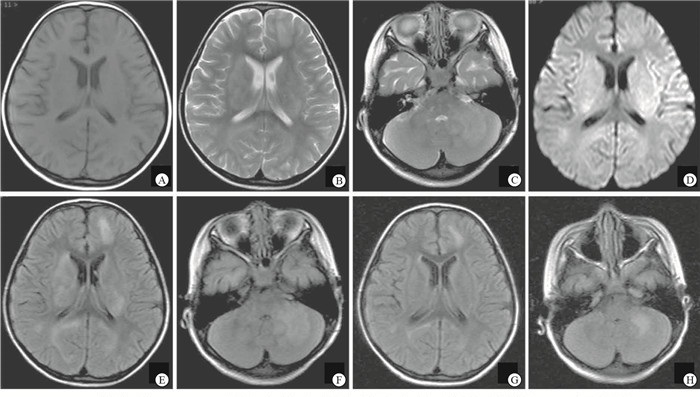
76例入院后接受头颅MRI检查,66例(86.8%)异常(见图 1),56例接受脊髓MRI检查,27例(48.2%)异常。10例头颅MRI正常患儿,依据脊髓MRI异常信号诊断。
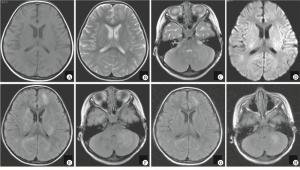
图 1 ADEM患儿(女,5岁3月龄)头颅MRI
-
75例患儿在对症、支持治疗基础上,采用免疫治疗方案,10例患儿仅用糖皮质激素治疗,3例患儿仅用免疫球蛋白治疗,62例患儿同时应用免疫球蛋白联合糖皮质激素治疗。应用糖皮质激素治疗患儿后续泼尼松1~2 mg·kg-1·d-1口服,逐渐减量,总疗程3~5月。
-
77例患儿,4例表现为ADEM多相型:第1例病史3年,停药2年半再发;第2例病史半年,停药10 d再发;第3例病史10个月,减药量过程中反复;第4例病史2个月,治疗好转后复查头颅MRI见新病灶。4例中有3例检测了CSF的OB、MBP和IgG鞘内合成,均正常;2例检测了CSF和血清MOG,1例为血清阳性、CSF阴性,另1例血清及CSF均为阴性。
-
随访到患儿41例,随访时间为病后6个月至6年6个月,根据随访结果分为2组:痊愈组和不完全痊愈组,其中痊愈组31例,患儿临床症状消失,无治疗;不完全痊愈组包括运动能力下降2例,病后尿床1例,抽搐伴语言运动能力下降1例,头痛1例,无症状、口服泼尼松治疗中1例,病情反复需继续治疗1例,严重双下肢无力、萎缩伴二便障碍1例,死亡2例(1例治疗稳定数月可上学,突发抽搐、呼吸衰竭死亡,另1例病情重,治疗中死亡)。
-
2组患儿性别、发病年龄、病前诱因、临床主要症状、CSF白细胞及蛋白水平、四肢肌电图、头颅MRI差异均无统计学意义(P>0.05) (见表 1)。
变量 痊愈组(n=31) 不完全痊愈组(n=10) χ2 P 性别 女 15(48.4) 6(60.0) 0.08 >0.05 男 16(51.6) 4(40.0) 年龄/岁 < 2 5(16.1) 3(30.0) — >0.05* 2~5 10(32.3) 2(20.0) >5 16(51.6) 5(50.0) 肢体活动障碍 11(35.5) 3(30.0) 0.00 >0.05 症状 惊厥 7(22.6) 4(40.0) 0.45 >0.05 意识障碍 7(22.6) 4(40.0) 0.45 >0.05 头痛头晕 7(22.6) 1(10.0) 0.17 >0.05 发热 10(32.3) 2(20.0) 0.12 >0.05 诱因 疫苗接种 1(3.2) 1(10.0) — >0.05* 前驱感染 19(61.3) 10(100.0) 3.76 >0.05 CSF白细胞 异常 15(53.6) 5(55.6) 0.00 >0.05 正常 13(46.4) 4(44.4) CSF蛋白 异常 8(28.6) 4(44.4) 1.15 >0.05 正常 20(71.4) 5(55.6) 四肢肌电图 异常 4(30.8) 3(75) 0.98 >0.05 正常 9(69.2) 1(25) 头颅MRI 有基底核或脑干病灶 11(36.7) 4(40) 0.00 >0.05 无基底核或脑干病灶 19(63.3) 6(60) *示Fisher′s确切概率法P值 表 1 41例随访患儿痊愈组与不完全痊愈组变量比较[n; 百分率(%)]
-
目前认为ADEM是由于某些病原体的氨基酸序列和人髓鞘蛋白的氨基酸序列相似,病原体感染后发生抗原抗体反应导致的免疫损伤性疾病,患儿常有病前感染或疫苗接种史。ADEM临床症状复杂多样、缺乏特异性,CSF及血液化验无明显特征性,影像学表现常为诊断的重要依据[3]。需与多发性硬化、视神经脊髓炎、急性横贯性脊髓炎、神经系统其他免疫或代谢性疾病等鉴别。治疗主要是糖皮质激素、免疫球蛋白和对症治疗。
本组患儿在发病诱因、临床症状构成、辅助检查情况、预后等与文献[4]报道基本一致。病前感染率77.9%,疫苗接种率9.1%。临床症状按发生频率排序:发热,肢体活动障碍,惊厥,意识障碍,头痛头晕,二便障碍,口眼歪斜,视物不清,共济失调,精神行为异常等,其中非特异症状以发热多见,病程中有发热,但临床症状体征不能用发热解释。ADEM患儿的CSF和血清中可检测到异常免疫球蛋白,这些免疫指标对鉴别诊断有一定意义[5]。本组少部分病例检测了CSF和血清OB、MBP、MOG及支原体IgM抗体这些免疫指标,阳性率低,符合儿童ADEM病因单纯、预后良好的特点。ADEM病灶广泛累及中枢,但近年不少同时存在周围神经损害的报道[6-7],本组肌电图检查异常率37.9%,证实周围神经损害的存在。本组病例头颅MRI阳性率86.8%,脊髓MRI阳性率48.2%,支持儿童ADEM的诊断以影像依据为重[8]。
ADEM多为单相病程,多相型ADEM指发生2次符合ADEM诊断标准的临床事件,2次间隔至少3个月,第2次事件可以是前一次的原病灶复发,也可以出现新的临床或MRI病灶[1]。KOELMA等[5]回顾性观察了228例ADEM病人,其中112例为儿童,认为儿童ADEM复发多数应诊断为多相型ADEM,成人更多可诊断为多发性硬化。PAPETTI等[9]研究发现CSF中存在OB是儿童ADEM向多发性硬化转化的预测指标。本组观察ADEM患儿77例,多相型4例,其中3例接受免疫指标检测,CSF的OB、MBP、IgG鞘内合成均正常,不支持多发性硬化诊断。
ADEM伴发视神经炎是儿童病人偶然的临床现象。本组中有4例单眼或双眼视力下降(不伴有脊髓异常信号),其中3例接受视觉诱发电位检测,均明显异常,1例CSF行OB、MBP及IgG抗体检测,未发现异常;随访到3例,均无病情反复、无视物不适感。儿童ADEM继发视神经炎预后良好,转化为多发性硬化的情况少,与KIM等[10]的报道一致。
MOG抗体疾病是新鉴定的中枢神经系统炎症状态[11],发病部位包括视神经、脊髓、脑干和脑。ADEM亦属MOG抗体疾病,因此有必要对ADEM患儿进行CSF和血清的MOG抗体检测。BAUMANN等[12]报道一组33例ADEM患儿,有19例MOG抗体阳性,抗体阳性的患儿除CSF细胞数偏高外,发病年龄、性别及临床症状与阴性患儿均无区别,并发现MOG抗体的存在代表预后良好。本组5例检测CSF及血清MOG抗体,并均成功随访,
CSF均阴性,2例血清阳性,发现血清阳性组与血清阴性组各有1例多相型ADEM患儿,余3例单相病程,无严重后遗症患儿。
儿童ADEM的预后判断困难,研究预后影响因素的文献较少,CSF中OB阳性者复发倾向高[9],MOG抗体阳性患儿预后好[12]。本组资料因检测免疫指标的病例数少,未进行免疫指标对预后影响的统计分析。我们把随访到的41例患儿分为痊愈组和不完全痊愈组,对性别,发病年龄,病前诱因,主要临床症状的肢体活动障碍、惊厥、意识障碍、头痛头晕、发热,CSF白细胞及蛋白水平,四肢肌电图,头颅MRI基底核或脑干病灶的差异进行了统计学分析,探寻这些常见指标是否能预测儿童ADEM的预后,结果显示这些指标2组间差异无统计学意义(P>0.05),不能预测预后。
本组资料属于回顾性研究,基于较多病例数及较长时间随访,可以总结出:儿童ADEM,急性或亚急性起病,脑病样表现,头颅或脊髓MRI异常为其主要诊断依据,大多数经免疫治疗效果良好,少数患儿病情反复或遗留后遗症状,偶有死亡。性别、发病年龄、病前诱因、主要临床症状、CSF白细胞及蛋白水平、四肢肌电图及头颅MRI差异不能预测儿童ADEM的预后。
儿童急性播散性脑脊髓炎临床特点及预后影响因素分析
Clinical analysis and influencing prognosis factors in 77 children with acute disseminated encephalomyelitis
-
摘要:
目的总结儿童急性播散性脑脊髓炎(acute disseminated encephalomyelitis,ADEM)的临床特点并分析影响预后的因素。 方法回顾性分析77例ADEM患儿的临床特点。随访到的患儿分为痊愈组和不完全痊愈组,对2组患儿的发病年龄、性别、诱因、主要临床症状、脑脊液白细胞及蛋白水平、四肢肌电图、头颅MRI进行统计分析,探寻预后影响因素。 结果77例中男44例,女33例,发病年龄4月14天至14岁。病前60例有感染诱因,7例有疫苗接种史,14例无明确诱因。主要临床症状:肢体活动障碍、惊厥、意识障碍、头痛头晕等,常伴非特异症状发热。头颅和脊髓MRI检查:76例接受头颅MRI检查,66例异常;56例接受脊髓MRI检查,27例异常;头颅MRI正常患儿脊髓MRI见病灶。随访到41例患儿,随访时间病后6个月至6年6个月,其中痊愈组31例,不完全痊愈组10例。2组患儿年龄、性别、诱因、主要临床症状、脑脊液白细胞及蛋白水平、四肢肌电图、头颅MRI的差异均无统计学意义(P>0.05)。 结论儿童ADEM,急性或亚急性起病,脑病样表现,头颅或脊髓MRI异常为其主要诊断依据,多数预后良好。性别、发病年龄、病前诱因、主要临床症状、脑脊液一般检查、四肢肌电图及头颅MRI差异对预后无影响。 Abstract:ObjectiveTo summarize the clinical features and analyze the factors of influencing prognosis in children with acute disseminated encephalomyelitis(ADEM). MethodsThe clinical features of children with ADEM retrospectively analyzed.The children patients were divided into the complete healing group and incomplete healing group.The age, gender, inducements, clinical symptoms, white cell and albumen level in cerebrospinal fluid, electromyogram in extremities and encephalic MRI were compared between two groups, and the factors of influencing prognosis were explored. ResultsA total of 77 patients(44 male and 33 female), aged range from 4 months 14 days to 14 years old, were investigated.Sixty cases with infection history, 7 cases with vaccination history and 14 cases without definite inducement were found.The major clinical symptoms included the motility disorders of extremities, eclampsia, conscious disturbance, headache and dizziness, and the patients often accompanied by non-specific symptoms of fever.The results of encephalic MRI in 76 cases showed that 66 cases were abnormity, and the results of spinal cord MRI in 56 cases showed that 27 cases were abnormity.The lesion in spinal cord was found in the patients with normal encephalic MRI.Forty-one children(including 31 cases of complete healing group and 10 cases of incomplete healing group) were followed up for 6 months to 6 years after illness.The differences of the age, gender, inducements, clinical symptoms, cerebrospinal fluid white blood cell count and protein level, electromyography of limbs and encephalic MRI between two groups were not statistically significant(P>0.05). ConclusionsThe acute or subacute onset, encephalopathy, MRI abnormalities in the cranial or spinal cord are the main diagnosis criteria, and the prognosis in most patients are good.The gender, age of onset, predisposition, main clinical symptoms, general examination of cerebrospinal fluid, electromyography of limbs and head MRI do not affect on the prognosis. -
Key words:
- acute disseminated encephalomyelitis /
- children /
- clinical features /
- follow-up /
- prognosis
-
表 1 41例随访患儿痊愈组与不完全痊愈组变量比较[n; 百分率(%)]
变量 痊愈组(n=31) 不完全痊愈组(n=10) χ2 P 性别 女 15(48.4) 6(60.0) 0.08 >0.05 男 16(51.6) 4(40.0) 年龄/岁 < 2 5(16.1) 3(30.0) — >0.05* 2~5 10(32.3) 2(20.0) >5 16(51.6) 5(50.0) 肢体活动障碍 11(35.5) 3(30.0) 0.00 >0.05 症状 惊厥 7(22.6) 4(40.0) 0.45 >0.05 意识障碍 7(22.6) 4(40.0) 0.45 >0.05 头痛头晕 7(22.6) 1(10.0) 0.17 >0.05 发热 10(32.3) 2(20.0) 0.12 >0.05 诱因 疫苗接种 1(3.2) 1(10.0) — >0.05* 前驱感染 19(61.3) 10(100.0) 3.76 >0.05 CSF白细胞 异常 15(53.6) 5(55.6) 0.00 >0.05 正常 13(46.4) 4(44.4) CSF蛋白 异常 8(28.6) 4(44.4) 1.15 >0.05 正常 20(71.4) 5(55.6) 四肢肌电图 异常 4(30.8) 3(75) 0.98 >0.05 正常 9(69.2) 1(25) 头颅MRI 有基底核或脑干病灶 11(36.7) 4(40) 0.00 >0.05 无基底核或脑干病灶 19(63.3) 6(60) *示Fisher′s确切概率法P值  下载: 导出CSV
下载: 导出CSV
-
[1] KRUPP LB, TARDIEU M, AMATO MP, et al. International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: revisions to the 2007 definitions[J]. Mult Scler, 2013, 19(10): 1261. doi: 10.1177/1352458513484547 [2] GANEROD J, AMBROSE HE, DAVIES NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study[J]. Lancet Infect Dis, 2010, 10(12): 835. doi: 10.1016/S1473-3099(10)70222-X [3] 徐敏, 汤继宏, 师晓燕, 等. 急性播散性脑脊髓炎临床及影像学随访研究[J]. 中华实用儿科临床杂志, 2017, 32(12): 936. doi: 10.3760/cma.j.issn.2095-428X.2017.12.014 [4] GOWDA VK, SHETTY D, MADIVALA BV, et al. Clinical and radiological profiles, treatment, and outcome of pediatric acquired demyelinating disorders of central nervous system[J]. J Pediatr Neurosci, 2019, 14(2): 76. doi: 10.4103/jpn.JPN_62_18 [5] KOELMAN DL, CHAHIN S, MAR SS, et al. Acute disseminated encephalomyelitis in 228 patients: A retrospective, multicenter US study[J]. Neurology, 2016, 86(22): 2085. doi: 10.1212/WNL.0000000000002723 [6] DESENA A, GRAVES D, MORRISS MC, et al. Transverse myelitis plus syndrome and acute disseminated encephalomyelitis plus syndrome: a case series of 5 children[J]. JAMA Neurol, 2014, 71(5): 624. doi: 10.1001/jamaneurol.2013.5323 [7] TRINDADE RAR, KLAES AINM DUARTE JÁ. The many faces of demyelinating diseases: acute disseminated encephalomyelitis and Guillain-Barré syndrome in the same patient[J]. Arq Neuropsiquiatr, 2017, 75(5): 324. doi: 10.1590/0004-282x20170037 [8] BOESEN MS, BLINKENBERG M, KOCH-HENRIKSEN N, et al. Implications of the International Paediatric Multiple Sclerosis Study Group consensus criteria for paediatric acute disseminated encephalomyelitis: a nationwide validation study[J]. Dev Med Child Neurol, 2018, 60(11): 1123. doi: 10.1111/dmcn.13798 [9] PAPETTI L, FIGÀ TALAMANCA L, SPALICE A, et al. Predictors of evolution into multiple sclerosis after a first acute demyelinating syndrome in children and adolescents[J]. Front Neurol, 2019, 9: 1156. doi: 10.3389/fneur.2018.01156 [10] KIM YM, KIM HY, CHO MJ, et al. Optic neuritis in korean children: low risk of subsequent multiple sclerosis[J]. Pediatr Neurol, 2015, 53(3): 221. doi: 10.1016/j.pediatrneurol.2015.05.010 [11] JURYNCZYK M, MESSINA S, WOODHALL MR, et al. Clinical presentation and prognosis in MOG-antibody disease: a UK study[J]. Brain, 2017, 140(12): 3128. doi: 10.1093/brain/awx276 [12] BAUMANN M, HÄUSLER M, EISENKÖLBL A, et al. Clinical and neuroradiological differences of paediatric acute disseminating encephalomyelitis with and without antibodies to the myelin oligodendrocyte glycoprotein[J]. J Neurol Neurosurg Psychiatry, 2015, 86(3): 265. doi: 10.1136/jnnp-2014-308346 -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 3465
- HTML全文浏览量: 2004
- PDF下载量: 7
- 被引次数: 0
