

-
回顾性分析2017年3月至2020年12月就诊于我科的急性脑梗死病人,诊断标准:中国急性缺血性脑卒中诊治指南(2018)[7]及急性缺血性卒中血管内治疗中国指南(2018)[8]。最终选取的33例脑梗死病人纳入本研究,根据治疗方式的不同分为静脉溶栓组(A组,17例)和静脉溶栓联合介入治疗组(B组,16例)。2组病人年龄、性别、吸烟史、血压、血糖、总胆固醇(TC)等差异均无统计学意义(P>0.05)(见表 1),具有可比性。
项目 A组(n=17) B组(n=16) t P 年龄/岁 71.94±8.42 65.81±13.56 1.57 >0.05 性别(男) 11(64.7) 7(43.8) 1.46# >0.05 吸烟史 10(58.8) 10(62.5) 0.05# >0.05 血压/mmHg 154.59±11.52 150.6±8.19 1.14 >0.05 血糖/(mmol/L) 7.21±2.01 6.17±1.79 1.57 >0.05 TG/(mmol/L) 1.22±0.62 1.25±0.64 0.15 >0.05 TC/(mmol/L) 5.31±1.31 5.54±1.38 0.50 >0.05 LDL-C/(mmol/L) 2.35±0.53 2.05±0.37 1.89 >0.05 FDP/(mg/L) 3.75±1.87 4.96±2.24 1.70 >0.05 D-二聚体/(mg/L) 1.82±1.72 2.85±1.90 1.64 >0.05 FIB/(g/L) 3.15±0.99 3.24±1.18 0.23 >0.05 入院时NIHSS评分/分 15.53±5.50 16.00±4.95 0.26 >0.05 入院时Barthel评分/分 14.42±15.99 17.81±21.29 0.52 >0.05 溶栓等待时间/h 2.82±0.73 2.50±0.98 1.08 >0.05 #示χ2值。TG:三酰甘油;LDL-C:低密度脂蛋白;FDP:纤维蛋白原降解产物;FIB:纤维蛋白原 表 1 2组病人一般资料(x±s)
-
(1) 病人因急性脑梗死发病导致出现神经功能缺损症状;(2)症状出现 < 4.5 h;(3)病人行静脉溶栓或介入治疗,取得病人或其家属同意,并均需签署知情同意书。
-
(1) 病人的CT检查结果提示为大面积脑梗死(病变面积>1/3大脑中动脉分布区);(2)病人在近3个月发生卒中病史或重大的头颅外伤病史,在近2周内有过大型的外科手术或有严重的外伤史;(3)既往有颅内出血的病人,临床不能排除颅内出血可能的病人;(4)病人有明确的颅内肿瘤、动静脉畸形、颅内动脉瘤病史;(5)血压升高:收缩压≥180 mmHg或舒张压≥100 mmHg且药物不能控制的病人;(6)病人目前有活动性内出血或有急性出血可能;(7)血糖 < 2.7 mmol/L;(8)妊娠。
-
应用0.9 mg/kg阿替普酶,将其中10%药物剂量通过静脉推注(1 min内),其余90%药物通过持续静脉泵入(60 min内)完成治疗,使用药物的总量不得超过90 mg。在对病人进行静脉溶栓的过程中需要密切监测血压、脉搏和呼吸及病人的意识水平;治疗完成后进行神经功能评分,如若出现进一步意识障碍或障碍程度加深,病人血压急剧升高,剧烈头痛、恶心和呕吐、神经定位体征变化,则需要停止溶栓,立即给予CT检查,排除出血等并发症;在进行常规溶栓治疗结束后,需要在24 h后给予头颅CT的检查,排除出血后再给予阿司匹林等常规神经内科药物治疗及护理。
-
监测病人的生命体征,并给予病人神经内科的常规治疗和护理,建立静脉通路,先给予病人静脉溶栓治疗(与A组治疗方法相同),然后病人平躺,腹股沟区给予聚维酮碘消毒,铺无菌巾,给予局麻,应用改良Seldinger技术,用手触摸到右侧腹股沟区股动脉搏动最强处,取该处为穿刺点,放置6F~8F鞘,在泥鳅导丝的引导下,应用单弯造影管注射造影剂,有效显示病变血管的部位、程度及血管的代偿状况,并进行评价,评价后选用Rebar-27的微导管,塑形,在微导丝的协助下跨过可疑血栓部位,再通过微导管进行造影,进一步评估血栓形态及代偿的血管情况,选取Solitaire-FR支架(根据病人的血管情况,可选用对应合适型号的支架)进行取栓或联合ACE导管进行抽吸,如进行取栓,需在病变血管可能存在血栓的部位释放支架取栓,稍停留后,在同时负压吸引导引导管,缓慢回收Solitaire-FR支架系统至体外,观察栓子的情况,等待15 min后再通过造影评估血管的再通情况,如血管再通情况差,可能需要再次行机械取栓;若采用联合抽吸的方式,则将导管送至血管闭塞处的前端,在负压持续抽吸的情况下逐渐撤出ACE导管, 观察血栓,并再次造影评价血管情况,如有必要需辅助球囊扩张术,直至病变的血管血流恢复通畅良好(TICI分级Ⅱb~Ⅲ级),再回撤导引导管,结束手术, 同样需要在24 h后给予头颅CT的检查,排除出血后再给予阿司匹林等常规神经内科药物治疗及护理常规。
-
记录病人入院时、术后24 h与术后7 d的NIHSS评分和Barthel指数评分,分析影响急性脑梗死发生的关键诱发因素,比较不同治疗方法对2组病人的预后的影响效果。
-
采用t检验、χ2检验、Pearson相关分析和线性回归分析。
-
血压、血糖、TC水平和血浆D-二聚体水平、FDP以及吸烟史与急性脑梗死病人入院后的NIHSS评分均呈正相关关系(P < 0.05~P < 0.01)(见表 2)。
危险因素 病人入院时NIHSS评分 r p 吸烟史 0.388 <0.05 血压 0.768 <0.01 血糖 0.559 <0.01 TG 0.220 >0.05 TC 0.644 <0.01 LDL-C -0.258 >0.05 FDP 0.521 <0.01 D二聚体 0.641 <0.01 FIB 0.191 >0.05 表 2 急性脑梗死病人NIHSS评分与可控性危险因素的相关性
-
A组病人治疗后7 d和B组病人治疗后24 h、7 d的NIHSS评分变化均与等待治疗时间长短有关,等待治疗时间越短,NIHSS评分改善越明显(P < 0.05~P < 0.01)。同时,溶栓等待时间越短,病人的Barthel评分改善越明显(P < 0.01)。治疗后24 h、7 d,B组病人NIHSS评分和Barthel评分改善相对A组改善均更加明显(P < 0.05~P < 0.01)(见表 3)。取栓治疗前后对比见图 1。
分组 n ≤2 h >2 h t P 治疗后NIHSS评分差值 治疗24 h后 A组 17 0.67±0.52 0.45±0.52 0.80 >0.05 B组 16 5.44±2.07 3.14±1.46 2.49 <0.05 t — 5.48 4.55 — — P — <0.01 <0.01 — — 治疗7 d后 A组 17 6.67±3.20 0.91±2.81 3.85 <0.01 B组 16 10.22±2.73 6.43±1.90 3.12 <0.01 t — 2.31 4.55 — — P — <0.05 <0.01 — — 治疗7 d后Barthel评分差值 A组 17 15.83±11.58 2.50±2.64 3.57 <0.01 B组 16 42.22±21.08 8.57±8.02 3.98 <0.01 t — 2.78 2.25 — — P — <0.01 <0.05 — — 表 3 2组溶栓时间窗对NIHSS评分和Barthel评分的影响(x±s)
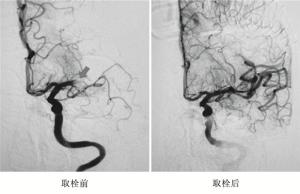
图 1 溶栓治疗后, 介人取栓前后效果对比
-
急性脑梗死的发病特点为起病迅速,死亡率高、致残率高,病情凶险,严重威胁病人生存率及病后生活质量。脑梗死病人的临床表现与闭塞血管供血的脑功能区病变部位及范围有关,当闭塞血管为主要供血血管,且闭塞时间长,未接受及时的治疗,病人则出现更严重症状[9]。因此,及时有效的诊断和时效性合理对症的治疗策略对改善急性脑梗死病人的预后具有极为重要的价值。急性脑梗死的治疗重点是短时间内迅速恢复缺血脑组织的血氧供给,恢复闭塞的脑血管,保护脑组织,促进神经功能的最大可能性的恢复[10]。目前,在时间窗引导下早期溶栓质量一种是临床公认的有效治疗方法,同时介入治疗使闭塞的血管尽可能地在短时间内再通也在临床应用当中逐渐被证明是切实有效的治疗方法[4]。急性脑梗死病人在有效时间窗内接受静脉溶栓治疗是保证良好预后的关键,而到目前为止,重组组织型纤溶酶原激活剂(rt-PA)已被明确是能降低缺血性脑卒中病人致残率的药物。静脉溶栓联合介入取栓治疗能够为急性脑梗死病人的临床疗效提供重要保障,在没有rt-PA应用禁忌证的情况下, rt-PA静脉溶栓联合介入取栓适用于大部分急性脑梗死病人,对血管再通以及改善病人神经功能有着重要作用,同时治疗后很少出现后遗症,这对于改变脑梗死治疗现状有着积极的意义。同时研究表明,当急性基底动脉闭塞病人经溶栓和介入治疗后,生存状况得到明显改善[11-14]。
NIHSS评分具有良好的可信性和有效性,用以确定脑卒中病人神经功能缺陷的严重程度,被广泛用于评估急性缺血性卒中的严重程度, 有研究发现,发病超过4.5 h接受静脉溶栓治疗,病人仍然能够得到有效治疗,从而改善急性脑梗病人的长期预后[15]。我们通过对病人治疗前后NIHSS评分的改善情况进行分析,将符合纳入标准的病人分为2组,其中一组病人采用静脉溶栓治疗联合介入治疗的方法,探讨这种桥接治疗的方法是否可以更进一步改善病人预后,结果显示,大多数急性脑梗死病人在发病后积极接受溶栓治疗时可以获得良好的预后,而溶栓联合介入的治疗对急性脑梗死病人的治疗效果可能更佳。本研究结果表明,联合治疗的病人比单独溶栓治疗的病人治疗后Barthel评分更高,而NIHSS评分更低,证明接受了联合治疗方法的病人生存状况得到了很大改善。
目前研究者认为血管再灌注是急性脑梗死治疗的直接措施,能有效降低病人的死亡率[16]。此外,我们的数据提示急性脑梗死的发生与病人凝血功能存在着一定的关系,纤溶亢进的病人急性脑梗死发生概率越高。本研究表明,经溶栓治疗的病人凝血能力明显降低,这有助于血栓的溶解,而介入治疗对凝血条件改善的影响较少。因此,联合治疗的方法在临床中可以有效、安全地应用[4]。同时,溶栓时间窗对急性脑梗死病人的恢复十分重要,溶栓等待时间越长,溶栓效果越差,病人预后也越差[5]。
综上,静脉溶栓联合介入治疗可有效改善脑动脉栓塞病人的预后。因本次研究的病例数有限,有少数溶栓治疗病人预后改善效果可能不太明显,但总体可以说明缩短病人溶栓治疗等待时间对于病人的预后改善非常重要,急性脑梗死病人应尽早应用溶栓或溶栓联合介入治疗,同时应重视监测病人的基本生命体征,对高血压、凝血功能较差、有吸烟史等高危因素的病人,在治疗的同时倡导病人合理的生活习惯,以降低该病的发生率,改善病人的预后。
静脉溶栓联合介入取栓对急性脑梗死病人预后改善的有效性分析
Effectiveness analysis of intravenous thrombolysis combined with interventional thrombectomy in improving the prognosis of patients with acute cerebral infarction
-
摘要:
目的研究急性脑梗死病人静脉溶栓联合介入取栓术是否能够有效改善病人预后。 方法选取33例急性脑梗死病人,依据治疗方式的不同分为静脉溶栓组(A组,17例)、静脉溶栓联合介入治疗组(B组,16例)。收集所有病人治疗前后的相关临床资料,主要包括:性别、年龄、吸烟史、血压、血糖水平、总胆固醇水平、溶栓治疗等待时间等,分析急性脑梗死相关危险因素及病人治疗前后的美国国立卫生研究院卒中量表(NIHSS)评分和Barthel指数评分变化,比较病人的预后及生活能力差异。 结果病人的血压水平、血糖水平、总胆固醇水平、血浆D-二聚体水平、纤维蛋白原降解产物以及吸烟史与急性脑梗死病人入院后的NIHSS评分均呈正相关关系(P < 0.05~P < 0.01)。急性脑梗死病人的治疗效果及预后与接受治疗的等待时间和治疗方法有密切关系,A组病人治疗后7 d和B组病人治疗后24 h、7 d后的NIHSS评分变化均与等待治疗时间长短有关,等待治疗时间越短,NIHSS评分改善越明显(P < 0.05~P < 0.01)。同时,溶栓等待时间越短,病人的Barthel评分改善越明显(P < 0.01)。治疗后24 h及7 d,B组病人NIHSS评分和Barthel评分改善相对A组均改善更加明显(P < 0.01)。 结论急性脑梗死病人从发病到接受溶栓治疗的时间越短越有助于病人的恢复,静脉溶栓联合介入取栓治疗对急性脑梗病人的恢复效果优于单纯静脉溶栓治疗。 Abstract:ObjectiveTo study whether intravenous thrombolysis combined with interventional thrombectomy can effectively improve the prognosis of patients with acute cerebral infarction. MethodsThirty-three patients with acute cerebral infarction were selected and randomly divided into intravenous thrombolysis group (group A, 17 cases) and intravenous thrombolysis combined with interventional thrombectomy group (group B, 16 cases) according to different treatment methods.Relevant clinical data of all patients before and after treatment, including gender, age, smoking history, blood pressure, blood sugar level, total cholesterol level, waiting time for thrombolytic therapy and so on were collected.The risk factors of acute cerebral infarction and the changes of the National Institutes of Health stroke scale (NIHSS) score and Barthel index score between before and after treatment were analyzed, and the prognosis and living ability of patients were compared. ResultsThe levels of blood pressure, blood glucose, total cholesterol, plasma D dimer, fibrinogen degradation products and smoking history were positively correlated with the NIHSS score after admission to the hospital (P < 0.05 to P < 0.01).Pearson correlation analysis found that the patient's blood pressure and blood glucose level were the key factors affecting the occurrence of acute cerebral infarction(r=0.768, 0.559).The treatment effect and prognosis of patients with acute cerebral infarction were closely related to the waiting time and treatment methods for treatment.The changes of NIHSS score of patients in group A at 7 days after treatment, and at 24 hours after treatment and 7 days after treatment in group B were tightly related to the length of waiting time for treatment, i.e.the improvement of NIHSS score was more obvious with shorter waiting time for treatment (P < 0.05).There was no significant correlation between the changes of NIHSS score of patients in group A and the waiting time for treatment at 24 h after treatment (P>0.05), while which in group B had different degrees of improvement.At the same time, the improvement of the patient's Barthel score was more obvious with shorter the waiting time for thrombolysis (P < 0.01).At 24 h and 7 d after receiving treatment, the improvement of NIHSS score and Barthel score of patients in group B was more obvious than that in group A(P < 0.01). ConclusionsThe better the recovery of patients with acute cerebral infarction can be obtained with shorter time from onset to thrombectomy.Intravenous thrombolysis combined with interventional thrombectomy has better recovery effect for patients with acute cerebral infarction than intravenous thrombectomy alone. -
Key words:
- acute cerebral infarction /
- thrombolysis /
- interventional thrombectomy
-
表 1 2组病人一般资料(x±s)
项目 A组(n=17) B组(n=16) t P 年龄/岁 71.94±8.42 65.81±13.56 1.57 >0.05 性别(男) 11(64.7) 7(43.8) 1.46# >0.05 吸烟史 10(58.8) 10(62.5) 0.05# >0.05 血压/mmHg 154.59±11.52 150.6±8.19 1.14 >0.05 血糖/(mmol/L) 7.21±2.01 6.17±1.79 1.57 >0.05 TG/(mmol/L) 1.22±0.62 1.25±0.64 0.15 >0.05 TC/(mmol/L) 5.31±1.31 5.54±1.38 0.50 >0.05 LDL-C/(mmol/L) 2.35±0.53 2.05±0.37 1.89 >0.05 FDP/(mg/L) 3.75±1.87 4.96±2.24 1.70 >0.05 D-二聚体/(mg/L) 1.82±1.72 2.85±1.90 1.64 >0.05 FIB/(g/L) 3.15±0.99 3.24±1.18 0.23 >0.05 入院时NIHSS评分/分 15.53±5.50 16.00±4.95 0.26 >0.05 入院时Barthel评分/分 14.42±15.99 17.81±21.29 0.52 >0.05 溶栓等待时间/h 2.82±0.73 2.50±0.98 1.08 >0.05 #示χ2值。TG:三酰甘油;LDL-C:低密度脂蛋白;FDP:纤维蛋白原降解产物;FIB:纤维蛋白原  下载: 导出CSV
下载: 导出CSV
表 2 急性脑梗死病人NIHSS评分与可控性危险因素的相关性
危险因素 病人入院时NIHSS评分 r p 吸烟史 0.388 <0.05 血压 0.768 <0.01 血糖 0.559 <0.01 TG 0.220 >0.05 TC 0.644 <0.01 LDL-C -0.258 >0.05 FDP 0.521 <0.01 D二聚体 0.641 <0.01 FIB 0.191 >0.05
下载: 导出CSV
表 3 2组溶栓时间窗对NIHSS评分和Barthel评分的影响(x±s)
分组 n ≤2 h >2 h t P 治疗后NIHSS评分差值 治疗24 h后 A组 17 0.67±0.52 0.45±0.52 0.80 >0.05 B组 16 5.44±2.07 3.14±1.46 2.49 <0.05 t — 5.48 4.55 — — P — <0.01 <0.01 — — 治疗7 d后 A组 17 6.67±3.20 0.91±2.81 3.85 <0.01 B组 16 10.22±2.73 6.43±1.90 3.12 <0.01 t — 2.31 4.55 — — P — <0.05 <0.01 — — 治疗7 d后Barthel评分差值 A组 17 15.83±11.58 2.50±2.64 3.57 <0.01 B组 16 42.22±21.08 8.57±8.02 3.98 <0.01 t — 2.78 2.25 — — P — <0.01 <0.05 — —
下载: 导出CSV
-
[1] LIU L, WANG D, WONG KS, et al. Stroke and stroke care in China: huge burden, significant workload, and a national priority[J]. Stroke, 2011, 42: 3651. doi: 10.1161/STROKEAHA.111.635755 [2] KURIAKOSE DJ, XIAO ZC. Pathophysiology and treatment of stroke: Present status and future perspectives[J]. Int J Mol Sci, 2020, 21(20): 7609. doi: 10.3390/ijms21207609 [3] MOZAFFARIAN D, BENJAMIN EJ, GO AS, et al. Executive Summary: Heart Disease and Stroke Statistics 2016 Update: A Report From the American Heart Association[J]. Circulation, 2016, 133: 447. doi: 10.1161/CIR.0000000000000366 [4] ZHAO XX, YUE CS, MEI Q, et al. The efficiency analysis of thrombolytic rt-PA combined with intravascular interventional therapy in patients with acute basilar artery occlusion[J]. Int J Biol Sci, 2017, 13(1): 57. doi: 10.7150/ijbs.16029 [5] LEES KR, BLUHMKI E, VON KUMMER R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials[J]. Lancet, 2010, 375: 1695. doi: 10.1016/S0140-6736(10)60491-6 [6] REEVES MJ, ARORA S, BRODERICK JP, et al. Acute stroke care in the US: results from 4 pilot prototypes of the Paul Coverdell National Acute Stroke Registry[J]. Stroke, 2005, 36: 1232. doi: 10.1161/01.STR.0000165902.18021.5b [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [8] 中国卒中学会, 中国卒中学会神经介入分会, 中华预防医学会卒中预防与控制专业委员会介入学组. 急性缺血性卒中血管内治疗中国指南2018[J]. 中国卒中杂志, 2018, 13(7): 706. doi: 10.3969/j.issn.1673-5765.2018.07.014 [9] 彭斌. 急性缺血性脑卒中的诊治[J]. 中华神经科杂志, 2020, 53(2): 122. doi: 10.3760/cma.j.issn.1006-7876.2020.02.009 [10] MICHAEL S PHIPPS, CAROLYN A CRONIN. Management of acute ischemic stroke[J]. BMJ, 2020, 13: 368. [11] 田太伟. 静脉溶栓与介入治疗联合应用于急性脑梗死治疗的效果分析[J]. 母婴世界, 2021(1): 70. [12] 王庆瑞. 静脉溶栓联合介入治疗急性脑梗死的临床疗效[J]. 中国保健营养, 2021, 31(14): 78. [13] ZHAO XX, YUE CS, MEI Q, et al. The efficiency analysis of thrombolytic rt-PA combined with intravascular interventional therapy in patients with acute basilar artery occlusion[J]. Int J Biol Sci, 2017, 13(1): 57. doi: 10.7150/ijbs.16029 [14] ROSSI R, FITZGERALD S, MOLINA S, et al. The administration of rtPA before mechanical thrombectomy in acute ischemic stroke patients is associated with a signifcant reduction of the retrieved clot area but it does not infuence revascularization outcome[J]. J Thromb Thrombolys, 2021, 51(2): 545. doi: 10.1007/s11239-020-02279-1 [15] DENG PP, WU N, CHEN XJ, et al. NIHSS-the Alberta Stroke Program Early CT Score mismatch in guiding thrombolysis in patients with acute ischemic stroke[J]. J Neurol, 2021, 27: 1. doi: 10.1007/s00415-021-10704-5 [16] PATEL RG, MCMULLEN PW. Neuroprotection in the treatment of acute ischemic stroke[J]. Prog Cardiovasc Dis, 2017, 59(6): 542. doi: 10.1016/j.pcad.2017.04.005 -

 点击查看大图
点击查看大图

图(1)表(3)
计量
- 文章访问数: 3089
- HTML全文浏览量: 1546
- PDF下载量: 14
- 被引次数: 0
