


-
卵巢癌是女性生殖系统中最常见的恶性肿瘤,其起病隐匿, 确诊时多已是晚期且预后较差[1],大约90%的病例属于上皮性卵巢癌,最常见的是高级别浆液性癌。与其他恶性肿瘤相同,上皮性卵巢癌的发生是一个将正常细胞推向恶性状态的过程,可能涉及基因突变[2-3]。近年来较多研究指出BRCA1和BRCA2基因是卵巢癌的发病遗传因素[4]。随着近两年卵巢癌维持治疗的新探索,BRCA1/2基因检测变得尤为重要,并且2020年NCCN指南中提出了完善BRCA1/2检测将有益于卵巢癌整个一线治疗模式的选择。但病人的BRCA1/2基因状态与病人的临床病理特征有无密切的联系,需要更进一步探索。本研究收集我院2018年1月至2019年1月就诊的上皮性卵巢癌病人共70例进行BRCA1/2基因检测,查看突变情况,并根据检测结果将病人分为致病突变组和对照组,基于SPSS22.0分析2组病人的临床病理特征有无差异。现作报道。
-
病理确诊为上皮性卵巢癌的病人70例,其中 < 50岁28例,≥50岁42例;临床分期:Ⅰ~Ⅱ期31例,Ⅲ~Ⅳ期39例;病理类型:高级别浆液性乳头状癌44例,非高级别浆液性乳头状癌26例;具有家族遗传性16例,无家族遗传性54例;铂敏感病人59例,铂耐药病人11例。
-
人类BRCA1/2基因突变检测试剂盒(HANDLE System),DNA提取试剂盒(厦门艾德生物医药科技股份有限公司生产)、Illumina测序试剂、普通PCR仪、磁力架、片段分析仪、凝胶电泳系统、核酸定量仪、掌上离心机、漩涡混合仪。
-
采取上皮性卵巢癌病人外周血2 mL,严格按照《DNA提取操作规程》进行DNA分离,分离完毕后按照Qubit.2.0 Fluorometer标准操作规程,对DNA样本的dsDNA浓度进行检测,并记录浓度。
-
首先将引物(厦门艾德生物医药科技股份有限公司生产)涡旋混匀,短暂离心,然后将PCR反应管置于PCR仪上进行扩增,PCR设置体积为50 μL,98 ℃ 30 s预变性,98 ℃ 10 s变性,61 ℃ 10 s退火,72 ℃ 20 s延伸,25个循环,后72 ℃延伸5 min,4 ℃保存。最后运用磁力架对PCR产物进行纯化。
-
首先对纯化后的文库进行浓度质控和质量质控,然后使用illumina公司的Cartridge和Flow cell对文库进行二代测序,使用厦门艾德生物信息分析系统对测序结果进行分析,得到BRCA1基因和BRCA2基因的突变结果,最后对测序结果进行人工复核。
-
采用t′检验和χ2检验。
-
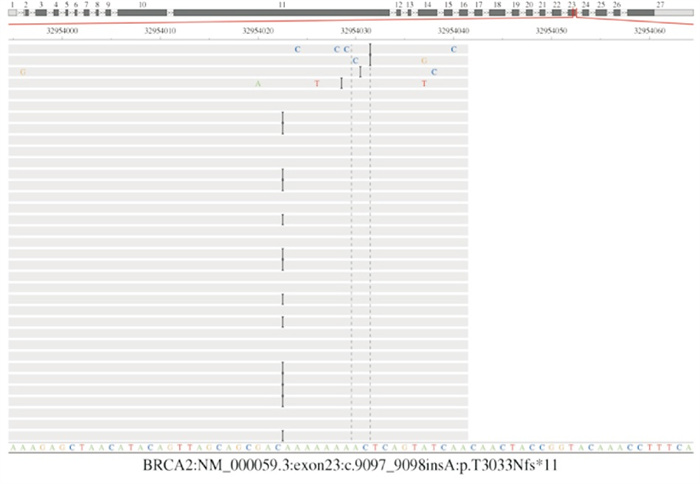
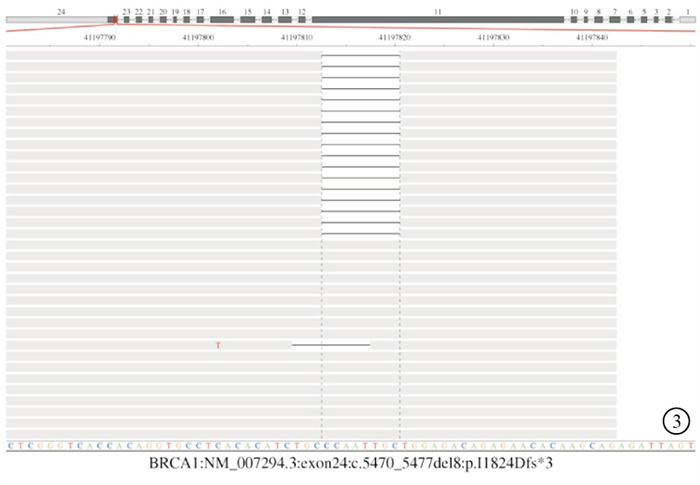
70例上皮性卵巢癌病人中,出现BRCA1/2基因致病性突变的病人共计20例,总占比28.5%。BRCA1突变16例占22.85%(16/70),BRCA2突变4例占5.71%(4/70)。其中移码突变12例,无义突变8例。外显子11突变8例占40%,在BRCA1中11号外显子突变7例,其中2例为981-982位删除AT后出现一个终止密码子,翻译终止(序号6),2例1504-1508位删除TTAAA后,502位的L(亮氨酸)突变为A(丙氨酸),并在突变位点之后2个氨基酸处终止翻译(序号11),1例2138位的C(半胱氨酸)突变为G(丙氨酸),并形成了终止密码,翻译终止(序号11),2例为c.4801A>T的无义突变(序号14)。在BRCA2中11号外显子突变1例,为4065-4068位删除TACC后,1355位的N(天冬氨酸)突变为K(赖氨酸),并在突变位点之后10个氨基酸处终止翻译(序号10)。临床数据表明,在BRCA1/2突变的病人中,BRCA1基因中11号外显子突变频率较高,该外显子或许是一个潜在的突变热点区域。20种BRCA1、BRCA2基因致病突变情况见表 1及图 1~4。
序号 突变位置 碱基序列变化 氨基酸改变 突变类型 例数 1 BRCA1外显子21 c.5503C>T p.R1835* 无义突变 1 2 BRCA2外显子23 c.9097_9098insA p.T3033Nfs*11 移码突变 1 3 BRCA1外显子24 c.5470_5477del8 p.I1824Dfs*3 移码突变 1 4 BRCA1外显子22 c.5353C>T p.Q1785*5 无义突变 1 5 BRCA2外显子24 c.5470_5477del8 p.I1824Dfs*3 移码突变 1 6 BRCA1外显子11 c.981_982delAT p.C328*10 无义突变 2 7 BRCA2外显子14 c.7389_7392delTCAA p.N2463Kfs*3 移码突变 1 8 BRCA1外显子15 c.4503C>A p.C1501* 无义突变 1 9 BRCA1外显子7 c.335delA p.N112Ifs*7 移码突变 2 10 BRCA2外显子11 c.4065_4068delTCAA p.N1355Kfs*10 移码突变 1 11 BRCA1外显子11 c.1504_1508delTTAAA p.L502Afs*2 移码突变 2 12 BRCA1外显子11 c.2138C>G p.S713* 无义突变 1 13 BRCA1外显子24 c.5521delA p.S1841Vfs*2 移码突变 1 14 BRCA1外显子11 c.4801A>T p.K1601* 无义突变 2 15 BRCA1外显子7 c.335delA p.N112Ifs*7 移码突变 2 表 1 20例上皮性卵巢癌病人BRCA1/2基因致病突变情况

图 1 BRCA1外显子11:C.981_ 982delAT: P.C328*无义突变

图 2 BRCA2外显子23 : c.9097_ 9098insA: p.T3033nfs*11移码突变
图 3 BRCA1外显子24:c. 5470_ 5477del8:p.I1824Dfs*3移码突变

图 4 BRCA2外显子14:c.7389_ 7392delTCAA: P.N2463Kfs*3移码突变
-
研究结果发现BRCA1/2致病性突变组高级别浆液性乳头状癌发生率、对铂类治疗药物敏感率、有家族史率均高于未突变组(P < 0.05~P < 0.01),2组年龄和临床分期比较差异无统计学意义(P>0.05)(见表 2)。
临床病理特征 n BRCA1/2突变(n=20) BRCA1/2未突变(n=50) χ2 P 年龄(x±s)/岁 70 50.25±7.11 52.08±11.16 0.82* >0.05 病理类型 高浆
非高浆44
2618
226
248.84 < 0.01 铂类药物 敏感
耐药59
1113
746
45.96 < 0.05 家族史 有
无16
549
117
436.13 < 0.05 临床分期 Ⅰ~Ⅱ
Ⅲ~Ⅳ31
397
1324
260.98 >0.05 *示t′值 表 2 BRCA1/2致病变异与未变异病人临床病理特征的比较
-
1990年和1994年,研究者先后发现了2种与乳腺癌存在密切相关性的基因。这两种基因,根据发现的先后,分别命名为乳腺癌1号和2号基因,即本文研究的BRCA1/2;2种基因均属于抑癌基因,其编码的蛋白通过同源重组通路参与DNA双链损伤的修复,控制DNA损伤应答、调节DNA转录和染色体重组以诱发凋亡等方式从而抑制肿瘤[5-6]。当2种基因发生突变,它们会产生无效蛋白,导致细胞发生变性及恶化。
在与此基因突变的相关人群当中,其罹患卵巢癌的风险明显增加。正常妇女罹患卵巢癌的风险为1.4%,BRCA1基因突变携带者到70岁时发生卵巢癌的机率为40%~60%, BRCA2基因携带者的概率为10%~20%[7]。卵巢癌的传统治疗模式为手术、化疗、复发、再治疗、再复发,最后多线治疗直至病人死亡。超过80%的晚期卵巢癌病人在经过一线治疗后会复发,且每次复发后,病人的疾病无进展生存时间(progression-free survival,PFS)会不断缩短[8]。卵巢癌病人复发与铂耐药密切相关,化疗缓解至复发的时间越长,再次铂化疗反应率越高[9]。人们在能否延长无铂间期的问题上付出了较多努力,并且提出了癌症的维持治疗[10]。所谓的维持治疗,主要是指癌症病人在通过合理的方式,接受初始治疗以后,相关的症状已经得到一定程度的缓解,但是为了能够进一步抑制其日后复发,而采取的系列维持治疗[11-12]。
经过长期的探索及实验,PARP抑制剂翻开了卵巢癌维持治疗的新篇章。奥拉帕利是全球第一个获批上市的PARP抑制剂[13],著名两大Ⅲ期临床实验SOLO1[14]、SOLO2[15],发现奥拉帕利作为一线及二线维持治疗药物可明显延长BRCA突变的初治及铂敏感复发卵巢癌病人的PFS,降低疾病进展或死亡风险。这两项著名研究的提出为卵巢癌病人的治疗提供了新的方向,但是也指出了PARP抑制剂的准确受益人群依赖BRCA基因检测。PARP抑制剂对BRCA基因突变的上皮性卵巢癌病人表现出了显著的效果,并在2020年NCCN指南中提出了完善BRCA检测将有宜于卵巢癌整个一线治疗模式的选择。
本研究选择蚌埠医学院第一附属医院自2018年1月至2019年1月收治经手术确诊的70例上皮性卵巢癌病人,通过二代测序方法,对每个病人进行BRCA1/2基因检测,了解相关的突变情况。探究病人是否在年龄、临床分期、病理类型、家族遗传性、铂敏感性之间有相关性。结果显示上皮性卵巢癌病人中,BRCA1/2突变占有较高比例,占28.5%,其中BRCA1 16例,BRCA2 4例,提示了对BRCA1/2基因检测可评估罹患卵巢癌风险程度。ROY等[16]指出,BRCA1/2为乳腺癌的易感基因,其最常见的突变类型是无义突变和移码突变,而且会以常染色体显性遗传的方式传给子代;本研究中,20例卵巢癌致病突变病人移码突变12例,无义突变8例,与之研究结果一致。HALL等[17]指出,BRCA1/2在不同人种间突变率及突变位点具有明显差异,本研究中外显子11突变8例,突变率较高占40%,说明11号外显子可能为卵巢癌BRCA1/2基因突变的突变热点。有研究[18]指出,BRCA基因突变的卵巢癌病人普遍比未突变病人年轻,并且与种族有关,犹太女性BRCA突变的可能性是普通人群的10倍。在本研究中,BRCA1/2突变组的年龄普遍低于未突变组,但差异并无统计学意义。YOU等[19]对172例中国上皮性卵巢癌病人的BRCA1/2突变进行检测,研究了BRCA突变状态对中国上皮性卵巢癌病人生存结果的影响。研究中表明与其他病理类型病人相比,高级别浆液性癌病人存在更多的致病性突变,本研究结果与之显示一致,此项结果代表了BRCA1/2突变卵巢癌病人肿瘤的恶性程度及复发风险可能相对较高。但BRCA1/2突变的病人表现出了对铂类药物治疗的敏感性,与PENNINGTON等[20]的研究结果相同,这一结果对卵巢癌的治疗效果评价具有指导作用。另外BRCA1/2卵巢癌病人基因突变与否与病人家族史有关,基因突变的病人具有一定的家族遗传性,通过BRCA检测,能够有效地筛查和评估病人的家族遗传性突变情况。同时,可以对病人家属的卵巢癌的患病风险情况进行评估。随着针对BRCA基因突变病人治疗方法的出现,精准治疗会越来越普及,对所有患有高级别浆液性卵巢癌病人进行基因检测,该人群的治疗效果将会有所改善,因此,了解BRCA状况有助于为治疗决策提供依据。
BRCA1/2基因突变与上皮性卵巢癌病人临床病理特征的关系
Analysis of the relationship between BRCA1/2 gene mutation and clinicopathological characteristics of epithelial ovarian cancer
-
摘要:
目的 探究BRCA1/2突变与上皮性卵巢癌病人的临床病理特征关系。 方法对70例经病理确诊的上皮性卵巢癌病人进行BRCA基因检测,分析卵巢癌病人BRCA1/2突变情况,并分析BRCA1/2基因突变与卵巢癌病人的临床病理特征包括年龄、临床分期、病理类型、家族遗传性、铂类药物敏感性的关系。 结果70例上皮性卵巢癌病人中,20例存在BRCA1/2致病性突变,占28.5%,其中BRCA1 16例,BRCA2 4例;BRCA1/2致病性突变组高级别浆液性乳头状癌发生率、对铂类治疗药物敏感率、有家族史率均高于未突变组(P < 0.05~P < 0.01),2组年龄和临床分期比较差异无统计学意义(P>0.05)。 结论BRCA1/2突变的上皮性卵巢癌病人易复发、恶性程度较高,但对铂类药物敏感,BRC1/2基因突变的上皮性卵巢癌病人具有家族遗传性。 Abstract:ObjectiveTo explore the relationship between BRCA1/2 mutation and clinicopathological features of epithelial ovarian cancer. MethodsThe BRCA gene in 70 patients with epithelial ovarian cancer diagnosed by pathology was detected, the BRCA1/2 mutation was analyzed, and the relationship between BRCA1/2 mutation and clinicopathogical characterloistics of ovarian cancer patients(including age, clinical stage, pathological type, familial inheritance and platinum drug sensitivity) was analyzed. ResultsAmong 70 patients with epithelial ovarian cancer, 20 cases with BRCA1/2 gene mutation were found(accounting for 28.5%), which included 16 cases with BRCA1/2 gene mutation and 4 cases with BRCA2 gene mutation.The incidence rate of high-grade papillary carcinoma, susceptibility to platinum therapy and family history in BRCA1/2 mutation group were higher than those in non-mutation group(P < 0.05 to P < 0.01), but there was no statistical significance in the age and clinical stage between two groups(P>0.05). ConclusionsThe epithelial ovarian cancer with BRCA1/2 mutation is prone to recurrence, high grade malignancy, and sensitive to platinum drugs.The BRCA1/2 gene mutation in epithelial ovarian cancer patients is related to the family genetic history of the patients. -
Key words:
- epithelial ovarian neoplasms /
- BRCA1/2 /
- gene mutation
-
表 1 20例上皮性卵巢癌病人BRCA1/2基因致病突变情况
序号 突变位置 碱基序列变化 氨基酸改变 突变类型 例数 1 BRCA1外显子21 c.5503C>T p.R1835* 无义突变 1 2 BRCA2外显子23 c.9097_9098insA p.T3033Nfs*11 移码突变 1 3 BRCA1外显子24 c.5470_5477del8 p.I1824Dfs*3 移码突变 1 4 BRCA1外显子22 c.5353C>T p.Q1785*5 无义突变 1 5 BRCA2外显子24 c.5470_5477del8 p.I1824Dfs*3 移码突变 1 6 BRCA1外显子11 c.981_982delAT p.C328*10 无义突变 2 7 BRCA2外显子14 c.7389_7392delTCAA p.N2463Kfs*3 移码突变 1 8 BRCA1外显子15 c.4503C>A p.C1501* 无义突变 1 9 BRCA1外显子7 c.335delA p.N112Ifs*7 移码突变 2 10 BRCA2外显子11 c.4065_4068delTCAA p.N1355Kfs*10 移码突变 1 11 BRCA1外显子11 c.1504_1508delTTAAA p.L502Afs*2 移码突变 2 12 BRCA1外显子11 c.2138C>G p.S713* 无义突变 1 13 BRCA1外显子24 c.5521delA p.S1841Vfs*2 移码突变 1 14 BRCA1外显子11 c.4801A>T p.K1601* 无义突变 2 15 BRCA1外显子7 c.335delA p.N112Ifs*7 移码突变 2  下载: 导出CSV
下载: 导出CSV
表 2 BRCA1/2致病变异与未变异病人临床病理特征的比较
临床病理特征 n BRCA1/2突变(n=20) BRCA1/2未突变(n=50) χ2 P 年龄(x±s)/岁 70 50.25±7.11 52.08±11.16 0.82* >0.05 病理类型 高浆
非高浆44
2618
226
248.84 < 0.01 铂类药物 敏感
耐药59
1113
746
45.96 < 0.05 家族史 有
无16
549
117
436.13 < 0.05 临床分期 Ⅰ~Ⅱ
Ⅲ~Ⅳ31
397
1324
260.98 >0.05 *示t′值
下载: 导出CSV
-
[1] 王秀, 刘真, 吴晶晶, 等. 人附睾蛋白4、CA199、LPA在卵巢癌中的表达及与临床病理特征的相关性[J]. 蚌埠医学院学报, 2021, 46(2): 183. [2] STRATTON MR, CAMPBELL PJ, FUTREAL PA. The cancer genome[J]. Nature, 2009, 458(7239): 719. doi: 10.1038/nature07943 [3] STRATTON MR. Exploring the genomes of cancer cells: progress and promise[J]. Science, 2011, 331(6024): 1553. doi: 10.1126/science.1204040 [4] MATSUMOTO K, NISHIMURA M, ONOE T, et al. PARP inhibitors for BRCA wild type ovarian cancer; gene alterations, homologous recombination deficiency and combination therapy[J]. Jpn J Clin Oncol, 2019, 49(8): 703. doi: 10.1093/jjco/hyz090 [5] JIANG X, LI X, LI W, et al. PARP inhibitors in ovarian cancer: Sensitivity prediction and resistance mechanisms[J]. J Cell Mol Med, 2019, 23(4): 2303. doi: 10.1111/jcmm.14133 [6] MADARIAGA A, LHEUREUX S, OZA AM. Tailoring Ovarian Cancer Treatment: Implications of BRCA1/2 Mutations[J]. Cancers (Basel), 2019, 11(3): 416. doi: 10.3390/cancers11030416 [7] 饶阳, 李潇, 徐德欢, 等. 74例上皮性卵巢癌患者BRCA基因突变状况及临床意义分析[J]. 国际妇产科杂志, 2021, 48(3): 351. [8] KORKMAZ T, SEBER S, BASARAN G. Review of the current role of targeted therapies as maintenance therapies in first and second line treatment of epithelial ovarian cancer; In the light of completed trials[J]. Crit Rev Oncol Hematol, 2016, 98: 180. doi: 10.1016/j.critrevonc.2015.10.006 [9] SUSANNA LC, JAMES DB. Evolution of platinum resistance in high-grade serous ovarian cancer. [J]. Lancet Oncol, 2011, 12(12): 1169. doi: 10.1016/S1470-2045(11)70123-1 [10] 中国抗癌协会妇科肿瘤专业委员会. 中国卵巢上皮性癌维持治疗专家共识(2019)[J]. 中国实用妇科与产科杂志, 2019, 35(6): 655. [11] GONZALO HG. Management of relapsed ovarian cancer: a review[J]. Springerplus, 2016, 5(1): 1197. doi: 10.1186/s40064-016-2660-0 [12] SAIRA K, JANE MH, JONATHAN AL, et al. Maintenance therapy in ovarian cancer[J]. Curr Opin Oncol, 2014, 26(5): 521. doi: 10.1097/CCO.0000000000000110 [13] 高庆蕾, 孔北华, 尹如铁, 等. PARP抑制剂治疗复发性卵巢癌专家共识[J]. 现代妇产科进展, 2018, 27(10): 721. [14] KATHLEEN M, NICOLETTA C, GIOVANNI S, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer[J]. N Engl J Med, 2018, 379(26): 2495. doi: 10.1056/NEJMoa1810858 [15] ERIC PL, JONATHAN AL, FREDERIC S, et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial[J]. Lancet Oncol, 2017, 18(9): 1274. doi: 10.1016/S1470-2045(17)30469-2 [16] ROY R, CHUN J, POWELL SN. BRCA1 and BRCA2: different roles in a common pathway of genome proctection[J]. Nat Rev Cancer, 2011, 12(1): 68 [17] HALL MJ, REID JE, BURBIDGE LA, et al. BRCA1 and BRCA2 mutations in women of different ethnicities undergoing testing for hereditary breast-ovarian cancer[J]. Cancer, 2009, 115(10): 2222. doi: 10.1002/cncr.24200 [18] ELISABETE W, JERZY ET. Epidemiology of Patients with Ovarian Cancer with and Without a BRCA1/2 Mutation[J]. Mol Diagn Ther, 2015, 19(6): 351. doi: 10.1007/s40291-015-0168-x [19] YOU Y, LI L, LU J, et al. Germline and somatic BRCA1/2 mutations in 172 Chinese women with epithelial ovarian Cancer[J]. Front Oncol, 2020, 10: 295. doi: 10.3389/fonc.2020.00295 [20] PENNINGTON KP, WALSH T, HARREL MI, et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas[J]. Clin Cancer Res, 2014, 20(3): 764. -

 点击查看大图
点击查看大图

图(4)表(2)
计量
- 文章访问数: 4204
- HTML全文浏览量: 2304
- PDF下载量: 17
- 被引次数: 0
