

-
肺癌是世界上发病率及死亡率最高的肿瘤,其中非小细胞肺癌(non-small cell lung cancer,NSCLC)约占80%,且多数病人不能早期发现。有效的治疗方法成了人们关注的焦点,目前针对表皮生长因子受体(epidermal growth factor receptor, EGFR)、间变性淋巴激酶(ALK)及ROS1等突变的靶向药物在临床上已广泛应用,病人的预后得到了极大改善,而大多数基因无突变的病人会选择含铂双药化疗。目前国内外对基因突变靶向治疗耐药和化疗失败的病人尚无规范的治疗方案,临床治疗效果亦不理想[1],关注这些病人的治疗是本研究的出发点。在我国自行研发的靶向药物中,小分子酪氨酸激酶抑制剂占多数,安罗替尼胶囊即为其中的一种,2018年5月,国家食品药品监督管理局批准其用于晚期NSCLC的三线治疗。长春瑞滨软胶囊是国产的长春花碱类的口服化疗药物,使用方便,疗效与注射用长春瑞滨相当,它可避免中心静脉置管或静脉炎的风险。本研究旨在观察安罗替尼胶囊联合长春瑞滨软胶囊双口服药物治疗晚期NSCLC的疗效及安全性,现作报道。
-
(1) 自愿加入本研究,且签署知情同意书;(2)性别不限,年龄≥18岁;(3)参照国际肺癌研究协会(IASLC)第八版的分期标准,经病理组织学或细胞学(除外痰细胞学)诊断为NSCLC,分期为ⅢB~Ⅳ;(3)经影像学证实,至少有一处可评价的靶病灶(参照RECIST1.1标准);(4)EGFR、ALK、ROS1基因检测阴性,进行至少2次系统性化疗后病情进展或不能耐受者(ⅢB期同步放化疗失败);或检测为阳性需接受相应靶向药物治疗后耐药或不可耐受者;(5)ECOG PS评分为0~2分;(6)预计生存期>3个月;(7)实验室检查要求, 治疗前1周, 血常规:白细胞计数≥3.5×109/L, 中性粒细胞计数≥1.5×109/L, 血小板计数≥80×109/L, 血红蛋白≥90 g/L; 肝功能:胆红素≤1.5×正常值上限(ULN); 不存在肝转移者丙氨酸氨基转氨酶(ALT)和天门冬氨酸氨基转氨酶(AST)≤2.5×ULN;肝转移者ALT和AST≤5×ULN; 肾功能:肌酐≤1.5×ULN或肌酐清除率≥55 mL/min; 心脏功能:心脏B超左室射血分数(LVEF)≥50%。
-
(1) 既往有高血压危象病史或未控制的高血压(收缩压≥150 mmHg和/或舒张压≥100 mmHg); 尿蛋白异常(≥2+或24 h尿蛋白定量>1.0 g);(2)空洞或中央型肺鳞状细胞癌,或咯血量>50 mL/d。(3)影像学检查显示肿瘤接近、包绕或侵犯大血管(如肺动脉或上腔静脉),可能引起危及生命的大出血,或研究者判断有出血倾向者;(4)妊娠或哺乳期的女性病人;(5)口服药物不耐受者。
-
入组病人均口服安罗替尼胶囊(12 mg)(正大天晴药业集团,国药准字:H20180004),1次/天,连续口服14 d,休息1周,联合口服长春瑞滨软胶囊(60 mg/m2)(江苏恒瑞有限责任公司,国药准字:H20061234)第1天及第8天各口服1次,21 d为1个周期,直至疾病进展、毒性不能耐受、死亡或病人拒绝。本研究得到我院伦理委员会批准。
-
(1) 近期疗效:每2个治疗周期评价一次; 参照实体瘤评价标准RECIST1.1版本[2]将评价结果分为完全缓解(CR)、部分缓解(PR)、疾病稳定(SD)及疾病进展(PD);客观有效率(ORR)为CR+PR且持续4周以上的病例数占可评价病人总数百分比; 疾病控制率(DCR)为CR+PR+SD且持续4周以上的病例数占可评价疗效病人总数百分比。(2)远期疗效:无进展生存期(PFS)指入组开始至第一次发生疾病进展或任何原因死亡的时间;总生存期(OS)指入组开始至任何原因引起的死亡的时间。(3)不良反应:按照美国国立癌症研究所不良反应标准NCI.CTCAE4.02版评价。
-
所有入组病人均通过门诊、住院及电话随访截至2020年8月。
-
采用生存曲线、Fisher确切概率法、Log-rank检验、Kaplan-Meier单因素法生存分析。
-
2018年8月至2020年2月共纳入本研究晚期NSCLC 30例,男24例,女6例;年龄49~75岁,中位年龄67岁;腺癌19例,鳞癌8例,其他3例。其他临床资料详见表 1。
项目 n 构成比/% 性别 男 24 80.00 女 6 20.00 年龄/岁 < 60 5 16.67 ≥60 25 83.33 ECOG PS评分/分 0~1 17 56.67 2 13 43.33 吸烟史 无 22 73.33 有 8 26.67 病理类型 腺癌 19 63.33 鳞癌 8 26.67 其他 3 10.00 临床分期 Ⅲb期 3 10.00 Ⅳ期 27 90.00 基因检测 未检测 6 20.00 无突变 19 63.33 EGFR突变 4 13.33 ALK突变 1 3.33 既往治疗线数 < 3 19 63.33 ≥3 11 36.67 表 1 30例入组NSCLC病人的临床基本资料
-
30例晚期NSCLC,无CR病例,PR率为13.3%(4/30), SD率为70%(21/30), PD率为16.7%(5/30), ORR为13.3%,DCR为83.3%。临床基本资料中仅ECOG PS评分对近期疗效影响有统计学意义(P < 0.01),其他因素对近期疗效影响均无统计学意义(P>0.05)(见表 2)
因素 CR PR SD PD P 性别 男 0 2 18 4 >0.05 女 0 2 3 1 年龄/岁 < 60 0 0 3 2 >0.05 ≥60 0 4 18 3 ECOG PS评分/分 0~1 0 4 10 0 < 0.01 2 0 0 11 5 吸烟史 无 0 3 16 3 >0.05 有 0 1 5 2 病理类型 腺癌 0 3 14 2 >0.05 鳞癌 0 1 5 2 其他 0 0 2 1 临床分期 Ⅲb期 0 1 1 1 >0.05 Ⅳ期 0 3 20 4 突变情况 未检测 0 1 3 2 >0.05 野生型 0 2 16 1 突变型 0 1 2 2 既往治疗线数 < 3 0 3 13 3 >0.05 ≥3 0 1 8 2 表 2 不同因素对NSCLC病人的近期疗效影响(n)
-
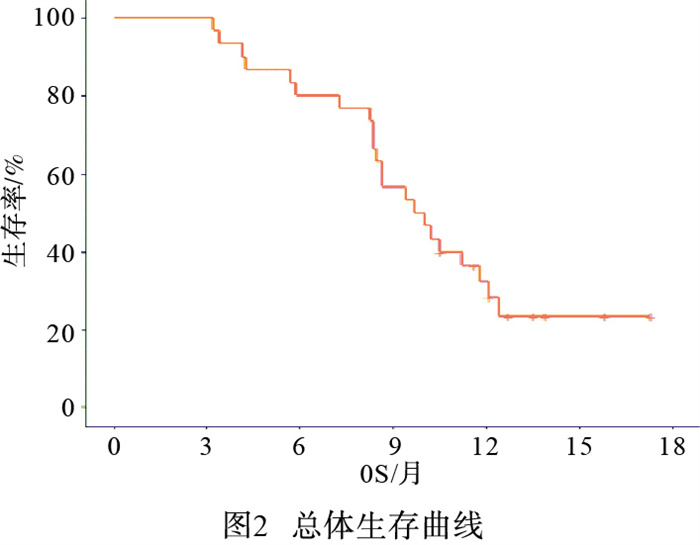
所有入组病人均随访至2020年8月,中位PFS为6.5个月(6.3~6.9个月),中位OS为9.9个月(7.7~11.7个月)(见图 1、2)。

图 1 总体无进展生存曲线

图 2 总体生存曲线
-
Kaplan-Meier单因素分析显示,年龄≥60岁、PS评分为0~1分、无吸烟史、病理类型为腺癌病人的中位PFS和中位OS均分别高于年龄 < 60岁、PS评分2分、有吸烟史、病理类型为鳞癌组的病人(P < 0.05~P < 0.01)(见表 3)。
因素 n 进展人数 中位PFS/月 χ2 P 死亡人数 中位OS/月 χ2 P 性别 男 24 24 6.6(6.313~6.887) 0.79 >0.05 19 8.7(7.26~10.14) 1.73 >0.05 女 6 16 6.1(3.219~8.981) 3 11.2(-) 年龄/岁 < 60 5 25 3.8(0.794~6.806) 6.09 < 0.05 5 17 5.7(2.69~8.71) 10.5(8.6-12.4) 13.54 < 0.01 ≥60 25 25 6.7(6.333~7.067) 17 10.5(8.6-12.4) ECOG PS评分/分 0~1 17 17 8.2(6.889~9.511) 24.73 < 0.01 9 12.4(11.41~13.39) 15.99 < 0.01 2 13 13 5.6(2.194~9.006) 13 8.4(5.31-11.49) 吸烟史 无 22 22 6.6(5.336~7.864) 4.79 < 0.05 15 10.5(8.15~12.85) 4.56 < 0.05 有 8 8 5.2(1.597~8.803) 7 87.3(4.53~10.07) 病理类型 腺癌 19 19 6.8(5.378~8.222) 12 11.8(9.83~13.77) 鳞癌 8 8 6.2(2.319~10.081) 7.40 < 0.05 7 8.353(5.99~10.61) 8.90 < 0.05 其他 3 3 5.2(0.719~9.681) 3 7.3(2.5~12.1) 临床分期 Ⅲb期 3 3 5.9(0.299~11.501) 1.39 >0.05 3 8.5(4.34~12.66) 1.76 >0.05 Ⅳ期 27 27 6.6(6.346~6.854) 19 10(8.13~11.87) 基因检测 未检测 6 6 6.5(1.339~11.661) 4.28 >0.05 5 8.853(4.1~12.5) 1.84 >0.05 无突变 19 19 6.6(6.038~7.162) 15 10(7.44~12.56) 既往化疗线数 < 3 19 19 6.4(5.753~7.047) 3.60 >0.05 13 11.2(8.92~13.48) 3.44 >0.05 ≥3 11 11 6.4(5.753~7.047) 9 8.5(8.07~8.93) 表 3 影响进展及死亡的单因素分析
-
本研究中最常见的不良反应前3位为恶心、呕吐,发生率为36.67%;疲乏的发生率为33.33%,腹泻的发生率为30.00%。主要为1~2级。经过对症治疗,病情好转。1例出现3级腹泻,停药后缓解,未出现4级不良反应(见表 4)。
分类 1级 2级 3级 合计 恶心、呕吐 11(36.67) 0(0.00) 0(0.00) 11(36.67) 疲乏 10(33.33) 0(0.00) 0(0.00) 10(33.33) 腹泻 5(16.67) 3(10.00) 1(3.33) 9(30.00) 白细胞减少 5(16.67) 1(3.33) 0(0.00) 6(20.00) 手足综合征 5(16.67) 1(3.33) 0(0.00) 6(20.00) 口腔黏膜炎 4(13.33) 1(3.33) 0(0.00) 5(16.67) 贫血 3(10) 1(3.33) 0(0.00) 4(13.33) 高血压 3(10) 0(0.00) 0(0.00) 3(10.00) 纳差 2(6.67) 0(0.00) 0(0.00) 2(6.67) 转氨酶升高 2(6.67) 0(0.00) 0(0.00) 2(6.67) 甲状腺功能减低 1(3.33) 1(3.33) 0(0.00) 2(6.67) 蛋白尿 1(3.33) 0(0.00) 0(0.00) 1(3.33) 咯血 1(3.33) 0(0.00) 0(0.00) 1(3.33) 表 4 30例入组病人不良反应发生情况[n;百分率(%)]
-
晚期NSCLC是肺癌治疗的重点,化疗、靶向药物治疗以及近年出现的免疫治疗是主要治疗方法[3]。针对基因突变的靶向药物治疗是其中一种重要的治疗方式[4]。随着靶向治疗的常规开展,基因突变型的晚期NSCLC取得了质的突破,显著延长了OS, 但靶向药物耐药的驱动基因阳性病人,以及基因突变阴性病人靶向治疗无法获益或二线化疗后的治疗目前没有标准治疗,而免疫治疗因为经济费用的原因,选择的人群相对较少,目前这部分人群成为晚期NSCLC治疗中急需解决的难题[5-6]。
肿瘤可依靠新生血管的营养供给来生长,通过抑制血管内皮细胞生长因子受体(VEGFR)、血小板衍生生长因子受体(PDGFR)、纤维母细胞生长因子受体(FGFR)和干细胞因子受体(C-kit)等,从而可抑制肿瘤的血管生成及肿瘤细胞增长[7-9]。长春瑞滨注射液是NSCLC化疗中常有的药物,它通过抑制微管蛋白聚集从而干扰细胞有丝分裂发挥抗肿瘤作用,静脉给药易引起静脉炎。长春瑞滨软胶囊的疗效与其相当, 且口服便利,不良反应小[10]。潘跃银等[11]研究表明,口服长春瑞滨软胶囊联合静脉注射顺铂治疗晚期NSCLC, 与注射用长春瑞滨的疗效相当,安全可控,经济实惠。安罗替尼胶囊被CSCO肺癌指南推荐用于晚期NSCLC的三线治疗是基于ALTER0303的临床研究,该研究[12-13]提示ORR及DCR分别为9.2%及81.0%,而本研究的ORR为13.3%,DCR为83.3%,比其略好, 与刘楠等[14]研究结果的近期疗效相仿。这可能与联合化疗药长春瑞滨软胶囊增加了近期疗效有关。安罗替尼胶囊与化疗药物联合使用可取得明显的疗效[15]。亚组分析ALTER-0303研究中的ECOG PS评分全部为0分的病人,本研究有13例评分为2分的病人,相对这部分人群的预后更差,加用一个口服化疗药却取得了优于该研究的结果,很值得我们临床医生的思考,且为双口服药,居家即可完成,使用方便,若遇特殊时期如疫情防控期间,优势更凸显,尤其在二线治疗后病人的ECOG PS评分较差的前提下,安罗替尼胶囊联合长春瑞滨胶囊可以达到更优的近期疗效。本研究的ECOG PS评分对近期疗效的影响有统计学意义,提示ECOG PS评分为0~1分的病人,近期疗效更佳。
ALTER0303的结果显示[12-13]安罗替尼胶囊治疗的中位PFS及OS分别为5.4个月和9.6个月。本研究中位PFS为6.5个月(6.3~6.9)较之延长1个月,中位OS为9.9个月(7.7~11.7),与之相仿。提示在短期疾病控制方面,联合化疗药具有优势,但OS无明显差异,这可能与这部分病人有效的治疗方法有限有关。但皇甫娟等[16]研究提示安罗替尼胶囊联合含铂双药化疗相对于单药安罗替尼胶囊的ORR分别为51.4%及31.4%;且PFS和OS也显著延长。本研究影响进展及死亡的单因素分析表明,ECOG PS评分为0~1分,中位PFS及中位OS比PS评分为2分的病人长(P< 0.01),这与CHENG等[17]研究结果中ECOG PS评分对生存的影响相符。本研究年龄、吸烟及病理类型的单因素分析中均有统计学意义,提示年龄<60岁的病人对2种药物联合治疗的耐受性更佳,而不吸烟及腺癌病人的中位PFS及中位OS更长,这可能表明这部分病人对抗血管靶向药及化疗更敏感,或可能有再次靶向治疗或免疫治疗的机会,而与基因检测情况、临床分期及既往治疗线数无相关性,国内外关于以上因素的单因素分析文献报道较少,有待进一步研究及探索。
金振兴等[18]研究表明口服安罗替尼胶囊后最常出现的不良反应为疲乏、高血压、厌食,1~2级占多数,少数为3级以上,经对症治疗、减少剂量或停药后,可控制不良反应。本研究最常见的不良反应为恶心、呕吐,发生率为36.7%,疲乏的发生率为33.3%,腹泻的发生率为30%,未出现4级不良反应,主要为1~2级,经对症处理后好转,1例出现3级腹泻,停药后缓解。本研究中发生率较高的不良反应为恶心、呕吐,考虑可能为口服长春瑞滨软胶囊化疗引起的消化道不良反应。在ALTER0303的研究[12-13]中,53例鳞癌病人咯血的发生率为20.4%(60/294),本研究报告了8例鳞癌,未发现严重出血,提示安罗替尼软胶囊的耐受性较好,不良反应可控。
刘楠等[14, 19]采用EORTC QLQ-LCI3和EORTC QLQ-C30生活质量调查问卷,与安慰剂比较发现,安罗替替尼胶囊改善了晚期NSCLC病人的生活质量。本研究未对病人的生活质量做进一步的调查和分析,有待于后续的工作中进一步研究。ZHANG等[20-21]分别研究了安罗替尼胶囊在肺癌脑转移及在TP53突变病人中的应用,这给我们进一步研究提供了方向。
综上所述,安罗替尼胶囊联合长春瑞滨软胶囊治疗晚期NSCLC的治疗有较好的疗效,不良反应可控,安全性良好,双口服,使用方便。但本研究样本量较小,需要进一步扩大样本量及进行更深入的亚组研究。
安罗替尼胶囊联合长春瑞滨软胶囊治疗晚期非小细胞肺癌的临床观察
Clinical effects of anlotinib capsule combined with vinorelbine soft capsule in the treatment of advanced non-small cell lung cancer
-
摘要:
目的 观察安罗替尼胶囊联合长春瑞滨软胶囊治疗晚期非小细胞肺癌的的疗效及安全性。 方法选择病理确诊的ⅢB/Ⅳ期非小细胞肺癌病人,口服安罗替尼胶囊(12 mg),1次/天,连续14 d,联合口服长春瑞滨软胶囊(60 mg/m2)第1天及第8天,21 d为1个周期,直至疾病进展或毒性不能耐受。记录病人客观反应率、疾病控制率、无进展生存期、总生存期及不良反应。 结果 共纳入研究30例病人,无完全缓解病例,部分缓解4例,疾病稳定21例,疾病进展5例。客观缓解率为13.3%,疾病控制率为83.3%。中位无进展生存期为6.5个月(6.3~6.9个月);中位总生存期为9.9个月(7.7~11.7个月)。在影响进展及死亡的单因素分析中,年龄≥60岁、PS评分为0~1分、无吸烟史、病理类型为腺癌病人的中位无进展生存时间和中位生存时间均分别高于年龄 < 60岁、PS评分为2分、有吸烟史、病理类型为鳞癌组的病人(P < 0.05~P < 0.01)。最常见的不良反应为恶心、呕吐,发生率为36.7%,疲乏的发生率为33.3%,腹泻的发生率为30%,但多为1~2级,对症治疗后改善。 结论 安罗替尼胶囊联合长春瑞滨软胶囊双口服药物对晚期非小细胞肺癌可达到较好的控制疾病进展,延长病人生存期的目的,且不良反应可控。 Abstract:ObjectiveTo observe the efficacy and safety of anlotinib capsule combined with vinorelbine soft capsule in the treatment of advanced non-small cell lung cancer(NSCLC). MethodsThe patients with stage ⅢB/Ⅳ NSCLC confirmed by pathology were treated with anlotinib capsule(12 mg) once a day for 14 days, and combined with vinorelbine soft capsule(60 mg/m2) orally on day 1 and day 8, 21 days for a cycle, and until disease progression or toxicity became intolerant.The objective response rates, disease control rates, progression-free survival, overall survival and adverse reactions were recorded. ResultsA total of 30 patients were included in this study, which included no complete response cases, 4 partial response cases, 21 stable disease cases and 5 progressive disease cases.The objective remission rate was 13.3%, and the disease control rate was 83.3%.The median progression-free survival was 6.5(6.3-6.9) months, and the median overall survival was 9.9(7.7-11.7) months.In the univariate analysis affecting progression and death, the median progression-free survival time and median survival time in patients with≥60 years old, PS score for 0-1, no smoking history and pathological type of adenocarcinoma were higher than those in patients with age < 60 years old, PS score for 2, smoking history and pathological type of squamous cell carcinoma(P < 0.05 to P < 0.01).The nausea and vomiting(36.7%), fatigue(33.3%) and diarrhea(30%) were the most common adverse reactions, but most of them were grade 1 or 2, which could be improved after symptomatic treatment. ConclusionsThe anlotinib capsule combined with vinorelbine soft capsule in the treatment of NSCLC can better control the disease progression, achieve the purpose of prolonging the patient′s survival time, and the adverse reactions can be controlled. -
Key words:
- non-small cell lung cancer /
- anlotinib capsule /
- vinorelbine soft capsule /
- oral /
- curative effect
-
表 1 30例入组NSCLC病人的临床基本资料
项目 n 构成比/% 性别 男 24 80.00 女 6 20.00 年龄/岁 < 60 5 16.67 ≥60 25 83.33 ECOG PS评分/分 0~1 17 56.67 2 13 43.33 吸烟史 无 22 73.33 有 8 26.67 病理类型 腺癌 19 63.33 鳞癌 8 26.67 其他 3 10.00 临床分期 Ⅲb期 3 10.00 Ⅳ期 27 90.00 基因检测 未检测 6 20.00 无突变 19 63.33 EGFR突变 4 13.33 ALK突变 1 3.33 既往治疗线数 < 3 19 63.33 ≥3 11 36.67  下载: 导出CSV
下载: 导出CSV
表 2 不同因素对NSCLC病人的近期疗效影响(n)
因素 CR PR SD PD P 性别 男 0 2 18 4 >0.05 女 0 2 3 1 年龄/岁 < 60 0 0 3 2 >0.05 ≥60 0 4 18 3 ECOG PS评分/分 0~1 0 4 10 0 < 0.01 2 0 0 11 5 吸烟史 无 0 3 16 3 >0.05 有 0 1 5 2 病理类型 腺癌 0 3 14 2 >0.05 鳞癌 0 1 5 2 其他 0 0 2 1 临床分期 Ⅲb期 0 1 1 1 >0.05 Ⅳ期 0 3 20 4 突变情况 未检测 0 1 3 2 >0.05 野生型 0 2 16 1 突变型 0 1 2 2 既往治疗线数 < 3 0 3 13 3 >0.05 ≥3 0 1 8 2
下载: 导出CSV
表 3 影响进展及死亡的单因素分析
因素 n 进展人数 中位PFS/月 χ2 P 死亡人数 中位OS/月 χ2 P 性别 男 24 24 6.6(6.313~6.887) 0.79 >0.05 19 8.7(7.26~10.14) 1.73 >0.05 女 6 16 6.1(3.219~8.981) 3 11.2(-) 年龄/岁 < 60 5 25 3.8(0.794~6.806) 6.09 < 0.05 5 17 5.7(2.69~8.71) 10.5(8.6-12.4) 13.54 < 0.01 ≥60 25 25 6.7(6.333~7.067) 17 10.5(8.6-12.4) ECOG PS评分/分 0~1 17 17 8.2(6.889~9.511) 24.73 < 0.01 9 12.4(11.41~13.39) 15.99 < 0.01 2 13 13 5.6(2.194~9.006) 13 8.4(5.31-11.49) 吸烟史 无 22 22 6.6(5.336~7.864) 4.79 < 0.05 15 10.5(8.15~12.85) 4.56 < 0.05 有 8 8 5.2(1.597~8.803) 7 87.3(4.53~10.07) 病理类型 腺癌 19 19 6.8(5.378~8.222) 12 11.8(9.83~13.77) 鳞癌 8 8 6.2(2.319~10.081) 7.40 < 0.05 7 8.353(5.99~10.61) 8.90 < 0.05 其他 3 3 5.2(0.719~9.681) 3 7.3(2.5~12.1) 临床分期 Ⅲb期 3 3 5.9(0.299~11.501) 1.39 >0.05 3 8.5(4.34~12.66) 1.76 >0.05 Ⅳ期 27 27 6.6(6.346~6.854) 19 10(8.13~11.87) 基因检测 未检测 6 6 6.5(1.339~11.661) 4.28 >0.05 5 8.853(4.1~12.5) 1.84 >0.05 无突变 19 19 6.6(6.038~7.162) 15 10(7.44~12.56) 既往化疗线数 < 3 19 19 6.4(5.753~7.047) 3.60 >0.05 13 11.2(8.92~13.48) 3.44 >0.05 ≥3 11 11 6.4(5.753~7.047) 9 8.5(8.07~8.93)
下载: 导出CSV
表 4 30例入组病人不良反应发生情况[n;百分率(%)]
分类 1级 2级 3级 合计 恶心、呕吐 11(36.67) 0(0.00) 0(0.00) 11(36.67) 疲乏 10(33.33) 0(0.00) 0(0.00) 10(33.33) 腹泻 5(16.67) 3(10.00) 1(3.33) 9(30.00) 白细胞减少 5(16.67) 1(3.33) 0(0.00) 6(20.00) 手足综合征 5(16.67) 1(3.33) 0(0.00) 6(20.00) 口腔黏膜炎 4(13.33) 1(3.33) 0(0.00) 5(16.67) 贫血 3(10) 1(3.33) 0(0.00) 4(13.33) 高血压 3(10) 0(0.00) 0(0.00) 3(10.00) 纳差 2(6.67) 0(0.00) 0(0.00) 2(6.67) 转氨酶升高 2(6.67) 0(0.00) 0(0.00) 2(6.67) 甲状腺功能减低 1(3.33) 1(3.33) 0(0.00) 2(6.67) 蛋白尿 1(3.33) 0(0.00) 0(0.00) 1(3.33) 咯血 1(3.33) 0(0.00) 0(0.00) 1(3.33)
下载: 导出CSV
-
[1] ETTINGER DS, WOOD DE, AISNER DL, et al. Non-small cell lung cancer, version 5.2017, nccn clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2017, 15(4): 504. doi: 10.6004/jnccn.2017.0050 [2] EISENHAUER EA, THERASSE P, BOGAERTS J, et al. New response evaluation criteria in solid tumors: revised RECIST guideline(version 1.1)[J]. Eur J Cancer, 2009, 45(2): 228. doi: 10.1016/j.ejca.2008.10.026 [3] FAEHLING M, ACHENBACH J, STAIB P, et al. Erlotinib in routine clinical practice for first-line maintenance therapy in patients with advanced non-small cell lung cancer(NSCLC)[J]. J Cancer Res Clin Oncol, 2018, 144(7): 1375. doi: 10.1007/s00432-018-2649-x [4] LIU MH, ZHANG HY, LI Y, et al. HOTAIR, a long noncoding RNA, is a marker of abnormal cell cycle regulation in lung cancer[J]. Cancer Sci, 2018, 109(9): 2717. doi: 10.1111/cas.13745 [5] LEONETTI A, ASSARAF YG, VELTSISTA PD, et al. Micrornas as a drug resistance mechanism to targeted therapies in egfr-mutated NSCSLC: Current implications and future directions[J]. Drug Resist Updat, 2019, 42: 1. doi: 10.1016/j.drup.2018.11.002 [6] LIM SM, SYN NL, CHO BC, et al. Acquired resistance to EGFR targeted therapy in non-small cell lung cancer: mechanisms and therapeutic strategies[J]. Cancer Treat Rev, 2018, 65: 1. doi: 10.1016/j.ctrv.2018.02.006 [7] LIN B, SONG X, YANG D, et al. Anlotinib inhibits angiogenesis via suppressing the activation of VEGFR2, PDGFRβ and FGFR1[J]. Gene, 2018, 654: 77. doi: 10.1016/j.gene.2018.02.026 [8] SHEN G, ZHENG F, REN D, et al. Anlotinib: a novel multi-targeting tyrosine kinase inhibitor in clinical development[J]. J Hematol Oncol, 2018, 11(1): 120. doi: 10.1186/s13045-018-0664-7 [9] TAURIN S, YANG CH, REYES M, et al. Endomemai cancers harboring mutated fibroblast growth factor receplor 2 protein are suocessfully treated witll a new smaIl tyrosine kinase inhibitor in an onhotopic mouse model[J]. Int J Gynecol cancer, 2018, 28(1): 152. doi: 10.1097/IGC.0000000000001129 [10] LUSH RM, MCCUNE JS, TETTEH L, et al. The absolute bioavailability of oral vinorelbine in patients with solid tumors[J]. Cancer Chemother Pharnacol, 2005, 56(6): 578. doi: 10.1007/s00280-005-1025-0 [11] 潘跃银, 郝吉庆, 顾康生, 等. 国产长春瑞滨软胶囊的Ⅱ期临床研究[J]. 临床肿瘤学杂志, 2004, 9(4): 376. doi: 10.3969/j.issn.1009-0460.2004.04.013 [12] HAN B, LI K, WANG Q, et al. Effect of anlotinib as a third-line or further treatment on overall survival of patients with advanced non-small cell lung cancer: the ALTER 0303 phase 3 randomized clinical trial[J]. JAMA Oncol, 2018, 4(11): 1625. [13] WANG L, HE Z, YANG S, et al. The impact of previous therapy strategy on the efficiency of anlotinib hydrochloride as a third-line treatment on patients with advanced non-small cell lung cancer(NSCLC): a subgroup analysis of ALTER0303 trial[J]. Transl Lung Cancer Res, 2019, 8(5): 575. doi: 10.21037/tlcr.2019.09.21 [14] 刘楠, 吴秀伟, 李烦繁, 等, 安罗替尼三线及以上治疗晚期非小细胞肺癌近期疗效及生命质量分析[J]. 国际肿瘤学杂志, 2019, 46(3): 147. doi: 10.3760/cma.j.issn.1673-422X.2019.03.004 [15] 孟令新, 曾琴琴, 孟芹, 等. 安罗替尼与贝伐珠单抗分别联合紫杉醇加卡铂治疗晚期肺腺癌的临床效果[J]. 中国医药, 2019, 14(8): 1164. doi: 10.3760/j.issn.1673-4777.2019.08.011 [16] 皇甫娟, 李文永, 张慧辉. 安罗替尼胶囊治疗晚期非小细胞肺癌对患者VEGF水平及生存期的影响[J]. 实用癌症杂志, 2020, 3(35): 360. [17] CHENG JD, CHAI LX, ZHAO ZP, et al. Effificacy and safety of anlotinib for patients with advanced nsclc who progressed after standard regimens and the preliminary analysis of an effificacy predictor[J]. Cancer Manag Res, 2020, 12: 5641. doi: 10.2147/CMAR.S253366 [18] 金振兴, 杜秀平. 盐酸安罗替尼治疗晚期非小细胞肺癌的临床观察[J]. 临床与病理杂志, 2020, 40(4): 911. [19] SI X, ZHANG L, WANG H, et al. Quality of life results from a randomized, placebo-controlled, multi-center phase Ⅲ trial of anlotinib in patients with advanced non-small cell lung cancer[J]. Lung Cancer, 2018, 122: 32. doi: 10.1016/j.lungcan.2018.05.013 [20] ZHANG C, KONG FW, WU WB, et al. First-line pemetrexed and carboplatin plus anlotinib for epidermal growth factor receptor wild-type and anaplastic lymphoma kinase-negative lung adenocarcinoma with brain metastasis: A case report and review of the literature[J]. Medicine(Baltimore), 2020, 99(36): e22128. [21] FANG S, CHENG W, ZHANG M, et al. Association of TP53 mutation with response to anlotinib treatment in advanced non-small cell lung cancer[J]. Onco Targets Ther, 2020, 13: 6645. doi: 10.2147/OTT.S257052 -

 点击查看大图
点击查看大图

图(2)表(4)
计量
- 文章访问数: 4713
- HTML全文浏览量: 2959
- PDF下载量: 11
- 被引次数: 0
