


-
重度脊柱侧后凸畸形是指侧凸、后凸Cobb角>90°的脊柱畸形[1-2]。其病理改变复杂,极易合并严重胸廓畸形,严重影响病人肺功能,因而病人手术耐受性差,矫形难度大,并发症多,风险极高。对于重度脊柱侧后凸畸形,目前常用的手术为经椎弓根截骨术(PSO)和后路全脊椎切除术(PVCR)[3]。因PSO截骨量较小而矫形程度有限,PVCR截骨量过大而风险过高[4],故介于二者之间的楔形截骨倍受临床青睐。楔形截骨术是PSO基础上的4级截骨,需切除临近椎间盘和上下终板[5]。已有临床研究[6]表明,经后路楔形截骨术能够有效降低重度脊柱侧后凸畸形病人的术中出血量、神经功能损伤及感染等风险,安全性高,加之其操作简单的优点,是目前临床的优选方案。本研究比较PSO与腰椎后路楔形截骨术治疗重度脊柱侧后凸畸形的临床疗效。现作报道。
-
选取我院2017年8月至2018年6月收治的80例重度脊柱侧后凸畸形病人作为研究对象,其中男47例,女33例,年龄21~77岁。纳入标准:(1)所有病人均经X线片检查诊断为重度脊柱侧后凸畸形;(2)脊髓神经功能损伤Frankle分级≤C级;(3)主弯Cobb角>90°;(4)治疗依从性好并完成12个月随访者。排除标准:(1)合并血液系统疾病者;(2)手术不耐受者;(3)合并严重心、肺等重要脏器功能障碍者。本研究经医院医学伦理委员会审核批准,所有病人及家属均签署研究知情同意书。将病人随机分为观察组和对照组,各40例,观察组男23例,女17例,年龄22~76岁;对照组男24例,女16例,年龄21~77岁,2组性别、年龄等临床资料均具有可比性。
-
2组病人入院后均进行X线片、CT和MRI检查,对其矢状面和冠状面Cobb角进行测量,充分掌握病人脊髓受压程度及是否合并髓内疾病等临床情况。(1)对照组:实施经椎弓根椎体截骨术,具体操作:病人全麻,取俯卧位,在充分暴露拟截骨椎体两侧的椎弓根后,切除小关节突、棘突、分椎板及椎板。然后沿椎弓根外侧骨膜向下剥离至椎体侧缘,将一侧椎体外壁去除后再沿对侧椎弓根对对侧部分椎体进行切除。采用“V”截除椎弓根内壁与椎体后壁,降低病人腰桥高度,闭合间隙并临时固定,然后再处理下一截骨,植骨融合使用切除骨质进行。缝合,常规引流,48 h拔除引流管。(2)观察组:实施腰椎后路楔形截骨术,具体操作:病人全麻,取俯卧位,于术前影像定位的切口位置作正中切口,沿两侧骨膜向下剥离竖脊肌以充分暴露双侧关节突及关节畸形节段,并将相应畸形节段椎板切除。暴露脊髓并将硬脊膜向一侧牵引,然后进行两侧截骨,将椎间盘、骨赘和上下软骨终板切除。畸形椎体充分松解后,以椎体后缘作为支撑点适度撑开,矫形角度确定满意后截骨,暴露松质骨面后植入自体骨或椎间融合器。最后安装预弯固定棒,以双棒交替加压和后路加压固定并矫正脊柱畸形。缝合,常规引流,48 h拔除引流管。
-
麻醉清醒后鼓励病人进行上下肢活动,在耐受疼痛的情况下指导病人进行四肢关节主动活动,包括向上勾脚-锻炼胫前肌和向下蹬脚-锻炼小腿三头肌的踝泵训练,以预防下肢静脉血栓(见图 1A、1B)。第3天开始指导并鼓励病人对股四头肌等进行长收缩运动,逐步进行高抬腿练习(见图 1C)。第5天床旁摄片确定无异常之后,指导病人缓慢摇高床头,使病人处于半卧位进行相关锻炼,然后视病人情况逐步进行仰卧挺腹训练和五点支撑训练以锻炼腰背肌(见图 1D、1E)。7 d后可进行床沿坐位和站位交替训练,10 d后视情况在支护器具辅助下慢步行走训练,视病人耐受程度适当增加运动量,2周后拆线。出院后指导病人及家属,辅助多作四肢运动,但要尽量避免扭躯、弯腰和侧屈等活动,以防脊柱内固定钉棒断裂。同时饮食禁过饱,功能锻炼要适度。支护器具佩戴时间不得少于6个月,同时加强腹肌和背肌训练,以及耸肩和扩胸运动,锻炼平衡肌力。随访12个月。

图 1 男性,54岁,L3重度脊柱侧后凸畸形(1A~1E为病人术后前期康复训练流程)
-
(1) 测量2组病人术前、术后即刻和术后12个月的Cobb角矫正情况;(2)于术前、术后6个月及术后12个月评价Oswestry功能障碍指数(ODI)、日常生活活动能力(ADL)评分。ODI评分:包括疼痛、单项功能、综合功能三个方面共10项,每项0~5分,得分越高说明腰部功能障碍越严重。ADL评分:包括进食、洗澡、穿衣、大便控制、小便控制、如厕、床-椅转移、平地行走及上下楼梯10项,共100分,得分越高说明日常生活活动能力越强。(3)术前和术后12个月对病人脊髓神经功能进行Frankle分级:A级,损伤平面以下感觉和肌肉运动功能完全消失;B级,残留部分感觉功能,随意运动功能消失;C级,感觉功能存在,残留部分无实用价值的运动功能;D级,感觉运动功能存在,但有神经损伤症状和体征;E级,正常。(4)记录手术时间、术中出血量、术后住院时间、平均固定节段数等临床手术指标资料。(5)记录出血过多、椎管狭窄、腰背疼痛加剧等并发症。
-
采用t检验、χ2检验和秩和检验。
-
2组组内术前、术后Cobb角差异均有统计学意义(P <0.01),术后Cobb角明显低于术前(P <0.01);但术前和术后2组间Cobb角差异均无统计学意义(P>0.05)(见表 1)。典型病例:女,23岁,L1先天性脊柱侧后凸畸形,病人Cobb角从术前82°矫正为33°(见图 2)。
分组 n 术前/(°) 术后即刻/(°) 术后12个月/(°) F P MS组内 观察组 40 103.87±25.44 39.34±11.99** 40.05±9.43** 187.20 < 0.01 293.293 对照组 40 104.34±23.09 41.19±13.67** 41.57±10.27** 192.10 < 0.01 275.163 t — 0.09 0.64 0.69 — — — P — > 0.05 > 0.05 > 0.05 — — — q检验:与术前比较** P < 0.01 表 1 2组手术前后的Cobb角比较(x±s)
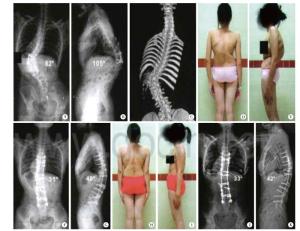
图 2 病人X线全脊柱正位、侧位片
-
2组组内术前、术后ODI和ADL评分差异均有统计意义(P <0.01),2组间术后6个月、12个月的ODI和ADL评分差异均有统计学意义(P <0.05~P <0.01)(见表 2)。
分组 n 术前 术后6个月 术后12个月 F P MS组内 ODI 观察组 40 45.56±13.44 28.78±9.53** 21.02±5.34**## 62.94 < 0.01 99.990 对照组 40 44.99±13.76 34.51±10.13** 26.57±7.49**## 29.43 < 0.01 116.018 t — 0.19 2.61 3.82 — — — P — > 0.05 < 0.05 < 0.01 — — — ADL 观察组 40 35.16±6.42△△ 68.44±6.12**△△ 79.97±10.37**##△△ 348.90 < 0.01 62.069 对照组 40 34.58±7.01△△ 54.26±4.86**△△ 65.77±8.03**##△△ 217.50 < 0.01 45.747 t — 0.39 11.48 6.85 — — — P — > 0.05 < 0.01 < 0.01 — — — 组内比较:△△ P < 0.01。q检验:与术前比较** P < 0.01;与术后6个月比较## P < 0.01 表 2 2组手术前后ODI和ADL评分比较(x±s;分)
-
术前2组间Frankle分级差异无统计学意义(P>0.05),术后12个月2组间Frankle分级差异有统计意义(P <0.01)(见表 3)。
分组 n A级 B级 C级 D级 E级 uc P 术前 观察组
对照组40
408(20.00)
7(17.50)23(57.50)
23(57.50)9(22.50)
10(25.00)0(0.00)
0(0.00)0(0.00)
0(0.00)0.34 > 0.05 术后12个月 观察组
对照组40
400(0.00)
0(0.00)1(2.50)
6(15.00)10(25.00)
19(47.50)17(42.50)
11(27.50)12(30.0)
4(10.00)3.37 < 0.01 观察组组内比较:uc=7.27,P < 0.01;对照组组内比较:uc=5.84,P < 0.01 表 3 2组手术前后Frankle分级比较[n;百分率(%)]
-
观察组术中出血量和术后住院时间均明显低于对照组(P <0.01),2组间手术时间和平均固定节段数差异均无统计学意义(P>0.05)(见表 4)。
分组 术中
出血量/mL术后住院
时间/d手术
时间/min平均固定
节段数/个观察组 2 730.88±423.77 12.55±3.57 270.09±45.29 7.81±1.89 对照组 3 944.66±655.79 19.79±4.33 276.96±47.78 7.13±1.97 t 9.83 8.16 0.66 1.58 P < 0.01 < 0.01 > 0.05 > 0.05 表 4 2组临床手术资料比较(ni=40;x±s)
-
观察组没有出现明显并发症;对照组出现1例腰背疼痛加剧,经对症治疗3 d后缓解,1例出血过多转入ICU,7 d后病情缓解而转入普通病房。
-
对于陈旧性胸腰椎骨折、退行性侧凸等角状后凸畸形且手术耐受差的高创伤矫形手术病人,楔形截骨术有比较大的优势。本研究中Cobb角均从100°左右矫正至40°左右,矫正率超过60%。这与闫煌等[7]报道的结果接近,其矫正率可达68.1%。姜超等[8]得到的术后Cobb角改善率为(59.6±22.05)%,与本研究的结果基本相当。本研究中有一年轻女性病人Cobb角从术前82°矫正为33°,显示了楔形截骨术对重度脊柱侧后凸畸形的良好效果。PSO要对全部椎弓根、棘突、椎板和部分关节突和椎体进行切除,极易破坏脊柱的稳定性和周围血运。腰椎后路楔形截骨术则可有效减少截骨处骨与骨之间的直接接触,可尽量保留椎弓根。因此,腰椎后路楔形截骨术一方面可以通过减少截骨处骨与骨的直接接触而达到保护周围血运的作用,确保截骨术后快速融合,避免失血量过大而导致病人死亡等不良事件[8-9]。另一方面,腰椎后路楔形截骨术对椎弓根的保留能够提供稳定支点,可以减少该水平内固定系统的应力和不稳定,从而降低内固定失败率及连接钉棒系统断裂的概率[10]。而PSO发生连接钉棒系统断裂、椎体脱位、假关节形成的风险极高,有研究[11-12]表明,PSO术后连接钉棒系统断裂和假关节形成的发生率高达32%,直接对截骨处的骨融合产生不良影响。
本研究结果显示,腰椎后路楔形截骨术病人的功能障碍改善和日常生活活动能力提高显著优于行PSO的病人,其原因正是如此。腰椎后路楔形截骨术切除上下椎间盘控制了病人部分椎体活动度,使得椎体中、后柱能够承担大部分应力[6, 13],加之科学有效的术后康复训练,不仅消除了病人康复过程中的悲观、焦虑情绪,而且通过脊柱弹性主动训练、肺功能训练、唤醒试验训练等康复方式保证了手术疗效[14-15],从而改善了病人功能障碍,提高了病人日常生活活动能力。
脊髓神经损伤是手术过程中难以避免的并发症。对于重度脊柱侧后凸畸形来讲,因脊髓长时间处于牵张状态,部分病人术前因脊髓缺血缺氧或受压而早已发生神经功能障碍。在本研究中,术前并发神经功能障碍而Frankle分级为A级者近20%,而术后Frankle分级B级+C级者也高达近30%。这国内外文献报道的0~30.7%基本吻合[16-17]。本研究结果显示,腰椎后路楔形截骨术的神经功能障碍Frankle分级明显优于PSO,显示了更好的手术安全性。根据WANG等[18]的报道,其神经障碍并发症发生率仅为8.7%,低于本研究。究其原因,可能是在手术操作过程中固定钉棒双侧交替矫正时截骨端发生移位,或者是截骨端对合时可能造成脊髓扭曲、褶皱及压迫,抑或是上下位椎板边缘咬除过程中减压不够充分而导致脊髓神经发生机械性压迫。本研究中,腰椎后路楔形截骨术的术中出血量和术后住院时间明显少于PSO。本组中就有1例行PSO的病人发生出血量过大而转入ICU。AKGVL等[19]认为,术中出血量过多不仅会导致术后输血和并发症发生率增高,而且还因为住院时间延长而增加病人家庭经济负担。
综上所述,腰椎后路楔形截骨术创伤小,结合术后康复训练可改善病人腰椎功能和脊髓神经功能障碍,提高病人生活质量。但是,本研究随访时间较短,加之病例数不多,不足以说明腰椎后路楔形截骨术对传统截骨术的长期优势,因此还需要进一步的研究验证。
腰椎后路楔形截骨术治疗重度脊柱侧后凸畸形的疗效分析及术后康复
Curative effect analysis and postoperative rehabilitation of lumbar posterior wedge osteotomy in the treatment of severe scoliosis deformity
-
摘要:
目的分析腰椎后路楔形截骨术对重度脊柱侧后凸畸形的临床疗效及术后康复影响。 方法选取80例重度脊柱侧后凸畸形病人作为研究对象,随机分为观察组和对照组,各40例。对照组实施经椎弓根椎体截骨治疗,观察组实施腰椎后路楔形截骨治疗及术后康复训练。观察2组术前、术后的Cobb角矫正、Oswestry功能障碍指数(ODI)、日常生活活动能力(ADL)评分、脊髓神经功能Frankle分级和并发症发生情况,以及手术时间、术中出血量、术后住院时间、平均固定节段数等临床手术指标资料。 结果2组组内术前、术后Cobb角差异均有统计学意义(P < 0.01),术后Cobb角明显低于术前(P < 0.01);但术前和术后2组间Cobb角差异均无统计学意义(P>0.05)。2组组内术前、术后ODI和ADL评分差异均有统计学意义(P < 0.01),2组间术后6个月、12个月的ODI和ADL评分差异均有统计学意义(P < 0.05~P < 0.01)。术前2组间Frankle分级差异无统计学意义(P>0.05),术后12个月2组间Frankle分级差异有统计学意义(P < 0.01)。观察组术中出血量和术后住院时间均明显低于对照组(P < 0.01),2组间手术时间和平均固定节段数差异均无统计学意义(P>0.05)。 结论腰椎后路楔形截骨术创伤小,结合术后康复训练可改善病人腰椎功能和脊髓神经功能障碍,提高病人生活质量,值得临床推广应用。 Abstract:ObjectiveTo analyze the clinical effects and rehabilitation strategy of posterior wedge osteotomy in the treatment of severe scoliosis deformity. MethodsEighty patients with severe scoliosis were selected and randomly divided into the observation group and control group(40 cases in each group).The observation group was treated with posterior lumbar wedge osteotomy combined with rehabilitation training, and the control group was treated with transpedicular vertebral osteotomy.The Cobb angle correction, Oswestry dysfunction index(ODI), activity of daily living(ADL)score, Frankle grade of spinal nerve function in two groups before and after operation were observed.The operation time, intraoperative bleeding volume, hospital stay after operation, average number of fixed segments and complications were compared between two groups. ResultsThe differences the Cobb angles in two groups between before and after operation were statistically significant(P < 0.01), the Cobb angle in two groups after operation were significantly lower than that before operation(P < 0.01), and the differences the Cobb angles between two groups before and after operation were not statistically significant(P>0.05).The differences the scores of ODI and ADL in two groups between before and after operation were statistically significant(P < 0.01), the differences the scores of ODI and ADL between two groups after 6 and 12 months of operation were statistically significant(P < 0.05 to P < 0.01).The difference of the Frankle grade between two groups before operation was not statistically significant(P>0.05), and the difference of the Frankle grade between two groups after 12 months of operation was statistically significant(P < 0.01).The intraoperative blood loss and postoperative hospital stay in observation group were significantly lower than those in control group(P < 0.01).There was no statistical significance in the operation time and the average number of fixed segments between two groups(P>0.05). ConclusionsThe posterior wedge osteotomy of lumbar spine has less trauma, and which combined with rehabilitation training after operation can improve the lumbar spine function, spinal nerve dysfunction and quality of life of patients, and is worthy of clinical promotion. -
Key words:
- scoliosis deformity /
- wedge osteotomy /
- lumbar posterior approach /
- rehabilitation
-
表 1 2组手术前后的Cobb角比较(x±s)
分组 n 术前/(°) 术后即刻/(°) 术后12个月/(°) F P MS组内 观察组 40 103.87±25.44 39.34±11.99** 40.05±9.43** 187.20 < 0.01 293.293 对照组 40 104.34±23.09 41.19±13.67** 41.57±10.27** 192.10 < 0.01 275.163 t — 0.09 0.64 0.69 — — — P — > 0.05 > 0.05 > 0.05 — — — q检验:与术前比较** P < 0.01  下载: 导出CSV
下载: 导出CSV
表 2 2组手术前后ODI和ADL评分比较(x±s;分)
分组 n 术前 术后6个月 术后12个月 F P MS组内 ODI 观察组 40 45.56±13.44 28.78±9.53** 21.02±5.34**## 62.94 < 0.01 99.990 对照组 40 44.99±13.76 34.51±10.13** 26.57±7.49**## 29.43 < 0.01 116.018 t — 0.19 2.61 3.82 — — — P — > 0.05 < 0.05 < 0.01 — — — ADL 观察组 40 35.16±6.42△△ 68.44±6.12**△△ 79.97±10.37**##△△ 348.90 < 0.01 62.069 对照组 40 34.58±7.01△△ 54.26±4.86**△△ 65.77±8.03**##△△ 217.50 < 0.01 45.747 t — 0.39 11.48 6.85 — — — P — > 0.05 < 0.01 < 0.01 — — — 组内比较:△△ P < 0.01。q检验:与术前比较** P < 0.01;与术后6个月比较## P < 0.01
下载: 导出CSV
表 3 2组手术前后Frankle分级比较[n;百分率(%)]
分组 n A级 B级 C级 D级 E级 uc P 术前 观察组
对照组40
408(20.00)
7(17.50)23(57.50)
23(57.50)9(22.50)
10(25.00)0(0.00)
0(0.00)0(0.00)
0(0.00)0.34 > 0.05 术后12个月 观察组
对照组40
400(0.00)
0(0.00)1(2.50)
6(15.00)10(25.00)
19(47.50)17(42.50)
11(27.50)12(30.0)
4(10.00)3.37 < 0.01 观察组组内比较:uc=7.27,P < 0.01;对照组组内比较:uc=5.84,P < 0.01
下载: 导出CSV
表 4 2组临床手术资料比较(ni=40;x±s)
分组 术中
出血量/mL术后住院
时间/d手术
时间/min平均固定
节段数/个观察组 2 730.88±423.77 12.55±3.57 270.09±45.29 7.81±1.89 对照组 3 944.66±655.79 19.79±4.33 276.96±47.78 7.13±1.97 t 9.83 8.16 0.66 1.58 P < 0.01 < 0.01 > 0.05 > 0.05
下载: 导出CSV
-
[1] 华文彬, 杨操, 郜勇, 等. 顶椎楔形截骨术治疗重度僵硬型脊柱侧后凸畸形[J]. 脊柱外科杂志, 2018, 16(16): 331. [2] 张凡, 孔新兴. 腰椎后路楔形截骨技术治疗重度脊柱侧后凸畸形的效果及对Frankle分级及ADL评分的影响[J]. 临床医学研究与实践, 2019, 4(5): 67. [3] HU W, ZHANG X, YU J, et al. Vertebral column decancellation in Pott's deformity: use of surgimap spine for preoperative surgical planning, retrospective review of 18 patients[J]. BMC Musculos Dis, 2018, 19(1): 223. doi: 10.1186/s12891-018-2156-x [4] HUANG ZF, YANG JF, SUI WY, et al. Surgical outcome comparison of posterior column resection with or without anterior column support in treatment of Yang's Type a severe thoracic spinal deformity[J]. World Neurosurg, 2019, 121(36): e433. [5] URIBE JS, SCHWAB F, MUNDIS GM, et al. The comprehensive anatomical spinal osteotomy and anterior column realignment classification[J]. J Neurosurgery Spine, 2018, 29(5): 565. doi: 10.3171/2018.4.SPINE171206 [6] 张凡, 孔新兴. 腰椎后路楔形截骨术治疗重度脊柱侧后凸畸形的疗效分析[J]. 实用骨科杂志, 2018, 24(12): 1114. [7] 闫煌, 邱勇, 朱泽章, 等. 脊柱截骨矫形技术治疗成人复杂脊柱侧后凸畸形的疗效及安全性的前瞻性观察[J]. 中国脊柱脊髓杂志, 2016, 26(1): 4. doi: 10.3969/j.issn.1004-406X.2016.01.02 [8] 姜超, 王欢, 范波, 等. 经椎间隙楔形截骨技术治疗脊柱侧后凸畸形[J]. 中华骨科杂志, 2017, 37(8): 466. doi: 10.3760/cma.j.issn.0253-2352.2017.08.003 [9] LI C, YANG M, WANG C, et al. Prediction factors predicting intraoperative blood loss in female patients with adolescent idiopathic scoliosis[J]. Medicine(Baltimore), 2015, 94(1): e359. [10] VAN LOON PJ, VAN SG, VAN LOON CJ, et al. A pedicle subtraction osteotomy as an adjunctive tool in the surgical treatment of a rigid thoracolumbar hyperkyphosis: a preliminary report[J]. Spine J, 2016, 6(2): 195. [11] ZHAO X, FAN SW, FANG XQ, et al. Clinical value of oblique lateral interbody fusion in the treatment of adult degenerative scoliosis[J]. Chin J Orthop, 2017, 37(16): 989. [12] TSCHUGG A, KAVAKEBI P, HARTMANN S, et al. Clinical and radiological effect of medialized cortical bone trajectory for lumbar pedicle screw fixation in patients with degenerative lumbar spondylolisthesis: study protocol for a randomized controlled trial(mPACT)[J]. Trials, 2018, 19(1): 129. doi: 10.1186/s13063-018-2504-z [13] 徐韬, 买尔旦·买买提, 郭海龙, 等. 后路经顶椎椎弓根截骨治疗重度僵硬性特发性脊柱侧凸[J]. 中华医学杂志, 2017, 97(15): 1150. doi: 10.3760/cma.j.issn.0376-2491.2017.15.008 [14] SCHWAB F, BLONDEL B, CHAY E, et al. The comprehensive anatomical spinal osteotomy classification[J]. Neurosurgery, 2015, 76(s1): s33. [15] 丁江平, 翁习生, 唐国柱, 等. 重度僵硬性脊柱畸形后路三柱截骨矫形67例疗效及并发症分析[J]. 中国骨与关节杂志, 2020, 9(4): 246. doi: 10.3969/j.issn.2095-252X.2020.04.003 [16] 潘家曌, 孙红, 杨华. 重度僵硬性脊柱侧凸的治疗进展[J]. 世界临床医学, 2019, 13(1): 69. [17] 华文彬, 杨操, 郜勇, 等. 顶椎楔形截骨术治疗重度僵硬型脊柱侧后凸畸形[J]. 脊柱外科杂志, 2018, 16(6): 331. doi: 10.3969/j.issn.1672-2957.2018.06.003 [18] WANG S, AIKENMU K, ZHANG J, et al. The aim of this retrospective study is to evaluate the efficacy and safety of posterior-only vertebral column resection(PVCR)for the treatment of angular and isolated congenital kyphosis[J]. Eur Spine J, 2017, 26(7): 1817. doi: 10.1007/s00586-015-4344-9 [19] HUIREN T, KAI Y, TAO L, et al. Is it possible to correct congenital spinal deformity associated with a tethered cord without prophylactic intradural detethering?[J]. Clin Orthop Relat Res, 2019, 477(7): 1689. doi: 10.1097/CORR.0000000000000652 [20] AKGÜL T, DIKICI F, EKINCI M, et al. The efficacy of cell saver method in the surgical treatment of adolescent idiopathic acoliosis[J]. Acta Orthop Traumatol Turc, 2014, 48(3): 303. doi: 10.3944/AOTT.2014.13.0146 -

 点击查看大图
点击查看大图

图(2)表(4)
计量
- 文章访问数: 2981
- HTML全文浏览量: 1538
- PDF下载量: 4
- 被引次数: 0
