

-
副乳癌(accessory breast cancer,ABC)系指正常乳腺以外出现乳腺组织,占女性乳腺疾病的1%~2%,占副乳症的1%~5%,是一种少见的乳腺疾病[1],ABC病人以腋下肿块(多为腋窝下或腋前无痛性肿物)为首发症状,由于腋窝处血液和淋巴结丰富易出现早期转移,临床发现时多已处于晚期,因此ABC生存率明显低于常规胸部乳腺癌(mammary cancer,MC)[2]。与常规胸部乳腺一样,副乳也受内分泌影响,可出现与常规胸部乳腺同样的良恶性肿瘤(如小叶增生、导管扩张及纤维腺瘤等),易与乳腺外肿瘤相混淆[3]。目前磁共振成像扫描在ABC诊断中价值尚不明确,但研究[4]证实超声引导下细针吸取细胞学或粗针穿刺活检有助于ABC的早期诊断,因此临床中可从分子水平上探究ABC与常规胸部MC的有效诊断方案。转录因子发状分裂相关增强子1(hairy and enhancer of split1,HES1)是细胞分化、细胞周期调控的重要因子,在肿瘤疾病中呈高表达[5],其在ABC中表达情况国内尚未见报道;人类表皮生长因子受体2(human epidermal growth factor receptor 2,HER2)是决定MC分子分型的重要分子生物学标志物,其在常规胸部MC组织中表达的研究[6]较多见,但有关其在ABC与常规胸部MC中表达差异的研究并不多见。本文旨在探讨ABC和常规胸部MC HES1、HER2表达差异及其与临床病理特征的关系,以期为ABC诊治提供参考信息。
-
选取2012年1月至2016年1月我院确诊的ABC病人(ABC组)和常规胸部MC病人(MC组),各30例。回顾性分析病人的临床诊治及随访资料。其中ABC组女28例,男2例;年龄30~69岁;腋窝下或腋前ABC 29例、腹股沟处ABC 1例。MC组均为女性,年龄28~72岁。
纳入标准:(1)符合ABC或MC诊断标准[7],术后病理证实有明确的ABC或常规胸部MC;(2)年龄≥18岁,症状可见有或无肿块疼痛、肿胀、泌乳、溢液、破溃等;(3)接受手术治疗;(4)临床资料完善;(5)入组前未接受ABC、常规MC放化疗药物治疗。
排除标准:(1)合并其他脏器恶性肿瘤;(2)入选前已进行过放射治疗、化学治疗或其他综合治疗;(3)入院时已发生远处转移而无法手术;(4)相关资料欠缺。
-
ABC组行ABC扩大区段切除加腋窝淋巴结清扫10例,乳腺癌改良根治术11例,乳腺癌根治术6例,ABC区段切除术3例;MC组行乳腺癌改良根治术20例,乳腺癌根治术6例,保乳术4例。术后均严格参照相关指南进行术后化疗、放疗及内分泌治疗。2组术后病人的放化疗和内分泌治疗均参照MC治疗指南[7]进行。术后随访2组病人复发情况。
-
免疫组织化学法检测:术前取ABC病人、MC病人癌组织标本,常规石蜡包埋切片,免疫组织化学法检测ABC、常规MC组织中HES1、HER2表达。步骤:脱蜡水化后,37 ℃ 3%H2O2温箱孵育,阻断内源性过氧化物酶,PBS液重复洗涤3次后柠檬酸缓冲液(pH值6.0)微波修复,室温冷却30 min;非免疫动物血清37 ℃温箱封闭,PBS液重复洗涤3次,滴加一抗、二抗,辣根过氧化酶标记链霉素亲和复合物,37 ℃温箱孵育后,DAB染色、苏木素复染、脱水、透明、封片。由两位病理科医师采用双盲法,依据染色强度(阴性、弱性、适中、强性对应计0、1、2、3分)、阳性染色细胞百分比(0%、>0%~10%、>10%~25%、>25%~50%、>50%对应计0、1、2、3、4分)评定免疫组织化学分析结果,染色强度+阳性染色细胞百分比总分4~8分提示HES1或HER2阳性。
-
采用χ2检验和Fisher′s确切概率法。
-
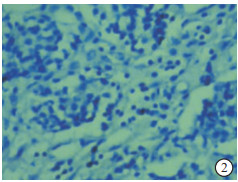
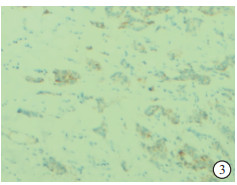
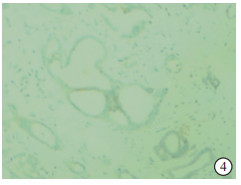
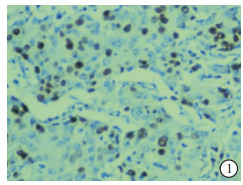
2组病人HES1和HER2阳性表达率差异均无统计学意义(P>0.05)(见图 1~4、表 1)。
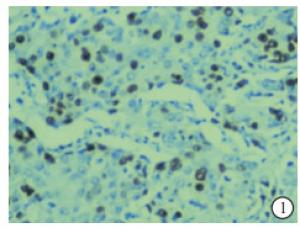
图 1 ABC组织中HES1阳性表达
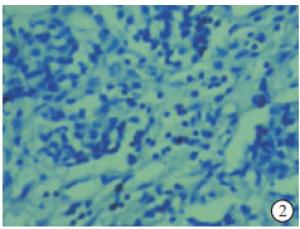
图 2 MC组织中HES1阳性表达

图 3 ABC组织中HER2表达
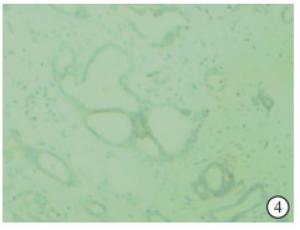
图 4 MC组织中HER2表达
分组 n HES1阳性 HER2阳性 ABC组 30 9(30.00) 16(53.33) MC组 30 12(40.00) 12(40.00) χ2 — 0.66 1.07 P — >0.05 >0.05 表 1 HES1、HER2在不同组织中的表达情况[n; 百分率(%)]
-
ABC组和MC组病人HES1阳性表达率在不同病理类型、组织学分级、临床分期和是否淋巴结转移、三阴乳腺癌间差异均有统计学意义(P < 0.05~P < 0.01),ABC组HES1阳性表达率在是否复发病人间差异亦有统计学意义(P < 0.05)。2组组间HES1阳性表达在淋巴结转移分布上差异有统计学意义(P < 0.05)(见表 2)。
临床特征 ABC组 MC组 n HES1阳性 χ2 P n HES1阳性 χ2 P 性别 男
女2
281
80.03 >0.05 0
300
12— — 年龄/岁 ≤60
>6018
127
20.80 >0.05 20
108
40.16 >0.05 月经情况 绝经期
绝经后13
175
40.23 >0.05 12
186
60.28 >0.05 病理类型 浸润性导管癌
其他16
148
14.65 < 0.05 17
1310
25.79 < 0.05 组织学分级/级 Ⅰ+Ⅱ
Ⅲ21
92
710.91 < 0.01 20
85
76.74 < 0.01 临床分期/期 Ⅰ 15 0 17 3 Ⅳ
Ⅲ8
42
422.86 < 0.01 7
33
312.56 < 0.01 Ⅳ 3 3 3 3 淋巴结转移 有
无24
63
617.50 < 0.05 23
712
04.10 < 0.05 三阴乳腺癌 是
否14
199
013.71 < 0.01 13
1711
115.89 < 0.01 复发 是
否11
197
27.00 < 0.05 4
263
90.97 >0.05 表 2 不同病理特征病人HES1阳性表达情况(n)
-
ABC病人HER2阳性表达率在不同病理类型、组织学分级、临床分期和是否三阴乳腺癌及复发间差异均有统计学意义(P < 0.05~P < 0.01);MC病人HER2阳性表达率在不同病理类型、临床分期和是否淋巴结转移、三阴乳腺癌间差异均有统计学意义(P < 0.01)。2组组间HER2阳性表达在病理类型分布上差异有统计学意义(P < 0.01)(见表 3)。
临床特征 ABC组 MC组 n HES2阳性 χ2 >P n HES2阳性 χ2 P 性别 男
女2
281
150.40 >0.05 0
300
12— — 年龄/岁 ≤60
>6018
207
90.15 >0.05 20
107
50.16 >0.05 月经情况 绝经期
绝经后13
176
100.48 >0.05 12
186
60.28 >0.05 病理类型 浸润性导管癌
其他16
144
1211.06 < 0.05 17
1312
015.29 < 0.01 组织学分级/级 Ⅰ+Ⅱ
Ⅲ21
915
16.95 < 0.01 20
811
11.41 >0.05 临床分期/期 Ⅰ 15 2 17 1 Ⅳ
Ⅲ8
47
419.52 < 0.05 7
35
320.13 < 0.01 Ⅳ 3 3 3 3 淋巴结转移 有
无24
612
40.08 >0.05 23
76
65.66 < 0.01 三阴乳腺癌 是
否14
1614
222.97 < 0.01 13
1712
026.15 < 0.01 复发 是
否11
1911
19— < 0.01** 4
262
100.01 >0.05 **示Fisher′s确切概率法 表 3 2组不同病理特征病人HES1阳性表达情况(n)
-
虽ABC发病率较低,但与常规MC病人相比,早期ABC临床症状缺乏特异性,且生化指标无明显变化,初步诊断易误诊为乳腺腋尾部癌、乳腺癌的腋窝淋巴结转移、隐性乳腺癌等,此外ABC位置较为特殊,其在钼靶上难以完全显示,临床当中尚缺乏行之有效的ABC早期诊断手段。随着分子生物学迅速发展,近年来分子生物学标志物在乳腺癌诊断中的研究日益广泛[8]。HES1属于碱性螺旋-环-螺旋基因转录抑制因子之一,有抑制组织细胞特征性分化的作用,可直接影响细胞分化以及增殖、细胞凋亡。研究[9]表明,HES1可阻碍神经干细胞以及小肠前体细胞分化,确保其保持未分化状态。国内外学者[10-11]研究证实HES1在卵巢癌、结肠癌、非小细胞肺癌等恶性肿瘤中呈高表达,且其表达水平与病人预后密切相关。HER2基因属于一种表皮生长因子受体家族成员,主要定位于染色体17q12-21.32,其可激活下游酪氨酸激酶使之磷酸化,有效调节肿瘤细胞增殖。研究[6]证实,HER2在乳腺癌组织中高表达往往预示着复发转移风险高、预后差。鉴于此,分析ABC病人HES1、HER2表达与常规胸部MC病人的差异及其与病理特征的关系,将有望为ABC术前诊断及预后评估提供参考。
既往报道[12-13]显示,HES1作为肿瘤细胞关键转录因子,其异常表达与肿瘤疾病发生、细胞分化、肿瘤恶性程度、肿瘤干细胞的成瘤性等生理及病理变化紧密相关;HER2表达与乳腺癌病人淋巴结转移、肿块大小、病理学分级间亦具有明显的相关性。本研究发现,ABC与MC组织中HES1、HER2阳性表达率无明显差异,而ABC组/MC组组内HES1阳性表达率在不同病理类型、组织学分级、临床分期、淋巴结转移、三阴乳腺癌病理特征间差异均有统计学意义。其中浸润性导管癌、三阴乳腺癌具更高的阳性表达率,可能是由于浸润性导管癌、三阴乳腺癌恶性程度更高,且随临床分期增高,淋巴结转移、肿瘤细胞浸润转移范围也更大,故而浸润性导管癌、三阴乳腺癌、临床分期高、组织学分级越高,以及合并淋巴结转移的ABC、常规胸部MC病人癌组织中HES1、HER2阳性表达率更高[14]。本研究结果显示,ABC组、MC组组间HES1阳性表达率在是否淋巴结转移间差异显著,表明HES1阳性表达率与ABC和MC病理特征密切相关;ABC病人HES1阳性表达率越高,其组织学分级越高和临床分期越晚,因HES1表达与ABC的侵袭能力有明显相关性,其可通过异常调控ABC干细胞自我更新能力,从而有效促进癌细胞增殖及转移,表现为组织学分级及临床分期晚,与早期李晓瑛等[15]研究指出的在乳腺癌病人中HES1阳性表达与TNM分期显著正相关的结论类似。本研究结果还显示,ABC组内HER2阳性表达率在不同病理类型、组织学分级、临床分期、三阴乳腺癌、复发病理特征间差异显著,而MC组内HER2阳性表达率在不同病理类型、临床分期、淋巴结转移、三阴乳腺癌病理特征间差异显著,提示ABC病人术前HER2阳性表达率越高,浸润性导管癌、三阴乳腺癌及复发可能性越高,而MC病人HER2阳性表达率越高,三阴乳腺癌风险越高,与早期学者[16]研究指出的乳腺癌病人中HER2表达与乳腺癌病理类型、三阴乳腺癌及复发密切相关的结论基本相符。2组组间HER2阳性表达率在病理类型分布上差异显著,提示或可通过不同病理类型病人HER2阳性表达率对两种乳腺癌进行鉴别。HER2其受体蛋白可通过同源或异源二聚体方式发生偶联,有效激活下游酪氨酸激酶使其磷酸化,促进肿瘤增殖,在肿瘤病理类型、恶性程度及预后中有一定预测价值[17]。
综上,术前ABC病人与MC病人HES1、HER2阳性表达率无明显差异,但术前HES1、HER2阳性表达率在预测ABC病人、MC病人病理特征方面可能有一定积极作用,可为临床合理治疗方案的制定提供参考。
副乳癌和常规胸部乳腺癌HES1、HER2表达差异及临床病理特征分析
Differential expression of HES1 and HER2 and analysis of clinicopathological features between accessory breast cancer and routine mammary cancer
-
摘要:
目的探讨副乳癌(ABC)和常规胸部乳腺癌(MC)转录因子发状分裂相关增强子1(HES1)、人类表皮生长因子受体2(HER2)表达差异及其与临床病理特征的关系。 方法回顾性分析30例ABC和30例MC病人的临床资料、病理资料和肿瘤组织HES1、HER2表达情况及随访资料,并进行统计分析。 结果ABC组HES1、HER2阳性表达率分别为30.00%、53.33%,MC组为40.00%、40.00%,2组HES1和HER2阳性率差异均无统计学意义(P>0.05)。ABC组和MC组病人HES1阳性表达率在不同病理类型、组织学分级、临床分期和是否淋巴结转移、三阴乳腺癌间差异均有统计学意义(P < 0.05~P < 0.01),ABC组HES1阳性表达率在是否复发病人间差异亦有统计学意义(P < 0.05)。ABC病人HER2阳性表达率在不同病理类型、组织学分级、临床分期和是否三阴乳腺癌及复发间差异均有统计学意义(P < 0.05~P < 0.01);MC病人HER2阳性表达率在不同病理类型、临床分期和是否淋巴结转移、三阴乳腺癌间差异均有统计学意义(P < 0.01)。 结论术前HES1、HER2阳性表达率可一定程度上反映ABC、MC病人病理特征,为合理手术方案的选择提供参考。 -
关键词:
- 乳腺肿瘤 /
- 转录因子发状分裂相关增强子1 /
- 人类表皮生长因子受体2
Abstract:ObjectiveTo investigate the differences in the expression of hairy and enhancer of split 1(HES1) and human epidermal growth factor receptor 2(HER2) in accessory breast cancer(ABC) and routine mammary cancer(MC) and their relationship with clinicopathological features. MethodsThe clinical data, pathological data, expression of HES1 and HER2 in cancer tissues and follow-up data of 30 patients with ABC and 30 patients with MC were analyzed retrospectively and evaluated statistically. ResultsThe positive expression rates of HES1 and HER2 in ABC group were 30.00% and 53.33%, respectively, which were 40.00% and 40.00% in MC group, respectively, and the difference of which was not statistically significant(P>0.05).There were significant differences in the positive expression rate of HES1 between ABC group and MC group in different pathological type, histological grades, clinical stage, lymph node metastasis and triple negative breast cancer(P < 0.05 to P < 0.01).The positive expression rate of HES1 in ABC group was also statistically significant between patients with recurrence or not(P < 0.05).The positive expression rate of HER2 in ABC patients was statistically significant among different pathological type, histological grade, clinical stage, triple negative breast cancer and recurrence or not(P < 0.05 to P < 0.01).The positive expression rate of HER2 in MC patients was statistically significant among different pathological type, clinical stage, lymph node metastasis or not and triple negative breast cancer(P < 0.01). ConclusionsThe positive expression rates of HES1 and HER2 before surgery can reflect the pathological features of ABC and MC patients to a certain extent, and provide reference for the selection of reasonable surgical plans. -
表 1 HES1、HER2在不同组织中的表达情况[n; 百分率(%)]
分组 n HES1阳性 HER2阳性 ABC组 30 9(30.00) 16(53.33) MC组 30 12(40.00) 12(40.00) χ2 — 0.66 1.07 P — >0.05 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 不同病理特征病人HES1阳性表达情况(n)
临床特征 ABC组 MC组 n HES1阳性 χ2 P n HES1阳性 χ2 P 性别 男
女2
281
80.03 >0.05 0
300
12— — 年龄/岁 ≤60
>6018
127
20.80 >0.05 20
108
40.16 >0.05 月经情况 绝经期
绝经后13
175
40.23 >0.05 12
186
60.28 >0.05 病理类型 浸润性导管癌
其他16
148
14.65 < 0.05 17
1310
25.79 < 0.05 组织学分级/级 Ⅰ+Ⅱ
Ⅲ21
92
710.91 < 0.01 20
85
76.74 < 0.01 临床分期/期 Ⅰ 15 0 17 3 Ⅳ
Ⅲ8
42
422.86 < 0.01 7
33
312.56 < 0.01 Ⅳ 3 3 3 3 淋巴结转移 有
无24
63
617.50 < 0.05 23
712
04.10 < 0.05 三阴乳腺癌 是
否14
199
013.71 < 0.01 13
1711
115.89 < 0.01 复发 是
否11
197
27.00 < 0.05 4
263
90.97 >0.05
下载: 导出CSV
表 3 2组不同病理特征病人HES1阳性表达情况(n)
临床特征 ABC组 MC组 n HES2阳性 χ2 >P n HES2阳性 χ2 P 性别 男
女2
281
150.40 >0.05 0
300
12— — 年龄/岁 ≤60
>6018
207
90.15 >0.05 20
107
50.16 >0.05 月经情况 绝经期
绝经后13
176
100.48 >0.05 12
186
60.28 >0.05 病理类型 浸润性导管癌
其他16
144
1211.06 < 0.05 17
1312
015.29 < 0.01 组织学分级/级 Ⅰ+Ⅱ
Ⅲ21
915
16.95 < 0.01 20
811
11.41 >0.05 临床分期/期 Ⅰ 15 2 17 1 Ⅳ
Ⅲ8
47
419.52 < 0.05 7
35
320.13 < 0.01 Ⅳ 3 3 3 3 淋巴结转移 有
无24
612
40.08 >0.05 23
76
65.66 < 0.01 三阴乳腺癌 是
否14
1614
222.97 < 0.01 13
1712
026.15 < 0.01 复发 是
否11
1911
19— < 0.01** 4
262
100.01 >0.05 **示Fisher′s确切概率法
下载: 导出CSV
-
[1] 刘晓, 桑晓旻, 刘红. 采用保留乳腺方式治疗副乳腺癌的临床分析[J]. 中国肿瘤临床, 2014, 41(7): 453. doi: 10.3969/j.issn.1000-8179.20132168 [2] 张硕, 汪孟森, 于甬华. 副乳腺癌诊治研究[J]. 中华肿瘤防治杂志, 2014, 21(15): 1208. [3] DEL RDI, TORRES LM, CEREZO TE, et al. Accessory joint and neural mobilizations for shoulder range of motion restriction after breast cancer surgery: A pilot randomized clinical trial[J]. J Chir Med, 2017, 16(1): 31. [4] 田秀芳, 翟震, 智英辉, 等. 副乳癌与常规胸部乳腺癌的临床病理特征及预后比较[J]. 山东医药, 2013, 53(13): 76. doi: 10.3969/j.issn.1002-266X.2013.13.028 [5] SUN L, KE J, HE Z, et al. HES1 promotes colorectal cancer cell resistance to 5-Fu by inducing of EMT and ABC transporter proteins[J]. J Cancer, 2017, 8(14): 2802. doi: 10.7150/jca.19142 [6] AHMED N, BRAWLEY V, HEGDE M, et al. HER2-specific chimeric antigen receptor-modified virus-specific T cells for progressive glioblastoma: A phase 1 dose-escalation Trial[J]. JAMA Oncol, 2017, 3(8): 1094. doi: 10.1001/jamaoncol.2017.0184 [7] 邵志敏, 沈镇宙. 乳腺肿瘤学[M]. 上海: 复旦大学出版社, 2013: 609. [8] 魏娅. 双侧原发乳腺癌的临床病理特点及生存状况[J]. 中国现代普通外科进展, 2018, 21(1): 58. [9] 洪磊, 周继红, 李伟, 等. Hes1在烟草诱导人支气管上皮细胞恶性转化过程中的作用[J]. 中国病理生理杂志, 2017, 33(7): 1153. doi: 10.3969/j.issn.1000-4718.2017.07.001 [10] 王春斐, 桂忠娜, 田强, 等. 胃癌组织中Notch1、Jagged1、Hes1的表达及临床意义[J]. 肿瘤学杂志, 2018, 24(2): 91. [11] GOTO N, UEO T, FUKUDA A, et al. Distinct roles of Hes1 in normal stem cells and tumor stem-like cells of the intestine[J]. Cancer Res, 2017, 77(13): 3442. doi: 10.1158/0008-5472.CAN-16-3192 [12] 胡慧, 刘倩, 徐玲, 等. 乳腺癌临床病理分类与临床病理特征研究[J]. 中华外科杂志, 2014, 52(2): 113. doi: 10.3760/cma.j.issn.0529-5815.2014.02.008 [13] 杨雅洁, 孙艳花. 乳腺癌组织中HER2的表达及其与临床病理特征的关系[J]. 南昌大学学报(医学版), 2018, 58(1): 55. [14] 龚慧青, 李云, 戴丽花. 2008-2012年上海市龙柏社区"六癌"流行病学调查分析[J]. 中国全科医学, 2014, 19(27): 3235. doi: 10.3969/j.issn.1007-9572.2014.27.019 [15] 李晓瑛, 曹彧, 金锋. 乳腺癌中HES1的表达情况及与生存预后的相关性[J]. 现代肿瘤医学, 2018, 26(6): 872. doi: 10.3969/j.issn.1672-4992.2018.06.014 [16] 李慧慧, 马飞, 曾瑄. 乳腺癌HER-2的表达与临床病理特征的关系[J]. 中华医学杂志, 2011, 91(2): 76. doi: 10.3760/cma.j.issn.0376-2491.2011.02.003 [17] 范小超, 杨奔, 左文述. 乳腺癌原发灶和转移灶激素受体与HER2表达差异及其影响因素[J]. 中华肿瘤防治杂志, 2017, 24(1): 65. -

 点击查看大图
点击查看大图
图(4)表(3)
计量
- 文章访问数: 3563
- HTML全文浏览量: 2062
- PDF下载量: 9
- 被引次数: 0
