



-
如今,随着人们健康体检意识的增强与超声诊断技术的提高,甲状腺癌检出率逐年增加[1],在4种病理类型中,最常见的病理类型为乳头状癌(papillary thyroid carcinoma,PTC),占80%以上,其中女性为主。世界卫生组织将直径≤10 mm的PTC定义为甲状腺微小乳头状癌(papillary thyroid microcarcinoma,PTMC),目前对PTMC的治疗首选为手术治疗[2]。传统手术会在颈部留下明显的瘢痕,给病人带来一定心理创伤,无法满足年轻病人对美的追求。腔镜技术的出现,因其可将切口隐蔽,越来越受病人与外科医生的喜欢。随着器械的改进与医生经验的提高,腔镜甲状腺技术从运用于良性甲状腺肿瘤到恶性甲状腺肿瘤,甚至颈侧区淋巴结清扫[3-4]。本研究回顾性分析蚌埠医学院第一附属医院肿瘤外科甲乳病区从2019年6月至2020年4月完成免充气经腋窝入路(腔镜组)PTMC 35例与传统开放手术(开放组)45例临床资料,并进行随访至少3个月,就此术式与疗效作一报道。
-
收集我科甲乳病区手术的80例PTMC临床资料,其中腔镜组35例,开放组45例。术前病人均行甲状腺激素、甲状旁腺激素、降钙素、颈部彩超等检查,明确手术指征及手术禁忌证,术中冷冻与术后病理均示为PTMC。术前告知病人与家属腔镜与开放术式的优缺点,根据病人意愿选择术式并签署知情同意书。
纳入标准:(1)甲状腺单侧病变;(2)结节影像学测量≤10 mm;(3)无颈侧区淋巴结转移或远处转移;(4)无颈部手术史或放疗史;(5)无胸骨后甲状腺肿物;(6)有美容需求。排除标准:(1)颈部手术或放疗史;(2)颈侧区淋巴结转移;(3)合并甲状腺炎或甲状腺功能亢进;(4)患心脑血管疾病需要进一步治疗;(5)肿块侵及周围组织。
-
2组均采用甲状腺患侧腺叶+峡部切除+中央区淋巴结清扫。
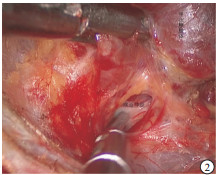
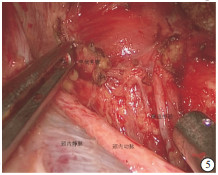
腔镜组:气管插管全麻。病人取仰卧位,颈肩部垫高,头偏向健侧;病人上肢外展并固定,显露腋窝,标记笔画出手术操作范围,显示器放置于主刀对面。常规消毒铺巾后,顺着腋窝皮肤褶皱作一4 cm左右斜行切口。顺着切口,用电刀在胸大肌表面游离皮瓣,然后在切口上方远心段,作一5 mm切口,置入Trocar,作为操作孔。将专用拉钩置入切口,固定拉钩,并接上吸引器吸烟。术者在胸大肌表面用超声刀沿着肌肉筋膜游离皮瓣,游离皮瓣跨过锁骨后,在颈阔肌深面显露胸锁乳突肌并找到胸骨头与锁骨头间隙(见图 1),适当分离后,用拉钩将胸骨头拉起,分离至显露病人颈前带状肌与甲状舌骨肌交点。用超声刀先从颈前带状肌外侧缘进行分离,调节专用拉钩拉起带状肌并固定好,显露术腔,暴露患侧甲状腺,内侧至峡部,上达甲状腺上极,下至胸锁关节水平。术者探查患侧甲状腺后,根据术野情况与操作习惯,从而采取先断上极或先断下极。一般先用超声刀在甲状腺外侧沿着被膜精细化解剖分离显露外侧缘,钝性分离解剖显露上极血管,再用超声刀紧贴甲状腺上极切断上极血管。接着将腺体推向对侧,从甲状腺外侧用分离钳解剖显露出喉返神经与下极血管(见图 2),再用超声刀切断甲状腺下极与下极血管。将患侧甲状腺向内侧提起,可充分显露气管、食管,解剖显露喉返神经全程,用超声刀切断甲状腺悬韧带,超声刀刀头需远离喉返神经并保持距离>3 mm,并及时用0.9%氯化钠溶液冲洗降温,最后用超声刀在靠近患侧腺体凝闭离断峡部(见图 3)。将腺体装入标本袋,完整取出患侧甲状腺,将标本送检进行冰冻,明确病变性质,再进行峡部切除与中央区淋巴结清扫(见图 4)。最后用0.9%氯化钠溶液冲洗术腔,创面彻底止血,并再次探查喉返神经完整性,并确保甲状旁腺完整与良好血供(见图 5)。腔内无需缝合,放置引流管1根从腋窝引出,撤去拉钩,缝合皮肤,结束手术。
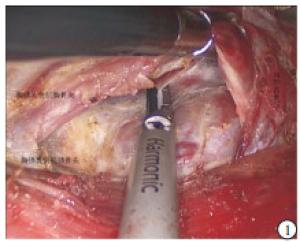
图 1 打开胸锁乳突肌的胸骨头与锁骨头

图 2 显露喉返神经

图 3 切断甲状腺峡部
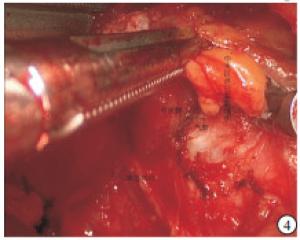
图 4 切除中央区淋巴脂肪组织

图 5 冲洗后的术野
开放组:气管插管麻醉成功后,取仰卧位,在胸骨上切迹约两横指处切一5 cm左右切口,先游离皮瓣,再切开颈白线,显露甲状腺后,凝闭离断甲状腺上、下极及周围血管,常规显露喉返神经,注意保护甲状旁腺,切除甲状腺,送冷冻,明确性质,在切除峡部与清扫中央区淋巴结,常规放置1根引流管,关闭术腔。
-
术中指标:手术时间,术中出血量,中央区淋巴结情况;术后指标:术后第1天引流量,术后第3天颈部视觉模拟评分(VAS),住院时间,术后住院时间;术后并发症:切口感染,术后出血,饮水呛咳,淋巴漏,食管、气管损伤,短暂性喉返神经麻痹,短暂性甲状旁腺功能减退;术后疗效及术后3个月进行美容效果满意度评分:5分(特别满意)、4分(满意)、3分(一般)、2分(不满意)、1分(特别不满意)。
-
采用t(或t′)检验和χ2检验。
-
腔镜组病人的平均年龄较开放组小(P<0.01)。2组在性别比例、肿块大小、肿瘤位置差异无统计学意义(P>0.05)(见表 1)。
分组 n 男 女 年龄/岁 肿块直径/mm 肿块位置 左 右 腔镜组 35 7 28 36.6±7.6 6.1±2.2 14 21 开放组 45 10 35 44.3±10.9 6.6±2.1 17 28 χ2 — 0.06 3.72* 0.92* 0.04 P — >0.05 < 0.01 >0.05 >0.05 *示t值 表 1 2组一般资料的比较(x±s)
-
2组均成功完成手术,其中腔镜组全部在腔镜下完成,无一例中转开放。腔镜组较开放组手术时间较长、术后第1天引流量多,但术中出血量少、术后第3天VAS评分低(P<0.01)。2组手术在术后住院时间、中央区淋巴结清扫上差异均无统计学意义(P>0.05)(见表 2)。
分组 n 手术时间/min 术中出血量/mL 术后第1天引流量/mL 术后住院时间/d 中央区淋巴结清扫数目 中央区淋巴结清扫阳性数目 术后第3天颈部VAS/分 腔镜组 35 109.0±23.9 24.3±4.2 62.7±9.5 4.3±1.1 3.1±2.5 0.8±1.3 2.5±0.6 开放组 45 64.5±16.4 31.4±5.9 51.4±6.7 4.0±0.7 2.4±2.4 0.7±1.0 3.5±0.7 t — 9.42* 6.02 5.95* 1.40* 1.27 0.52 6.80 P — < 0.01 < 0.01 < 0.01 >0.05 >0.05 >0.05 <0.01 *示t′值 表 2 2组围手术期资料比较(x±s)
-
腔镜组出现3例短暂性喉返神经麻痹,开放组出现5例短暂性喉返神经麻痹,均在术后1个月恢复。腔镜组出现1例、开放组出现2例轻微呛咳,1周后症状消失。2组均未出现淋巴瘘、切口血肿及切口感染,无气管、食管损伤,2组病人术后并发症比较差异无统计学意义(χ2=0.28, P>0.05)。
-
术后所有病人随访3~10个月,复查甲状腺彩超及颈部淋巴结彩超、甲状腺功能、甲状腺球蛋白均在正常范围内,均无肿瘤复发与转移。术后3个月美容效果满意度评分,腔镜组(4.0±0.7)分较开放组的(2.2±0.7)分高,差异有统计学意义(t=11.25, P<0.01)[1]。
-
自1997年HVSCHER等[5]首次报道腔镜甲状腺手术后,腔镜甲状腺手术经过20余年的发展,目前已开展多种手术入路,如经口入路、腋窝入路、全乳晕入路、胸乳入路等。随着科学技术的进步,国内外陆续开展机器人甲状腺手术。经过改良,国内郑传铭2018年报道免充气腋窝入路,取得了良好的手术效果[6-7]。腋窝入路将切口隐藏在腋窝,避免了在颈部留有瘢痕,美容效果佳。本研究中,接受腔镜手术的病人平均年龄明显小于开放手术组,术后美容满意度调查腔镜组明显高于开放组。
随着腔镜器械的改进与临床医生手术技能的提高等,腔镜甲状腺的手术的适应证不断扩大,禁忌证同时也逐渐缩小。但是在腔镜甲状腺手术上,目前国内外对各种甲状腺疾病及入路方式并未给出统一指南以供参考。PTMC是甲状腺癌中主要的病理类型,由于PTMC进展缓慢、恶性程度低、死亡率低,部分学者认为首选随访观察,不建议积极手术[8]。但2016年《甲状腺微小乳头状癌诊断和治疗中国专家共识》中指出[9],对于大多数PTMC仍需手术治疗。PTMC在N0期是否需要行预防性中央区淋巴结清扫,目前尚存争议。2018年,美国国立综合癌症网络指南认为[10],对于低危PTMC可不进行中央区淋巴结清扫;有研究[11]认为清扫后不仅不能显著改善预后,还增加了喉返神经、甲状旁腺损伤的风险。而国内指南建议行患侧中央区淋巴结清扫[12],清扫后不仅减少复发率,提高存活率,更避免了二次手术及产生的并发症。在清扫中央区淋巴结时,腔镜的放大作用增加了识别淋巴结的机会,而从腋窝入路,恰好提供了良好的操作角度,避免了从胸乳入路因为胸骨、锁骨的阻挡而致清扫中央区淋巴结时存在有盲区,造成清扫淋巴结不彻底,从而引起术后复发或转移。笔者经验,术中可用抓钳夹住中央区淋巴脂肪组织,轻微地向头端内上方牵拉,动作要轻柔。本研究组中腔镜组中央区淋巴结清扫的数量与开放组差异无统计学意义,而且术后随访未见复发与转移,说明腔镜组在治疗PTMC与开放组相当。
腔镜手术需要建立并维持一个适当的操作空间,而腔镜甲状腺手术不像胸腔、腹腔有天然的腔隙可供操作,需要人为建立一个腔隙。一般是持续充入CO2建立操作空间,可能会导致皮下气肿、气胸、CO2栓塞等并发症[13]。而我们利用拉钩悬吊皮瓣,随着手术的进行适当调整拉钩,提供良好的操作视野。术中超声刀产生的烟雾被接在拉钩上的吸引器及时吸走,避免镜头模糊影响操作。在游离胸前皮瓣时,我们沿着胸肌浅筋膜浅层游离,在越过锁骨后,从胸锁乳突肌的胸骨头与锁骨头向前游离建立术腔时,因为需要越过颈内静脉与颈总动脉,为了保护血管,我们常规显露颈内静脉,而对于颈总动脉因其在颈内静脉内后方,相对于颈内静脉被误切的可能小,一般不刻意显露。在颈内静脉与肩胛舌骨肌交界处上方,有2~3支小静脉回流至颈内静脉,且存在变异,所以在向上游离时,需小心处理。在游离显露甲状腺时,因为从侧方入路,根据术者经验,可以夹住甲状腺向对侧推,利于游离,不会出现操作盲区。
神经损伤为甲状腺手术常见的并发症[14],一般原因为牵拉、热损伤、钳夹。为了减少并发症的产生,术中操作轻柔,避免牵拉;超声刀功能刀头远离神经至少3 mm,必要时及时0.9%氯化钠溶液降温;术中遵循紧贴被摸操作的原则。对于喉上神经我们不做常规显露,而喉返神经常规显露,并用湿纱布覆盖神经,可降低损伤的发生率。据报道[15]神经检测仪的应用,可更好地保护喉返神经。本研究中,2组神经的损伤差异无统计学意义,此种方式虽然病例中全部为单侧手术,对于甲状旁腺的误切造成手足麻木的可能小。但是甲状旁腺的数量一般为2~6个,很有可能只有一侧有甲状旁腺,所以为了保护甲状旁腺,每一个甲状旁腺都认为其是最后一枚[16]。上位甲状旁腺位置一般较为固定,所以在断上极时采用“脱帽技术”;下位甲状旁腺位置不固定,不易寻找,尤其在清扫中央区淋巴结时,容易被一并切除,所以在清扫中央区淋巴结时,可应用纳米炭[17]来区分甲状旁腺与淋巴结。在切除甲状腺与中央区淋巴脂肪组织后,应仔细寻找切除的组织中是否有甲状旁腺,如果有,将其切碎种植在胸锁乳头肌中。肿瘤种植是手术后严重的并发症,所以腔镜手术中无瘤原则极其重要,故在术中必须保证肿瘤的完整性,用标本袋取出标本,本研究中病人复查未见复发。
本研究中腔镜组的手术时间多于开放组,主要原因是先期开展此手术时手术时间较长,随着手术例数的增加,手术时间明显减少。单侧腋窝入路,在切除一侧甲状腺、峡部、中央区淋巴结时优势明显,但切除对侧甲状腺与中央区淋巴结时极其困难,因此国内外很少报道双侧腋窝入路, 此术式虽然能顺利完成手术要求,但是明显增加了手术时间与创伤。一般双侧甲状腺病变会选择胸乳入路[18],但需要游离较多皮瓣。为此,我们开始尝试从锁骨下入路处理双侧病变,取得了良好的手术效果。
综上所述,在把握好手术适应证、禁忌证的基础上,免充气经腋窝入路在治疗N0期的PTMC是完全可行、有效、安全的,而且具有较佳的美容效果,值得推广。
免充气经腋窝入路腔镜下甲状腺微小乳头状癌手术疗效评价
Effect evaluation of endoscopic surgery for papillary thyroid microcarcinoma through axillary approach without inflation
-
摘要:
目的探讨免充气经腋窝入路治疗甲状腺微小乳头状癌的手术经验及疗效。 方法选取80例甲状腺微小乳头状癌病人,其中行腔镜手术35例(腔镜组),开放手术45例(开放组),比较2组病人围手术期资料、并发症及随访情况等资料。 结果腔镜组平均年龄较开放组年轻(P<0.05);腔镜组平均手术时间及术后第1天引流液量均较开放组多(P<0.01);腔镜组术中出血量比开放组少(P<0.01);术后第3天颈部VAS评分腔镜组较开放组低(P<0.05);中央区清扫后平均淋巴结数目腔镜组与开放组比较差异无统计学意义(P>0.05);2组病人术后住院时间、术后并发症比较差异无统计学意义(P>0.05);腔镜组术后美容满意度较高(P<0.01);随访3个月以上,均未见复发与转移。 结论免充气经腋窝入路腔镜下甲状腺微小乳头状癌手术安全可行,与开放手术相当,并具有较佳的美容效果。 Abstract:ObjectiveTo explore the surgical experience and curative effects of the axillary approach without inflation in the treatment of papillary thyroid microcarcinoma. MethodsA total of 80 patients with papillary thyroid microcarcinoma were divided into the endoscope group(35 cases treated with endoscopic surgery) and open group(45 cases treated with open surgery).The perioperative data, complications and following-up data were compared between two groups. ResultsThe average age in endoscope group was younger than that in open group(P<0.05), the average operation time and amount of drainage fluid on the first day after the operation in endoscope group were more than those in open group(P<0.01), and the intraoperative blood loss in endoscope group was less than that in open group(P<0.01).The neck VAS score in endoscope group was lower than that in open group on the third day after operation(P<0.05).The difference of the average number of lymph nodes after central dissection between two groups was not statistically significant(P>0.05).There was no statistical significance in the postoperative hospital stay and postoperative complications between two groups(P>0.05).The postoperative cosmetic satisfaction in endoscope group was higher than that in open group(P<0.01).All cases were followed up for more than 3 months, and no recurrence or metastasis case was found. ConclusionsThe axillary approach without inflation in the treatment of papillary thyroid microcarcinoma is safe and feasible, has better cosmetic effects, and which is comparable to open surgery. -
表 1 2组一般资料的比较(x±s)
分组 n 男 女 年龄/岁 肿块直径/mm 肿块位置 左 右 腔镜组 35 7 28 36.6±7.6 6.1±2.2 14 21 开放组 45 10 35 44.3±10.9 6.6±2.1 17 28 χ2 — 0.06 3.72* 0.92* 0.04 P — >0.05 < 0.01 >0.05 >0.05 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 2组围手术期资料比较(x±s)
分组 n 手术时间/min 术中出血量/mL 术后第1天引流量/mL 术后住院时间/d 中央区淋巴结清扫数目 中央区淋巴结清扫阳性数目 术后第3天颈部VAS/分 腔镜组 35 109.0±23.9 24.3±4.2 62.7±9.5 4.3±1.1 3.1±2.5 0.8±1.3 2.5±0.6 开放组 45 64.5±16.4 31.4±5.9 51.4±6.7 4.0±0.7 2.4±2.4 0.7±1.0 3.5±0.7 t — 9.42* 6.02 5.95* 1.40* 1.27 0.52 6.80 P — < 0.01 < 0.01 < 0.01 >0.05 >0.05 >0.05 <0.01 *示t′值
下载: 导出CSV
-
[1] KITAHARA CM, SOSA JA. The changing incidence of thyroid cancer[J]. Nat Rev Endocrinol, 2016, 12(11): 646. doi: 10.1038/nrendo.2016.110 [2] ITO Y, MIYAUCHI A, ODA H, et al. Low-risk papillary microcarcinoma of the thyroid: A review of active surveillance trials[J]. Eur J Surg Oncol, 2018, 44(3): 307. doi: 10.1016/j.ejso.2017.03.004 [3] TAN Y, GUO B, DENG X, et al. Transoral endoscopic selective lateral neck dissection for papillary thyroid carcinoma: a pilot study[J]. Surg Endosc, 2020, 34(12): 5274. doi: 10.1007/s00464-019-07314-8 [4] GUO Y, QU R, HUO J, et al. Technique for endoscopic thyroidectomy with selective lateral neck dissection via a chest breast approach[J]. Surg Endosc, 2019, 33(4): 1334. doi: 10.1007/s00464-018-06608-7 [5] HÜSCHER CS, CHIODINI S, NAPOLITANO C, et al. Endoscopic right thyroid lobectomy[J]. Surg Endosc, 1997, 11(8): 877. doi: 10.1007/s004649900476 [6] 郑传铭, 毛晓春, 王佳峰. 无充气腋窝入路完全腔镜下甲状腺癌根治术效果初步评价初期体会[J]. 中国肿瘤临床, 2018, 45(1): 27. doi: 10.3969/j.issn.1000-8179.2018.01.801 [7] 郑传铭, 徐加杰, 蒋烈浩, 等. 无充气腋窝入路完全腔镜下叶切除的方法-葛-郑氏七步法[J]. 中国普通外科杂志, 2019, 28(11): 1336. doi: 10.7659/j.issn.1005-6947.2019.11.003 [8] MIYAUCHI A, ITO Y, ODA H, et al. Insights into the Management of Papillary Microcarcinoma of the Thyroid[J]. Thyroid, 2018, 28(1): 23. doi: 10.1089/thy.2017.0227 [9] 高明, 葛明华, 嵇庆海, 等. 甲状腺微小乳头状癌诊断与治疗中国专家共识(2016版)[J]. 中国肿瘤临床, 2016, 43(10): 405. doi: 10.3969/j.issn.1000-8179.2016.10.001 [10] HADDAD RI, NASR C, BISCHOFF L, et al. NCCN Guidelines Insights: Thyroid Carcinoma, Version 2.2018[J]. J Natl Compr Canc Netw, 2018, 16(12): 1429. doi: 10.6004/jnccn.2018.0089 [11] MILANO AF. Thyroid Cancer: 20-Year Comparative Mortality and Survival Analysis of Six Thyroid Cancer Histologic Subtypes by Age, Sex, Race, Stage, Cohort Entry Time-Period and Disease Duration(SEER*Stat 8.3.2) A Systematic Review of 145, 457 Cases for Diagnosis Years 1993-2013[J]. J Insur Med, 2018, 47(3): 143. doi: 10.17849/insm-47-03-143-158.1 [12] 甲状腺癌诊疗规范(2018年版)[J/CD]. 中华普通外科学文献: 电子版, 2019, 13(1): 1. [13] FU J, LUO Y, CHEN Q, et al. Transoral Endoscopic Thyroidectomy: Review of 81 Cases in a Single Institute[J]. J Laparoendosc Adv Surg Tech A, 2018, 28(3): 286. doi: 10.1089/lap.2017.0435 [14] LI Y, ZHOU X. Comparison between endoscopic thyroidectomy and conventional open thyroidectomy for papillary thyroid microcarcinoma: A meta-analysis[J]. Cancer Res Ther, 2016, 12(2): 550. doi: 10.4103/0973-1482.157353 [15] DIONIGI G, KIM HY, WU CW, et al. Neuromonitoring in endoscopic and robotic thyroidectomy[J]. Updates Surg, 2017, 69(2): 171. doi: 10.1007/s13304-017-0442-z [16] PEISSIG K, CONDIE BG, MANLEY NR. Embryology of the Parathyroid Glands[J]. Endocrinol Metab Clin North Am, 2018, 47(4): 733. doi: 10.1016/j.ecl.2018.07.002 [17] TIAN W, XI HQ, WANG B. Pay attention to the standardized application of new techniques in surgical treatment of thyroid disease[J]. Zhonghua Wai Ke Za Zhi, 2017, 55(8): 561. [18] 邓锐, 周少波, 贲大刚, 等. 经胸乳入路腔镜甲状腺手术在甲状腺良性肿瘤中的应用[J]. 蚌埠医学院学报, 2020, 45(5): 606. -

 点击查看大图
点击查看大图

图(5)表(2)
计量
- 文章访问数: 3761
- HTML全文浏览量: 2129
- PDF下载量: 11
- 被引次数: 0
