

-
妊娠期高血压为妊娠期常见并发症之一,多于妊娠20周后发生,我国妊娠期高血压发病率为5%~9%,国外报道为7%~12%,是导致孕产妇及围产儿死亡的重要原因,积极进行防治,对改善母婴健康具有重要意义[1-2]。目前临床关于妊娠期高血压尚无特效治疗药物,仍以预防为重点[3]。临床研究[4-5]显示,随着人们生活水平的提高,孕龄期女性超重、肥胖问题日益突出,超重、肥胖问题不仅增加妊娠期及围产期并发症发生风险,还会影响胎儿的正常生长发育。国内相关报道[6]指出,妊娠期脂质代谢发生变化导致孕妇血脂水平处于异常表达状态,可能参与妊娠期高血压的发病。此外,妊娠期高血压最基本的病理生理改变是全身小动脉的痉挛,严重时可引发心、肝、肾等重要脏器的损害,从而影响母婴健康[7-8]。基于此,本研究探讨孕期体质量增值、血脂水平与孕妇妊娠期高血压靶器官损害及妊娠结局的关系,旨在为该病的防治提供参考。现作报道。
-
选取2018年5月至2020年3月我院收治的85例妊娠期高血压孕妇作为研究组,年龄21~34岁,孕周30~40周,经产情况:初产58例,非初产27例。随机选取同期60名正常孕妇作为对照组,年龄20~34岁,孕周30~41周;经产情况:初产38例,非初产22例。
-
纳入标准:(1)研究组,①符合妊娠期高血压诊断标准[9];②年龄≤34岁;③单胎妊娠;④自然受孕;⑤无子宫肌瘤、多囊卵巢综合征、输卵管阻塞等疾病;⑥自主行为能力良好,能配合完成研究;⑦于我院进行分娩;⑧病人知晓本研究,已签署同意书。(2)对照组,①健康、正常妊娠孕妇;②年龄≤34岁;③于我院进行分娩;孕妇及家属知晓本研究,已签署同意书。排除标准:(1)传染性疾病病人;(2)心脑肝肾等重要脏器功能不全者;(3)妊娠前明确诊断为高血压、高血脂者;(4)感染性疾病病人;(5)妊娠期糖尿病病人。
-
实验室指标检测方法:入组当天,采集所有研究对象外周静脉血3 mL,于2 h内以3 500 r/min转速离心处理5 min,取上层清液,置于-20 ℃冷藏室内保存,采用沈阳万泰医疗设备有限责任公司生产的OTA-400型全自动生化分析仪及其配套试剂盒检测血脂水平,包括三酰甘油(TG)、总胆固醇(TC)、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C),检测操作均由专业人员严格按照仪器操作说明及试剂盒说明书完成。治疗方法:2组入院后均施行饮食干预、利尿扩容、降低钠盐及体液摄入、卧床休息等综合干预,必要时可遵医嘱给予适量硫酸镁、盐酸拉贝洛尔等药物治疗。
-
2组一般资料,包括年龄、孕周、经产情况、高血压病家族史、孕前检查、户籍地、吸烟史、饮酒史、孕前体质量指数(BMI)、孕期体质量增值、高血压病家族史及TG、TC、HDL-C、LDL-C水平,孕期体质量增值=孕晚期体质量-孕前体质量;饮酒定义:每日饮白酒≥110 mL或啤酒≥2瓶,每周饮酒≥1次;吸烟定义:每天抽烟≥1支,连续吸烟时间>6个月。研究组不同靶器官损害情况病人的孕期体质量增值、血脂水平,靶器官损害情况包括无靶器官损害、1个靶器官损害、≥2个靶器官损害[10]。
-
采用χ2检验、方差分析、q检验、t检验、Spearman相关分析、logistic多因素回归分析、受试者工作特征(ROC)曲线和DeLong检验。
-
研究组年龄、孕周、经产情况、孕前检查、户籍地、吸烟史、饮酒史与对照组差异均无统计学意义(P>0.05);研究组孕前BMI、孕期体质量增值、高血压病家族史及TG、TC、LDL-C水平均较对照组高(P<0.01),HDL-C水平较对照组低(P<0.01)(见表 1)。
项目 研究组(n=85) 对照组(n=60) t P 年龄/岁 27.45±2.69 26.82±2.41 1.45 >0.05 孕周/周 35.26±2.17 35.81±2.43 1.43 >0.05 经产情况(初产/非初产) 58/27 38/22 0.38* >0.05 孕前BMI/(kg/m2) 23.48±2.16 21.26±1.84 6.47 < 0.01 孕期体质量增值/kg 17.24±3.88 13.86±3.75 5.24 < 0.01 高血压病家族史(有/无) 33/52 11/49 6.99* < 0.01 孕前检查(有/无) 53/32 38/22 0.02* >0.05 TG/(mmol/L) 5.30±1.22 3.12±0.85 11.94 < 0.01 TC/(mmol/L) 6.71±1.43 5.38±0.92 6.34* < 0.01 HDL-C/(mmol/L) 1.75±0.38 1.97±0.43 3.25 < 0.01 LDL-C/(mmol/L) 3.51±0.79 3.08±0.66 3.45 < 0.01 户籍地(城镇/农村) 41/44 32/28 0.37* >0.05 吸烟史(有/无) 15/70 8/52 0.49* >0.05 饮酒史(有/无) 18/67 9/51 0.89* >0.05 *示χ2值 表 1 一般资料比较(x±s)
-
以是否发生妊娠期高血压作为因变量(未发生为0,发生赋值为1),将单因素分析结果中差异有统计学意义的孕前BMI、孕期体质量增值、高血压病家族史及TG、TC、HDL-C、LDL-C水平作为自变量,纳入logistic回归分析模型,结果显示,孕前BMI、孕期体质量增值、高血压病家族史及TG、TC、HDL-C、LDL-C水平均为妊娠期高血压发生的影响因素(P<0.05~P<0.01)(见表 2)。
变量 B SE Waldχ2 P OR 95%CI 孕前BMI 1.026 0.521 3.875 < 0.01 2.789 1.243~6.257 孕期体质量增值 0.880 0.375 5.513 < 0.01 2.412 1.359~4.281 高血压病家族史 1.300 0.620 4.394 < 0.01 3.668 1.866~7.209 TG 0.593 0.226 6.881 < 0.01 1.809 1.105~2.962 TC 0.566 0.257 4.845 < 0.01 1.761 1.450~2.138 HDL-C -0.648 0.359 3.526 < 0.05 0.523 0.315~0.869 LDL-C 0.652 0.342 3.629 < 0.05 1.918 1.307~2.816 表 2 妊娠期高血压发生的影响因素分析
-
研究组随着靶器官损害数目的增加,病人的孕期体质量增值、TG、TC、与LDL-C水平增高(P<0.05~P<0.01),HDL-C水平降低(P<0.01)(见表 3)。
靶器官损害情况 n 孕期体质量增值/kg TG/(mmol/L) TC/(mmol/L) HDL-C/(mmol/L) LDL-C/(mmol/L) 无靶器官损害 21 15.81±2.10 4.39±0.95 5.87±0.97 1.85±0.39 3.12±0.61 1个靶器官损害 40 17.80±2.76** 5.48±1.19** 6.62±1.05* 1.37±0.34** 3.83±0.68** ≥2个靶器官损害 24 20.37±3.11**△△ 8.38±1.04**△△ 8.81±1.32**△△ 0.99±0.22**△△ 4.86±0.73**△△ F — 15.99 84.01 44.66 39.25 37.94 P — < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 MS组内 — 7.412 1.197 1.243 0.106 0.460 q检验:与无靶器官损害组比较*P<0.05,**P<0.01;与1个靶器官损害组比较△△P<0.01 表 3 研究组不同靶器官损害情况病人的孕期体质量增值、血脂水平(x±s)
-
孕期体质量增值、TG、TC、LDL-C水平与靶器官损害间呈正相关关系(P<0.01),HDL-C水平与靶器官损害间呈负相关关系(P<0.01)(见表 4)。
指标 孕期体质量增值 TG TC HDL-C LDL-C 靶器官损害情况 r 0.346 0.571 0.526 -0.491 0.452 P < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 表 4 妊娠期高血压孕期体质量增值、血脂水平与靶器官损害的关联性分析
-
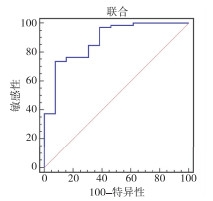
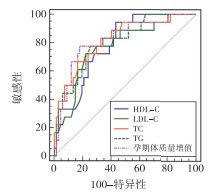
孕期体质量增值、TG、TC、HDL-C、LDL-C水平联合评估靶器官损害的AUC为0.879,大于各指标单一评估,最佳评估敏感度、特异度分别为73.82%、92.40%(P<0.01)(见图 1~2、表 5)。

图 1 孕期体质量增值、血脂水平单一评估ROC

图 2 孕期体质量增值、血脂水平联合评估ROC
指标 AUC 95%CI Z P 截断值 截断值敏感度/% 截断值特异度/% 孕期体质量增值 0.789 0.679~0.899 5.129 <0.01 >17.21 kg 69.44 92.31 TG 0.819 0.681~0.958 4.529 <0.01 >5.67 mmol/L 73.61 84.62 TC 0.810 0.710~0.910 6.074 <0.01 >6.80 mmol/L 66.67 92.28 HDL-C 0.754 0.595~0.913 3.132 <0.01 ≤1.57 mmol/L 83.33 61.54 LDL-C 0.782 0.665~0.900 4.704 <0.01 >3.69 mmol/L 69.38 84.59 联合预测 0.879 0.773~0.985 7.001 <0.01 — 73.82 92.40 表 5 孕期体质量增值、血脂水平评估靶器官损害情况的效能分析
-
随访至妊娠结束,统计研究组妊娠结局,其中产后出血2例,胎儿宫内窘迫4例,早产儿6例,胎膜早破2例,羊水过少4例,纳入妊娠结局不良,共18例。妊娠结局不良病人的孕期体质量增值、TG、TC、LDL-C水平均较妊娠结局良好病人高(P<0.01),HDL-C水平较妊娠结局良好病人低(P<0.01)(见表 6)。
妊娠结局 n 孕期体质量增值/kg TG/(mmol/L) TC/(mmol/L) HDL-C/ (mmol/L) LDL-C/ (mmol/L) 妊娠结局良好 67 16.12±3.59 5.13±1.31 6.60±1.13 1.85±0.52 3.37±0.75 妊娠结局不良 18 19.13±3.92 8.61±1.45 9.12±1.46 1.04±0.35 4.32±0.83 t — 3.10 9.78 7.88 6.23 4.66 P — <0.01 <0.01 <0.01 <0.01 <0.01 表 6 研究组妊娠结局良好与妊娠结局不良病人的孕期体质量增值、血脂水平(x±s)
-
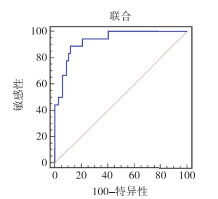
孕期体质量增值、TG、TC、HDL-C、LDL-C水平联合预测妊娠结局不良的AUC为0.932,大于各指标单一预测,最佳预测敏感度、特异度分别为88.89%、88.06%(P<0.01)(见图 3~4、表 7)。
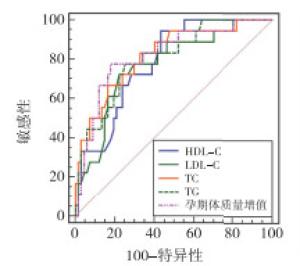
图 3 孕期体质量增值、血脂水平单一预测ROC
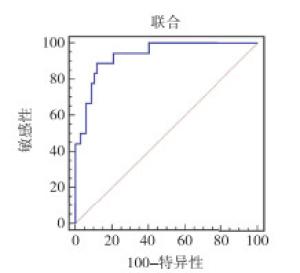
图 4 孕期体质量增值、血脂水平联合预测ROC
指标 AUC 95%CI Z P 截断值 截断值敏感度/% 截断值特异度/% 孕期体质量增值 0.822 0.710~0.933 5.652 <0.01 >18.04 kg 77.78 82.09 TG 0.804 0.694~0.915 5.413 <0.01 >6.94 mmol/L 77.78 74.63 TC 0.819 0.707~0.931 5.595 <0.01 >7.42 mmol/L 83.33 67.16 HDL-C 0.786 0.682~0.889 5.413 <0.01 ≤1.64 mmol/L 94.44 56.72 LDL-C 0.773 0.651~0.895 4.384 <0.01 >3.99 mmol/L 72.22 77.61 联合预测 0.932 0.875~0.989 14.817 <0.01 — 88.89 88.06 表 7 孕期体质量增值、血脂水平预测妊娠结局不良的效能分析
-
妊娠期高血压临床表现为高血压、蛋白尿、浮肿,严重时出现抽搐、昏迷,甚至母婴死亡,是全球范围内重点关注的公共健康问题之一[11-12]。早发现、早诊断、早治疗,对保障妊娠期高血压孕妇及胎儿生命安全至关重要。
肥胖是妊娠期高血压发病的基础之一[13],本研究发现,妊娠期高血压病人的孕前BMI、孕期体质量增值明显高于正常孕妇,且均为妊娠期高血压发生的影响因素,提示孕前BMI、孕期体质量增值过大可增加妊娠期高血压发生风险。石晛等[14]通过对366例妊娠期高血压疾病的一项研究显示,BMI与妊娠期高血压疾病的发生密切相关。符剑花等[15]报道显示,孕早期增重过多可增加妊娠期高血压发生风险。均支持本研究结果结论。BMI是反映机体内脂肪含量的重要指标,其值变化可反映机体肥胖程度[16-17]。孕前BMI高提示孕妇孕前脂肪含量较多,孕期体质量增值大提示孕妇妊娠期体质量增长超过正常水平,也是体内脂肪含量增加的主要表现,体内脂肪含量增加,可导致血液循环中血脂含量升高,孕妇体内易出现血脂代谢紊乱、脂质过氧化反应增强及前列环素生成减少,导致血管内皮损伤和血液浓缩,引起血流动力学改变及外周循环阻力增加,从而增加妊娠期高血压发生风险[18-19]。郭欣等[20]研究显示,血脂代谢与妊娠期高血压内皮损伤有关,病人TG、TC、LDL-C水平明显升高,HDL-C水平明显降低。本研究也发现妊娠期高血压病人TG、TC、LDL-C水平明显高于正常孕妇,HDL-C水平低于正常孕妇,且是妊娠期高血压发生的影响因素。进一步证实血脂水平异常参与妊娠期高血压的发生发展。血脂代谢异常引起氧化应激,并引发血管内皮损伤,促进妊娠期高血压发生[21-22]。本研究还发现,高血压病家族史也是妊娠期高血压发生的影响因素,与国内外相关研究结果相符。对于存在上述危险因素的孕妇,应加强相关干预,积极预防妊娠期高血压。
此外,高血压是引起心脑血管疾病的高危因素,长期的高血压可引起多器官、组织功能损害[23-24]。本研究发现,不同靶器官损害数量妊娠期高血压病人的孕期体质量增值、TG、TC、HDL-C、LDL-C水平存在明显差异,我们首次通过相关性分析探讨孕期体质量增值、血脂水平与妊娠期高血压靶器官损害的关联性,发现孕期体质量增值、TG、TC、LDL-C水平与靶器官损害呈正相关,HDL-C水平与靶器官损害呈负相关。提示孕期体质量增值、TG、TC、LDL-C水平升高、HDL-C水平降低越明显,靶器官损害就越多。因此,妊娠期高血压发生后应积极开展控制体质量、降脂等干预或治疗,尽量降低靶器官损害,保障母婴健康。我们通过ROC曲线分析发现,孕期体质量增值、血脂水平在评估靶器官损害方面具有良好效能,可辅助临床判断妊娠期高血压靶器官损害情况,有助于指导相关治疗的开展。国内外多项研究[25-27]显示,妊娠期高血压可造成子宫和胎盘内供血量减少,引起胎盘功能降低,致使胎儿摄入母体内营养物质和氧气量减少,胎盘内酶活性降低,最终影响胎儿生长发育,增加不良妊娠结局发生风险。我们通过随访研究发现,妊娠结局不良妊娠期高血压病人的孕期体质量增值、血脂水平与妊娠结局良好病人存在明显差异,提示孕期体质量增值、血脂水平在判断妊娠期高血压妊娠结局方面具有一定潜力。进一步通过ROC曲线分析发现,孕期体质量增值、TG、TC、HDL-C、LDL-C水平预测妊娠期高血压不良妊娠结局的AUC均在0.75以上,具有良好应用价值,尤其是各指标联合预测的AUC高达0.932,可为临床判断妊娠期高血压妊娠结局提供更准确信息,从而指导相关干预、治疗措施的制定和开展。
综上所述,孕妇妊娠期高血压的发病、靶器官损害与孕期体质量增值、血脂水平关联性显著,明确孕期体质量增值、血脂水平变化情况可辅助临床预测不良妊娠结局发生风险,具有较高临床应用价值。本研究创新之处在于明确了孕期体质量增值、血脂水平与孕妇妊娠期高血压发病、靶器官损害及妊娠结局的关系,可为临床预防、治疗妊娠期高血压提供参考。但本研究为单中心研究,存在一定局限性,可能出现不可避免的选择偏倚及结果偏差等,有待日后通过多中心研究进一步研究结果的正确性。
孕期体质量增值、血脂水平与孕妇妊娠期高血压靶器官损害及妊娠结局的关联性分析
Correlation analysis of the body mass gain and blood lipid level during pregnancy with target organ damage of pregnancy hypertension and pregnancy outcome
-
摘要:
目的探讨孕期体质量增值、血脂水平与孕妇妊娠期高血压靶器官损害及妊娠结局的关联性。 方法选取85例妊娠期高血压孕妇作为研究组,随机选取同期60名正常孕妇作为对照组。统计比较2组一般资料,探讨妊娠期高血压发病的危险因素,比较研究组不同靶器官损害情况病人的孕期体质量增值、血脂水平,并分析孕期体质量增值、血脂水平与靶器官损害的关联性,随访至妊娠结束,统计研究组妊娠结局,比较妊娠结局良好与妊娠结局不良病人的孕期体质量增值、血脂水平,探究孕期体质量增值、血脂水平评估靶器官损害情况及预测妊娠结局不良的效能。 结果研究组孕前体质量指数(BMI)、孕期体质量增值、高血压病家族史及三酰甘油(TG)、总胆固醇(TC)、低密度脂蛋白胆固醇(LDL-C)水平均高于对照组(P<0.01),高密度脂蛋白胆固醇(HDL-C)水平低于对照组(P<0.05);妊娠期高血压发生的影响因素包括孕前BMI、孕期体质量增值、高血压病家族史及TG、TC、HDL-C、LDL-C水平(P<0.05~P<0.01);孕期体质量增值、TG、TC、LDL-C水平与靶器官损害呈正相关关系(P<0.01),HDL-C水平与靶器官损害呈负相关关系(P<0.05);孕期体质量增值、TG、TC、HDL-C、LDL-C水平联合评估靶器官损害情况的曲线下面积(AUC)为0.879,大于各指标单一评估,最佳评估敏感度、特异度分别为73.82%、92.40%;妊娠结局不良病人的孕期体质量增值、TG、TC、LDL-C水平高于妊娠结局良好病人,HDL-C水平低于妊娠结局良好患者病人(P<0.05);孕期体质量增值、TG、TC、HDL-C、LDL-C水平联合预测妊娠结局不良的AUC为0.932,大于各指标单一预测,最佳预测敏感度、特异度分别为88.89%、88.06%。 结论孕期体质量增值、血脂水平与孕妇妊娠期高血压发病及靶器官损害密切相关,且能辅助临床评估靶器官损害情况、预测不良妊娠结局发生风险。 Abstract:ObjectiveTo explore the correlation of the body mass gain and blood lipid level during pregnancy with target organ damage of pregnancy hypertension and pregnancy outcome. MethodsA total of 85 pregnant women with hypertension during pregnancy were set as the study group, and 60 normal pregnant women during the same period were randomly selected as the control group.The general data of two groups were statistically compared, and the risk factors of hypertension during pregnancy were investigated.The body mass gain and blood lipid level during pregnancy of patients with different target organ damage in study group were compared, and the correlation between the body mass gain, blood lipid level during pregnancy and target organ damage were analyzed.The study group was followed up to the end of pregnancy, and the pregnancy outcome of the study group was counted.The baody mass gain and blood lipid level during pregnancy were compared between patients with good and poor pregnancy outcomes and the efficacy of body mass gain and blood lipid level during pregnancy in assessing target organ damage and predicting poor pregnancy outcome were explored. ResultsBefore pregnancy, the body mass index(BMI), body mass gain during pregnancy, family history of hypertension, and levels of triglyceride(TG), total cholesterol(TC) and low-density lipoprotein cholesterol(LDL-C) in study group were higher than those in control group(P<0.01), and the high-density lipoprotein cholesterol(HDL-C) level in study group was lower than that in control group(P<0.05).The BMI before pregnancy, body mass gain during pregnancy, family history of hypertension, and levels of TG, TC, HDL-C and LDL-C were the influencing factors of hypertension during pregnancy(P<0.05 to P<0.01).The body mass gain during pregnancy, and levels of TG, TC and LDL-C were positively correlated with the target organ damage(P<0.01), and the HDL-C level was negatively correlated with target organ damage(P<0.05).The area under the curve (AUC) of body mass gain during pregnancy, and levels of TG, TC, HDL-C and LDL-C in the combined assessment of target organ damage was 0.879, which was greater than a single assessment of each index, and the best evaluation sensitivity and specificity were 73.82% and 92.40%, respectively.The body mass gain during pregnancy, and levels of TG, TC and LDL-C in patients with poor pregnancy outcome were higher than those in patients with good pregnancy outcome(P<0.05), and the HDL-C level in patients with poor pregnancy outcome was lower than that in patients with good pregnancy outcome(P<0.05).The AUC of body mass gain during pregnancy, and levels of TG, TC, HDL-C and LDL-C in the combined assessment of poor pregnancy outcome was 0.932, which was greater than a single assessment of each index, and the best evaluation sensitivity and specificity were 88.89% and 88.06%, respectively. ConclusionsThe body mass gain and blood lipid level during pregnancy are closely related to the onset of pregnancy-induced hypertension and target organ damage, and can assist the clinical assessment of target organ damage and predict the risk of adverse pregnancy outcome. -
表 1 一般资料比较(x±s)
项目 研究组(n=85) 对照组(n=60) t P 年龄/岁 27.45±2.69 26.82±2.41 1.45 >0.05 孕周/周 35.26±2.17 35.81±2.43 1.43 >0.05 经产情况(初产/非初产) 58/27 38/22 0.38* >0.05 孕前BMI/(kg/m2) 23.48±2.16 21.26±1.84 6.47 < 0.01 孕期体质量增值/kg 17.24±3.88 13.86±3.75 5.24 < 0.01 高血压病家族史(有/无) 33/52 11/49 6.99* < 0.01 孕前检查(有/无) 53/32 38/22 0.02* >0.05 TG/(mmol/L) 5.30±1.22 3.12±0.85 11.94 < 0.01 TC/(mmol/L) 6.71±1.43 5.38±0.92 6.34* < 0.01 HDL-C/(mmol/L) 1.75±0.38 1.97±0.43 3.25 < 0.01 LDL-C/(mmol/L) 3.51±0.79 3.08±0.66 3.45 < 0.01 户籍地(城镇/农村) 41/44 32/28 0.37* >0.05 吸烟史(有/无) 15/70 8/52 0.49* >0.05 饮酒史(有/无) 18/67 9/51 0.89* >0.05 *示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 妊娠期高血压发生的影响因素分析
变量 B SE Waldχ2 P OR 95%CI 孕前BMI 1.026 0.521 3.875 < 0.01 2.789 1.243~6.257 孕期体质量增值 0.880 0.375 5.513 < 0.01 2.412 1.359~4.281 高血压病家族史 1.300 0.620 4.394 < 0.01 3.668 1.866~7.209 TG 0.593 0.226 6.881 < 0.01 1.809 1.105~2.962 TC 0.566 0.257 4.845 < 0.01 1.761 1.450~2.138 HDL-C -0.648 0.359 3.526 < 0.05 0.523 0.315~0.869 LDL-C 0.652 0.342 3.629 < 0.05 1.918 1.307~2.816
下载: 导出CSV
表 3 研究组不同靶器官损害情况病人的孕期体质量增值、血脂水平(x±s)
靶器官损害情况 n 孕期体质量增值/kg TG/(mmol/L) TC/(mmol/L) HDL-C/(mmol/L) LDL-C/(mmol/L) 无靶器官损害 21 15.81±2.10 4.39±0.95 5.87±0.97 1.85±0.39 3.12±0.61 1个靶器官损害 40 17.80±2.76** 5.48±1.19** 6.62±1.05* 1.37±0.34** 3.83±0.68** ≥2个靶器官损害 24 20.37±3.11**△△ 8.38±1.04**△△ 8.81±1.32**△△ 0.99±0.22**△△ 4.86±0.73**△△ F — 15.99 84.01 44.66 39.25 37.94 P — < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 MS组内 — 7.412 1.197 1.243 0.106 0.460 q检验:与无靶器官损害组比较*P<0.05,**P<0.01;与1个靶器官损害组比较△△P<0.01
下载: 导出CSV
表 4 妊娠期高血压孕期体质量增值、血脂水平与靶器官损害的关联性分析
指标 孕期体质量增值 TG TC HDL-C LDL-C 靶器官损害情况 r 0.346 0.571 0.526 -0.491 0.452 P < 0.01 < 0.01 < 0.01 < 0.01 < 0.01
下载: 导出CSV
表 5 孕期体质量增值、血脂水平评估靶器官损害情况的效能分析
指标 AUC 95%CI Z P 截断值 截断值敏感度/% 截断值特异度/% 孕期体质量增值 0.789 0.679~0.899 5.129 <0.01 >17.21 kg 69.44 92.31 TG 0.819 0.681~0.958 4.529 <0.01 >5.67 mmol/L 73.61 84.62 TC 0.810 0.710~0.910 6.074 <0.01 >6.80 mmol/L 66.67 92.28 HDL-C 0.754 0.595~0.913 3.132 <0.01 ≤1.57 mmol/L 83.33 61.54 LDL-C 0.782 0.665~0.900 4.704 <0.01 >3.69 mmol/L 69.38 84.59 联合预测 0.879 0.773~0.985 7.001 <0.01 — 73.82 92.40
下载: 导出CSV
表 6 研究组妊娠结局良好与妊娠结局不良病人的孕期体质量增值、血脂水平(x±s)
妊娠结局 n 孕期体质量增值/kg TG/(mmol/L) TC/(mmol/L) HDL-C/ (mmol/L) LDL-C/ (mmol/L) 妊娠结局良好 67 16.12±3.59 5.13±1.31 6.60±1.13 1.85±0.52 3.37±0.75 妊娠结局不良 18 19.13±3.92 8.61±1.45 9.12±1.46 1.04±0.35 4.32±0.83 t — 3.10 9.78 7.88 6.23 4.66 P — <0.01 <0.01 <0.01 <0.01 <0.01
下载: 导出CSV
表 7 孕期体质量增值、血脂水平预测妊娠结局不良的效能分析
指标 AUC 95%CI Z P 截断值 截断值敏感度/% 截断值特异度/% 孕期体质量增值 0.822 0.710~0.933 5.652 <0.01 >18.04 kg 77.78 82.09 TG 0.804 0.694~0.915 5.413 <0.01 >6.94 mmol/L 77.78 74.63 TC 0.819 0.707~0.931 5.595 <0.01 >7.42 mmol/L 83.33 67.16 HDL-C 0.786 0.682~0.889 5.413 <0.01 ≤1.64 mmol/L 94.44 56.72 LDL-C 0.773 0.651~0.895 4.384 <0.01 >3.99 mmol/L 72.22 77.61 联合预测 0.932 0.875~0.989 14.817 <0.01 — 88.89 88.06
下载: 导出CSV
-
[1] 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2020)[J]. 中华妇产科杂志, 2020, 55(4): 277. [2] Canadian Hypertension Education Program, Society of Obstetricians and Gynaecologists of Canada. Hypertension Canada's 2018 Guidelines for the Management of Hypertension in Pregnancy[J]. Can J Cardiol, 2018, 34(5): 526. doi: 10.1016/j.cjca.2018.02.021 [3] 邓琼, 江丹丹, 莫萍, 等. 小剂量阿司匹林预防妊娠期高血压疾病的效果分析[J]. 中国实用医药, 2020, 15(19): 135. [4] FERNÁNDEZ ALBA JJ, MESA PÁEZ C, VILAR SÁNCHEZ Á, et al. Overweight and obesity at risk factors for hypertensive states of pregnancy: a retrospective cohort study[J]. Nutr Hosp, 2018, 35(4): 874. doi: 10.20960/nh.1702 [5] SANTOS S, VOERMAN E, AMIANO P, et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: an individual participant data meta-analysis of European, North American and Australian cohorts[J]. BJOG, 2019, 126(8): 984. [6] 郑君, 彭菊生, 饶敏. 孕期血清脂溶性维生素及血脂水平与妊娠期高血压疾病关系[J]. 中国计划生育学杂志, 2019, 27(8): 994. [7] 李艳红, 乔江丽. 硝苯地平联合拉贝洛尔对妊娠期高血压疾病病人心肾功能及血流动力学的影响[J]. 内蒙古医科大学学报, 2019, 41(3): 243. [8] 尹雪, 张华, 刘振东, 等. 妊娠期高血压疾病危险因素及其在靶器官损害中的作用[J]. 河北医学, 2018, 24(7): 1178. doi: 10.3969/j.issn.1006-6233.2018.07.030 [9] BROWN MA, MAGEE LA, KENNY LC, et al. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice[J]. Hypertens, 2018, 72(1): 24. doi: 10.1161/HYPERTENSIONAHA.117.10803 [10] 张姗姗. 妊娠期高血压疾病患者血清硫化氢水平及其与靶器官损害的相关性[J]. 中国妇幼保健, 2017, 32(3): 449. [11] 吴琳琳, 周欣, 牛建民. 《妊娠期高血压疾病: 国际妊娠期高血压研究学会分类、诊断和管理指南(2018)》解读[J]. 中国实用妇科与产科杂志, 2018, 34(7): 758. [12] American College of Obstetricians and Gynecologists. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222[J]. Obstet Gynecol, 2020, 135(6): e237. doi: 10.1097/AOG.0000000000003891 [13] 彭威, 漆洪波. ACOG"妊娠期慢性高血压指南(2019)"解读[J]. 中国实用妇科与产科杂志, 2019, 35(9): 1014. [14] 石晛, 邓芯茹, 钟小翠, 等. 妊娠期高血压疾病相关因素分析[J]. 重庆医学, 2020, 49(3): 457. doi: 10.3969/j.issn.1671-8348.2020.03.026 [15] 符剑花, 于英, 杨善珏. 妊娠期高血压的相关危险因素分析[J]. 广西医科大学学报, 2018, 35(9): 1298. [16] GUTIN I. In BMI we trust: reframing the body mass index as a measure of health[J]. Soc Theory Health, 2018, 16(3): 256. doi: 10.1057/s41285-017-0055-0 [17] 郭晓蒙, 张烨, 王娟, 等. BMI联合血脂对妊娠期高血压及子痫前期的预测价值[J]. 中国妇产科临床杂志, 2019, 20(3): 199. [18] 胥芹, 杨英, 蔺莉, 等. 孕前BMI和孕期增重与孕期血压水平的相关性研究[J]. 中国计划生育学杂志, 2018, 26(10): 941. [19] 李精华, 杨柳, 陈庆, 等. 妊娠前体质指数及妊娠期体质量增加对妊娠并发症和妊娠结局影响的前瞻性队列研究[J]. 中华妇产科杂志, 2019, 54(3): 184. [20] 郭欣, 刘清, 方芳, 等. 妊娠期高血压患者血脂和凝血指标变化及与围产期结局的关系[J]. 中国慢性病预防与控制, 2017, 25(3): 229. [21] 赵明, 李光辉. 孕早期血脂水平与妊娠期高血压的关系研究[J]. 中国妇幼健康研究, 2017, 28(5): 517. doi: 10.3969/j.issn.1673-5293.2017.05.009 [22] 郝晋红, 任丽华, 傅松涛, 等. 妊娠期高血压疾病与血清脂溶性维生素及血脂水平的相关性[J]. 山西医科大学学报, 2018, 49(9): 1100. [23] 潘玲, 莫丽德尔·白山, 严金龙. 不同亚型高血压与靶器官损害的研究进展[J]. 心血管病学进展, 2018, 39(2): 194. [24] 项伟忠, 陈礼平, 杨群菲, 等. 高血压家族史人群隐匿性高血压发生情况及对靶器官损害程度的研究[J]. 中国医师杂志, 2019, 21(9): 1336. doi: 10.3760/cma.j.issn.1008-1372.2019.09.012 [25] BERHE AK, ILESANMI AO, AIMAKHU CO, et al. Effect of pregnancy induced hypertension on adverse perinatal outcomes in Tigray regional state, Ethiopia: a prospective cohort study[J]. BMC Pregnancy Childbirth, 2019, 20(1): 7. [26] 孙芳璨, 韩冰. 妊娠期高血压疾病不良结局预测模型的研究进展[J]. 实用妇产科杂志, 2019, 35(9): 677. [27] 庞静, 聂红艳, 陈伟伟, 等. 妊娠期高血压疾病产妇子宫动脉和胎儿脐动脉超声参数预测妊娠结局的临床价值[J]. 中国计划生育和妇产科, 2019, 11(1): 77. doi: 10.3969/j.issn.1674-4020.2019.01.21 -

 点击查看大图
点击查看大图

图(4)表(7)
计量
- 文章访问数: 4087
- HTML全文浏览量: 1588
- PDF下载量: 6
- 被引次数: 0
