





-
随着病人对医疗舒适化的要求日益增加,程序化镇静镇痛(procedural sedation and analgesia,PSA)已经成为有创性诊断和治疗操作中缓解焦虑、不适和疼痛的一种应用广泛的麻醉方式[1]。镇静深度和镇痛深度是评价PSA有效性的两个最重要的指标。脑电双频谱指数(bispectral index,BIS)作为监测镇静深度可靠的客观指标,现已普遍用于临床[2]。而由于缺乏有效的测量手段,对于术中镇痛效果的评价往往只能通过评估病人心率、血压等生命体征的变化进行预判,这种方法的灵敏度不高[3]。近几年,越来越多的研究试图通过系统性分析测量疼痛指数(pain index,PI),评估病人术中对伤害性刺激的反应程度,从而指导麻醉过程中镇痛药物的使用[4-5]。然而,PI并非临床中的常规监测项目,目前临床上仍将BIS监测作为评估PSA有效性的主要参考指标[6]。既往研究[7]发现,在一定镇静深度下,疼痛刺激增加可以使BIS值上升。但PI与镇静深度的相关性到底如何,PI是否可以有效评判PSA的有效性尚未见报道。本研究拟通过观察镇静镇痛麻醉中不同时间点PI值与BIS值的变化,分析两者的相关性,探讨PI是否可以作为评估PSA有效性的可行性监测指标。现作报道。
-
本研究经医院医学伦理委员会讨论批准,于术前获取病人知情同意并签署知情同意书。选取美国麻醉医师协会(ASA)分级Ⅰ级或Ⅱ级,择期在PSA下行整形外科手术病人100例。其中男18例,女82例;年龄18~53岁;体质量指数16.9~29.4 kg/m2;ASA分级Ⅰ级95例,ASA分级Ⅱ级5例;手术时间(132.1±27.2)min。排除标准:(1)术前肝肾功能异常;(2)患有严重器质性心肺疾病;(3)术前存在急慢性疼痛(如慢性腰腿痛、偏头痛等),且48 h内服用过镇痛药物;(4)体质量指数≥30 kg/m2;(5)既往麻醉药物过敏史;(6)术前有严重心脏传导阻滞。
-
所有病人术前常规禁食禁饮,均无术前用药。入室后常规连续监测心电图、无创血压、心率、脉搏血氧饱和度,开放静脉通路。使用BIS VISTA监护仪(美国Aspect公司)监测BIS值;使用HXD-I多功能组合式监护仪(北京易飞华通科技开发有限公司)监测PI值。麻醉开始,所有病人给予静脉单次输注咪达唑仑0.04 mg/kg,同时静脉持续输注右美托咪定(负荷剂量1 μg/kg,15 min,后以0.4~0.7 μg·kg-1·h-1静脉持续输注)和瑞芬太尼0.1 μg·kg-1·min-1。待BIS值维持在60~80,外科医生在手术部位注射膨胀液局部麻醉,膨胀液按0.9%氯化钠溶液1000 mL+肾上腺素1 mg +利多卡因400 mg配制。术中调节右美托咪定剂量,维持BIS值60~80。若术中右美托咪定泵注速度已达0.7 μg·kg-1·h-1仍无法获得满意的镇静深度,则静脉注射咪唑安定2毫克/次。手术结束前30 min停止输注右美托咪定,手术结束时停止输注瑞芬太尼。术中持续呼吸循环监测,若脉搏血氧饱和度<90%则予面罩吸氧;出现上呼吸道梗阻时行托下颌处理;若心率 < 50次/分,予阿托品0.3毫克/次静脉注射;若平均动脉压 < 60 mmHg予麻黄碱6毫克/次静脉注射。
-
分别于麻醉开始(T1)、手术开始(T2)、麻醉后30 min(T3)、麻醉后60 min(T4)、停止输注右美托咪定即刻(T5)、手术结束(T6)时记录病人的BIS值与PI值。
-
采用方差分析、q检验和Pearson相关分析。
-
所有病人均顺利完成麻醉和手术;术中、麻醉恢复室中和术后随访期间均未发生严重麻醉相关并发症。
随着局麻开始(T1),术中病人BIS值下降,T2~3时均低于T1(P < 0.05);T4时BIS值较T2~3有所回升(P < 0.05);T5~6时BIS值逐渐上升,均明显高于T1~4(P < 0.01),T6时亦明显高于T5(P < 0.01)(见表 1)。
时点 PI值 BIS值 T1 4.5±3.1 65.8±7.1 T2 3.8±1.6 63.0±8.7* T3 3.5±3.2 62.9±6.7* T4 5.1±3.1#▼▼ 65.8±6.7#▼ T5 6.4±4.2**##▼▼▽▽ 69.8±9.1**##▼▼▽▽ T6 6.8±4.3**##▼▼▽▽ 75.8±8.8**##▼▼▽▽▲▲ F 16.11 38.53 P < 0.01 < 0.01 MS组内 11.358 62.688 q检验:与T1比较*P < 0.05,**P < 0.01;与T2比较#P < 0.05,##P < 0.01;与T3比较▼P < 0.05,▼▼P < 0.01;与T4比较▽▽P < 0.01;与T5比较▲▲P < 0.01 表 1 各时间点BIS值与PI值(x±s)
PI值和BIS各时点变化趋势基本一致。随着局麻开始(T1),T2~3时病人PI值逐渐下降,但与T1时差异无统计学意义(P>0.05);T4时PI值较T2~3升高(P < 0.05和P < 0.01);停止输注右美托咪定后(T5~6)PI值逐渐上升,均明显高于T1~4(P < 0.01)(见表 1)。
-
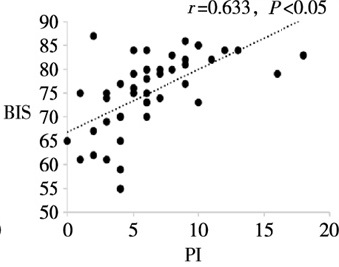
T1~6各时点,PI值与BIS值均呈明显正相关关系(r=0.633~0.798,P < 0.05)(见图 1~6)。
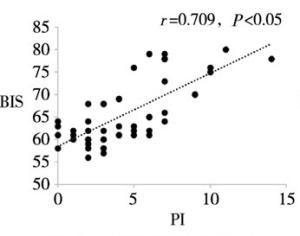
图 1 T1时PI与BIS的相关性
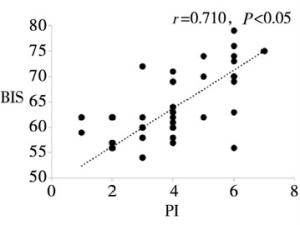
图 2 T2时PI与BIS的相关性
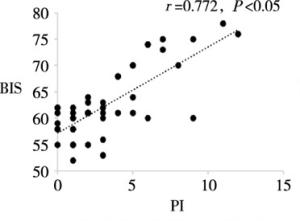
图 3 T3时PI与BIS的相关性
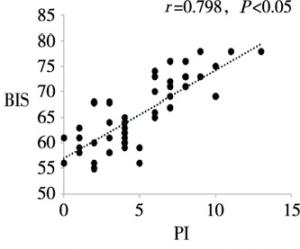
图 4 T4时PI与BIS的相关性
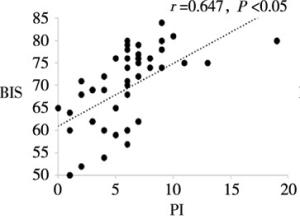
图 5 T5时PI与BIS的相关性
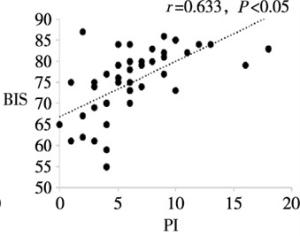
图 6 T6时PI与BIS的相关性
-
PSA关注麻醉方式本身的有效性和安全性[8]。用较完善的监测方式,较早识别出比预期更深的镇静或镇痛程度,可以指导更有效的镇静或镇痛药物的使用,减少不良反应的发生[9]。既往研究[6, 10]中多将BIS值作为PSA有效性常用的监测指标。在本研究发现,镇静镇痛麻醉中PI值与BIS值存在显著相关性,PI值也可以作为PSA有效性的可行性监测指标,在PSA中进一步推广使用,有助于更加全面地评估PSA的有效性。
临床医师和研究者普遍使用一些主观的评估量表如视觉模拟疼痛评分表、数字疼痛评分表、语言疼痛评分表、面部表情疼痛评分表等来评估病人的疼痛程度[11]。通过这些量表,我们可以对病人的疼痛程度做一个粗略的分级。但在某些特殊情况下,例如对于因年龄和精神疾病无法正确主诉的病人、深度镇静下无法进行正常交流的病人,使用这些量表来评价疼痛程度往往行不通或准确性较低。近些年,不少研究开始着手于术中疼痛程度客观量化地评估。例如,瞳孔疼痛指数强度增加的强直性刺激来评估瞳孔的反应性从而评估病人的镇痛程度[4]。镇痛伤害感受指数是利用心率变异性来反映交感张力/副交感张力的平衡,从而评估病人的疼痛水平,在全麻术中得到了有效的应用[12]。本研究中的PI是通过HXD-I多功能定量脑电图监测仪[13]获得的术中疼痛定量的监测指标,类似于BIS值,PI是通过测定和分析脑电图线性成分而转化成的一种简单的量化指标,由我国科研人员运用小波算法通过对脑电信号计算得出的疼痛客观定量评定指标(范围为0~100分)[14]。既往研究[15]中,脑电PI应用于评估临床疼痛程度的有效性已经得到了验证。
早在1990年的研究中就发现,在全身麻醉时通过监测疼痛相关的体觉诱发电位可以反映疼痛刺激的程度[16]。对于疼痛与BIS值之间的关系,研究[17]表明,在丙泊酚镇静下,使用瑞芬太尼与否可以影响病人在疼痛刺激下的BIS值;另外瑞芬太尼可以减轻气管插管后BIS值与平均动脉压的上升,且存在剂量相关性;在疼痛刺激下,BIS值与心血管反应一样可以敏感反映病人的镇痛情况。另一项研究[18]也发现增加瑞芬太尼的剂量可以降低病人的BIS值,研究者认为这可能和瑞芬太尼的镇静作用相关,但目前研究还没有明确瑞芬太尼存在镇静作用。
本研究中,术中采用瑞芬太尼恒速泵注,疼痛刺激来自于手术操作。我们将BIS值控制在60~80之间,保持中度镇静深度[19]。既往研究[20]可以看到,随着镇静镇痛药物的增加,进入深度镇静后,疼痛刺激与BIS值便无明显相关性。所以,现阶段我们所获得脑电PI值与BIS值的相关性仅限于在本研究中PSA的麻醉深度下。
综上所述,在PSA中,脑电PI值与BIS值存在相关性,脑电PI值可作为评价麻醉有效性的可行性的参考指标,有助于优化PSA中镇痛药物的合理使用。
程序化镇静镇痛中脑电疼痛指数与脑电双频谱指数的相关性分析
Correlation analysis between encephlogram pain index and bispectral index during procedural sedation and analgesia
-
摘要:
目的分析和评价程序化镇静镇痛中病人脑电疼痛指数(pain index,PI)与脑电双频谱指数(bispectral index,BIS)的相关性。 方法选择择期在程序化镇静镇痛下施行整形外科手术的病人100例,美国麻醉医师协会(American Society of Anesthesiologists,ASA)分级Ⅰ级或Ⅱ级,年龄18~53岁。麻醉开始给予所有病人静脉单次输注咪达唑仑0.04 mg/kg,同时静脉持续输注右美托咪定(负荷剂量1 μg/kg,后以0.4~0.7 μg·kg-1·h-1静脉持续输注)和瑞芬太尼0.1 μg·kg-1·min-1。待BIS值维持在60~80后,手术部位注射膨胀液局部麻醉。使用BIS VISTA监护仪和HXD-I多功能组合式监护仪分别测量和记录病人在局麻开始(T1)、手术开始(T2)、麻醉后30 min(T3)、麻醉后60 min(T4)、停止输注右美托咪定即刻(T5)、手术结束(T6)各时间点的BIS值和PI值。分析各时间点PI值与BIS的相关性。 结果在T1~T6各时点,PI值与BIS值均呈明显正相关关系(r=0.633~0.798,P < 0.05)。 结论在程序化镇静镇痛中,PI值与BIS值呈明显正相关关系,PI值随着BIS值(镇静的减浅或加深)而上升或下降,表明PI值可作为评估程序化镇静镇痛有效性的良好监测指标。 Abstract:ObjectiveTo analyze and evaluate the correlation between encephlogram pain index(PI) and bispectral index(BIS) during procedural sedation and analgesia. MethodsA total of 100 patients scheduled by plastic surgery under procedural sedation and analgesia, aged 18-53(grade Ⅰ or Ⅱ the American Society of Anesthesiologists were selected.All patients were anesthetized with intravenous injection of single 0.04 mg/kg of midazolam at the beginning of anesthesia, and continuous intravenous infusion of dexmedetomidine(loading dose for 1 μg/kg, followed by 0.4 to 0.7 μg·kg-1·h-1) and remifentanil(0.1 μg·kg-1·min-1) at the same time.After the BIS value was sustained from 60 and 80, the dilating fluid was injected into the surgical site for local anesthesia.The PI and BIS value in all patients were measured and recorded at the beginning of local anesthesia and surgery(T1 and T2), after 30 min and 60 min of anesthesia induction(T3 and T4), immediately after turning off dexmedeto midine infusion(T5) and at the end of surgery(T6) using BIS VISTA monitor and HXD-I multi-function combined monitor, respectively.The correlation between PI and BIS at each time-point was analyzed. ResultsAt the time points of T1-T6, the PI value was significantly positively correlated with BIS value(r=0.633-0.798, P < 0.05). ConclusionsDuring procedural sedation and analgesia, the PI value is significantly correlated with BIS value.The PI value increases or decreases with the increasing and decreasing of BIS value(lightening or deepening of sedation), which suggests that the PI value can be used as a good monitor to assess the effectiveness of procedural sedation and analgesia. -
Key words:
- procedural sedation and analgesia /
- pain index /
- bispectral index
-
表 1 各时间点BIS值与PI值(x±s)
时点 PI值 BIS值 T1 4.5±3.1 65.8±7.1 T2 3.8±1.6 63.0±8.7* T3 3.5±3.2 62.9±6.7* T4 5.1±3.1#▼▼ 65.8±6.7#▼ T5 6.4±4.2**##▼▼▽▽ 69.8±9.1**##▼▼▽▽ T6 6.8±4.3**##▼▼▽▽ 75.8±8.8**##▼▼▽▽▲▲ F 16.11 38.53 P < 0.01 < 0.01 MS组内 11.358 62.688 q检验:与T1比较*P < 0.05,**P < 0.01;与T2比较#P < 0.05,##P < 0.01;与T3比较▼P < 0.05,▼▼P < 0.01;与T4比较▽▽P < 0.01;与T5比较▲▲P < 0.01  下载: 导出CSV
下载: 导出CSV
-
[1] HINKELBEIN J, LAMPERTI M, AKESON J, et al. European Society of Anaesthesiology and European Board of Anaesthesiology guidelines for procedural sedation and analgesia in adults[J]. Eur J Anaesthesiol, 2018, 35(1): 6. doi: 10.1097/EJA.0000000000000683 [2] LEE HC, RYU HG, CHUNG EJ, et al. Prediction of bispectral index during target-controlled infusion of propofol and remifentanil: a deep learning approach[J]. Anesthesiology, 2018, 128(3): 492. doi: 10.1097/ALN.0000000000001892 [3] LUGINBVHL M, YPPÄRILÄ-WOLTERS H, RVFENACHT M, et al. Heart rate variability does not discriminate between different levels of haemodynamic responsiveness during surgical anaesthesia[J]. Br J Anaesth, 2007, 98(6): 728. doi: 10.1093/bja/aem085 [4] SABOURDIN N, DIARRA C, WOLK R, et al. Pupillary pain index changes after a standardized bolus of alfentanil under sevoflurane anesthesia: first evaluation of a new pupillometric index to assess the level of analgesia during general anesthesia[J]. Anesth Analg, 2019, 128(3): 467. doi: 10.1213/ANE.0000000000003681 [5] JULIEN-MARSOLLIER F, RACHDI K, CABALLERO MJ, et al. Evaluation of the analgesia nociception index for monitoring intraoperative analgesia in children[J]. Br J Anaesth, 2018, 121(2): 462. doi: 10.1016/j.bja.2018.03.034 [6] CONWAY A, SUTHERLAND J. Depth of anaesthesia monitoring during procedural sedation and analgesia: a systematic review and meta-analysis[J]. Int J Nurs Stud, 2016, 63: 201. doi: 10.1016/j.ijnurstu.2016.05.004 [7] ISELIN-CHAVES IA, FLAISHON R, SEBEL PS, et al. The effect of the interaction of propofol and alfentanil on recall, loss of consciousness, and the bispectral index[J]. Anesth Analg, 1998, 87(4): 949. doi: 10.1213/00000539-199810000-00038 [8] MENSOUR M, PINEAU R, SAHAI V, et al. Emergency department procedural sedation and analgesia: A Canadian Community Effectiveness and Safety Study (ACCESS)[J]. Can J Anaesth, 2006, 8(2): 94. [9] CONWAY A, SUTHERLAND J. Depth of anaesthesia monitoring during procedural sedation and analgesia: a systematic review protocol[J]. Syst Rev, 2015, 4(1): 1. doi: 10.1186/2046-4053-4-1 [10] AVCI S, BAYRAM B, ĪNANÇ G, et al. Evaluation of the compliance between EEG monitoring (Bispectral IndexTM) and Ramsey Sedation Scale to measure the depth of sedation in the patients who underwent procedural sedation and analgesia in the emergency department[J]. Ulus Travma Acil Cerrahi Derg, 2019, 25(5): 447. [11] FERREIRA-VALENTE MA, PAIS-RIBEIRO JL, JENSEN MP. Validity of four pain intensity rating scales[J]. Pain, 2011, 152(10): 2399. doi: 10.1016/j.pain.2011.07.005 [12] UPTON HD, LUDBROOK GL, WING A, et al. Intraoperative "Analgesia Nociception Index" guided fentanyl administration during sevoflurane anesthesia in lumbar discectomy and laminectomy: a randomized clinical trial[J]. Anesth Analg, 2017, 125(1): 81. doi: 10.1213/ANE.0000000000001984 [13] 陈学新, 马汉祥, 孟尽海, 等. 气管插管和放置喉罩对全麻用药量的影响[J]. 宁夏医学杂志, 2007, 29(12): 1090. doi: 10.3969/j.issn.1001-5949.2007.12.015 [14] 康娜, 吴安石. 脑电疼痛指数评估分娩镇痛产妇疼痛程度的有效性[J]. 临床麻醉学杂志, 2018, 34(4): 391. [15] 王智渊, 顾珏, 曹佳, 等. 脑功能状态仪疼痛指数在患者术后疼痛评估中的应用[J]. 临床麻醉学杂志, 2019, 35(7): 668. [16] KOCHS E, TREEDE RD, AM ESCH JS, et al. Modulation of pain-related somatosensory evoked potentials by general anesthesia[J]. Anesth Analg, 1990, 71(3): 225. [17] GUIGNARD B, MENIGAUX C, DUPONT X, et al. The effect of remifentanil on the bispectral index change and hemodynamic responses after orotracheal intubation[J]. Anesth Analg, 2000, 90(1): 161. doi: 10.1097/00000539-200001000-00034 [18] KOITABASHI T, JOHANSEN JW, SEBEL PS. Remifentanil dose/electroencephalogram bispectral response during combined propofol/regional anesthesia[J]. Anesth Analg, 2002, 94(6): 1530. doi: 10.1213/00000539-200206000-00028 [19] YUE H, HAN J, LIU L, et al. Effect of rocuronium on the bispectral index under anesthesia and tracheal intubation[J]. Exp Ther Med, 2016, 12(6): 3785. doi: 10.3892/etm.2016.3829 [20] ISELIN-CHAVES IA, FLAISHON R, SEBEL PS, et al. The effect of the interaction of propofol and alfentanil on recall, loss of consciousness, and the bispectral index[J]. Anesth Analg, 1998, 87(4): 949. doi: 10.1213/00000539-199810000-00038 -

 点击查看大图
点击查看大图

图(6)表(1)
计量
- 文章访问数: 4604
- HTML全文浏览量: 2593
- PDF下载量: 17
- 被引次数: 0
