

-
冠心病(CAD)是常见的心血管疾病,以老年群体居多,是导致老年人死亡的重要原因[1]。目前,我国人口老龄化趋势越来越明显,心血管病发病率逐年增高,老年病例的机体脏器处于衰退状态,大多合并多种疾病,用药种类繁多,治疗难度大,而探寻病人预后影响因素能对病人临床治疗进行更好的指导[2]。既往研究[3]指出心血管病的预后与多种因素有关,如认知障碍、衰弱等,其中衰弱属于多维度老年综合征,它能明确病人对应激状态的易损性,且可反映生理功能下降程度。有学者[4]发现,衰弱会增加心血管病病人的再入院率。临床衰弱评分(CFS)是评价病人衰弱程度的重要量表,因考虑到衰弱可能会影响心血管病者的预后,本次研究纳入120例病例进行分析,探讨CFS评分与老年CAD病人短期预后的关系,现作报道。
-
选取我院2019年6-12月收治的老年CAD病人120例,年龄≥65岁,均接受介入治疗,治疗前行CFS评分。其中男68例,女52例,年龄65~86岁,平均(74.49±6.90)岁;体质量指数18~24 kg/m2,平均(21.29±1.35)kg/m2;CAD类型:稳定型心绞痛55例,不稳定型心绞痛42例,心肌梗死23例;病变数量:单支病变79例,双支病变33例,三支病变8例;病变特点:分叉病变91例,三叉病变12例,钙化病变10例,长病变7例;病变部位:左主干13例,回旋支27例,左前降支48例,右冠状动脉32例;介入治疗支架置入数量1~3枚,平均(2.21±0.27)枚;支架总长度15~68 mm,平均(40.38±10.24)mm;合并高脂血症22例,糖尿病31例,高血压27例;有吸烟史者25例。
-
(1) CAD:①经心肌标志物、心电图结合临床症状提示存在异常;②经冠状动脉造影,提示存在至少1支主要冠状动脉血管病变,且血管狭窄超过50%;③存在明显的心绞痛表现,或有陈旧心肌梗死史。(2)冠状动脉病变:根据Gensini积分标准予以评价,狭窄≤25%计1分,狭窄在>25%~50%间计2分,狭窄在>50%~75%间计4分,狭窄在>75%~90%间计8分,狭窄在>90%~ <100%间计16分,狭窄为100%计32分,根据冠状动脉粥样硬化积分之和对病变程度进行评价。
-
(1) 非常健康(1分):具有较强的适应能力,能规律运动,动机明确,且精力旺盛、充沛;(2)健康(2分):不存在活动性疾病,健康程度略微差于完全健康者;(3)合并需干预的疾病(3分):合并不适症状,但临床控制较好;(4)亚健康(4分):行动变缓,未见明显依赖性;(5)轻度衰弱(5分):部分依赖;(6)中度衰弱(6分):大部分依赖于他人;(7)重度衰弱(7分):严重依赖于他人,或疾病进展成终末期。根据CFS评分,将病人分成衰弱组,其中满足(1)(2)(3)(4)项者纳入无衰弱组,将满足(5)(6)(7)者纳入衰弱组。CFS评分 < 5分为无衰弱,5、6、7分分别代表轻度、中度、重度衰弱。
-
纳入标准:(1)年龄≥65岁;(2)诊断满足上述标准;(3)入院前无介入治疗史,入院后行介入治疗;(4)知情同意。排除标准:(1)肾、脑、肺等脏器受损严重;(2)恶性肿瘤;(3)既往有精神病史;(4)拒绝接受衰弱评分;(5)病例资料不完整。
-
术前行双联血小板干预,经桡动脉路径行冠状动脉造影,并实施雷帕霉素药物洗脱支架置入术,给予肝素抗凝处理。观察造影结果,如果左回旋支、左主干、右冠状动脉、左前降支的动脉管腔内径超过50%,则确定为冠状动脉病变。记录支架数量、病变性质、病变血管位置、支架长度等信息。若原支架内狭窄超过50%,或支架两端5 mm内狭窄超过50%,则视为再狭窄。若再狭窄超过75%,并且伴有临床症状,必须再次行血运重建。
-
根据病人的短期(3个月内)预后情况,分成预后良好组和预后不良组,将死亡者、出现严重不良事件者(如泌尿系感染、严重出血等)纳入预后不良组,将无事件生存者纳入预后良好组。比较2组CFS评分,分析CFS评分对短期预后的预测价值。
-
比较预后良好组、预后不良组的CFS评分,并比较衰弱组、无衰弱组的临床特征,包括疾病类型、病变数量、病变特点、病变部位以及是否合并糖尿病、高血压、高脂血症。
-
采用t′检验和χ2检验。绘制受试者工作特征曲线(ROC)分析CFS评分对老年CAD病人短期预后不良的预测价值,确定曲线下面积(AUC)、最佳界值。
-
在120例病人中,有28例(23.33%)预后不良,92(76.67%)例预后良好。在28例预后不良者中,院内死亡4例(14.29%)(其中心力衰弱1例,心源性休克3例),泌尿系感染9例(32.14%),严重出血5例(17.86%),上呼吸道感染10例(35.71%)。
-
预后良好组CFS评分为(4.43±0.86)分低于预后不良组的(6.02±1.61)分,差异有统计学意义(t′=6.83,P <0.01)。
-
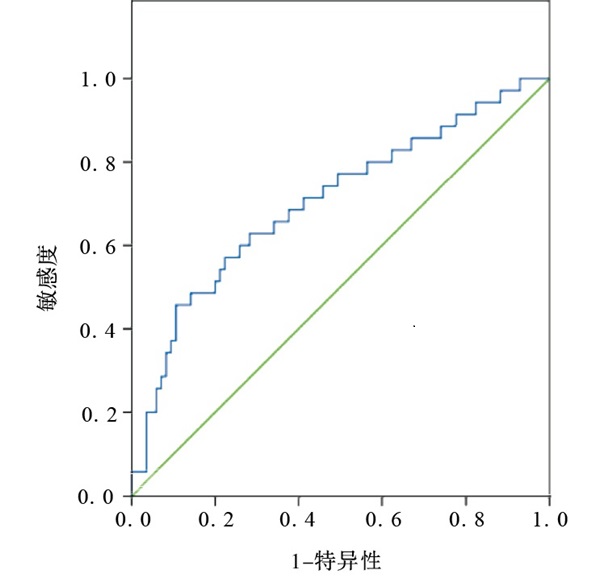
CFS评分预测老年CAD短期预后不良的AUC为0.704(标准误=0.055,P <0.01,95%CI=0.597~0.811),最佳界值为5.475分,敏感度为77.10%,特异度为62.40%。ROC曲线见图 1。
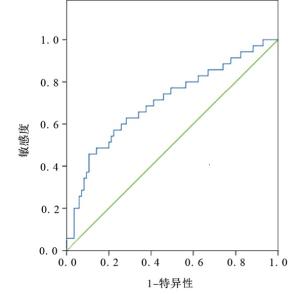
图 1 CFS评分预测老年CAD短期预后不良的ROC曲线
-
通过对病人进行CFS评分,提示无衰弱者79例,衰弱者41例,分别纳入无衰弱组(n=79)和衰弱组(n=41)。2组疾病类型和病变数量分布差异有统计学意义,衰弱组不稳定型心绞痛、双支病变与三支病变占比高于无衰弱组(P <0.01)(见表 1)。
分组 n CAD类型 病变数量 病变特点 稳定型心绞痛 不稳定型心绞痛 心肌梗死 单支病变 双支病变 三支病变 分叉病变 三叉病变 钙化病变 长病变 无衰弱组 79 45(56.96) 20(25.32) 14(17.72) 63(79.75) 14(17.72) 2(2.53) 61(77.22) 7(8.86) 6(7.59) 5(6.33) 衰弱组 41 10(24.39) 22(53.66) 9(21.95) 16(39.02) 19(46.34) 6(14.63) 30(73.17) 5(12.20) 4(9.76) 2(4.88) χ2 — 12.70 20.77 0.61 P — < 0.01 < 0.01 > 0.05 表 1 CFS评分与疾病类型、病变数量、病变特点的关系[n;百分率(%)]
-
衰弱组和无衰弱组病变部位以及高脂血症率、糖尿病率、高血压率、吸烟率差异均无统计学意义(P>0.05)(见表 2)。
分组 n 病变部位 高脂血症 糖尿病 高血压 吸烟史 左主干 回旋支 左前降支 右冠状动脉 有 无 有 无 有 无 是 否 无衰弱组 79 9(11.39) 19(24.05) 32(40.51) 19(24.05) 17(21.52) 62(78.48) 24(30.38) 55(69.62) 21(26.58) 58(73.42) 13(16.46) 66(83.54) 衰弱组 41 4(9.76) 8(19.51) 16(39.02) 13(31.71) 5(12.20) 36(87.80) 7(17.07) 34(82.93) 6(14.63) 35(85.37) 12(29.27) 29(70.73) χ2 — 0.92 1.57 2.49 2.21 2.69 P — > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 表 2 CFS评分与与病变部位及是否合并基础疾病的关系[n;百分率(%)]
-
有学者[7-8]发现,衰弱与CAD存在相同的发病基础,这两类病人均伴有低水平炎症,通过对循环系统内炎症因子表达进行检测,提示白细胞介素6、白细胞介素8等表达均显著上调,此外,单核细胞、中性粒细胞表达也明显增加[7-8]。低水平炎症可促进斑块中脂蛋白激活,并且能下调肌肉质量,引起代谢异常,从而削弱机体对应激源的修复、抵抗能力,导致衰弱[9]。研究[10]表明在稳定型CAD的女性病例中,6年内衰弱发生率为5%~12%,与非衰弱者相比,衰弱者的身体机能明显削弱,生活质量下降。现阶段,临床针对衰弱的评估已有多种方法,但并未形成统一标准。CFS量表具有简短、评分简单等优势,能反映衰弱病人的病理机制、生理机制变化情况,对衰弱的评价有重要意义[11]。
本次结果显示,在120例病例中,短期预后不良率达23.33%,这部分病人可能因病情较重,并发症风险高,逆转难度大所致。通过分析病人的CFS评分,提示与预后良好者比较,不良者的CFS评分更高。通过绘制ROC曲线,发现CFS评分对老年CAD病人短期预后不良有一定预测价值。CFS量表主要用于评价衰弱病人的严重程度,在老年病科中适用[12]。它通过问卷调查的方式对衰弱病情进行分析,可重复性强,容易推广。CFS评分对CAD病例的死亡风险具有预测价值,该量表可分析病人的行动状态,行动状态的变化则能反映活力水平,可用于对多器官系统功能进行评估[13]。本次结果确定了CFS评价病人短期预后不良的最佳界值,提示当CFS评分>5.475分时,预后不良风险更高。因此,临床可将CFS评分作为评估其预后的指标。
通过分析无衰弱者、衰弱者的临床特征,发现与无衰弱者相比,衰弱者的不稳定型心绞痛、双支病变与三支病变占比增高,表明疾病类型、病变数量与CFS评分有关,这间接证实CFS评分能对病人预后进行预测。研究[14]认为衰弱的发生是多种因素作用的结果,如内分泌系统、激素、免疫系统的变化均可能导致衰弱。此外,另有研究[15]提示,疾病类型、病变数量与CAD病人预后密切相关。不稳定心绞痛者发作时症状更剧烈,安静状态下也可发作,而病变数量越多,提示病变越严重,死亡风险更高[16]。
综上,预后不良者的CFS评分较预后良好者明显增高,且CFS评分对老年CAD病人的短期预后有一定预测价值,其评分可能受疾病类型、病变数量的影响。
临床衰弱评分与老年冠心病病人短期预后的关系
The relationship between clinical asthenia scale(CFS) and short-term prognosis of elderly patients with coronary heart disease
-
摘要:
目的探讨临床衰弱评分(CFS)与老年冠心病(CAD)病人短期预后的关系。 方法选取老年CAD病人120例,均接受介入治疗,治疗前行CFS评分。根据病人的短期预后情况,分成预后良好组和预后不良组,将死亡者、出现严重不良事件者纳入预后不良组,将无事件生存者纳入预后良好组。比较2组CFS评分,绘制受试者工作特征曲线(ROC)分析CFS评分对老年CAD病人短期预后不良的预测价值,确定曲线下面积(AUC)、最佳界值。根据CFS评分,将病人分成衰弱组和无衰弱组,分析衰弱与病人临床特征的关系。 结果在120例病人中,有28例(23.33%)预后不良,92例(76.67%)预后良好。在28例预后不良者中,院内死亡4例(14.29%)(其中心力衰弱3例,心源性休克1例),泌尿系感染9例(32.14%),严重出血5例(17.86%)、上呼吸道感染10例(35.71%)。预后良好组CFS评分为(4.13±0.56)分低于预后不良组的(6.02±1.61)分,差异有统计学意义(P < 0.01)。CFS评分预测老年CAD短期预后不良的AUC为0.704(标准误=0.055,P < 0.01,95% CI=0.597~0.811),最佳界值为5.475分。衰弱组和无衰弱组疾病类型和病变数量分布差异有统计学意义,其中衰弱组不稳定型心绞痛、双支病变与三支病变占比高于无衰弱组(P < 0.01)。衰弱组和无衰弱组的病变部位以及高脂血症率、糖尿病率、高血压率、吸烟率差异均无统计学意义(P>0.05)。 结论与短期预后良好者相比,预后不良者的CFS评分明显增高,CFS评分对老年冠心病病人的短期预后具有一定预测价值,且CFS评分可能受冠心病类型、病变数量的影响。 Abstract:ObjectiveTo explore the relationship between clinical asthenia scale(CFS) and short-term prognosis in elderly patients with coronary heart disease(CAD). MethodsOne hundred and twenty elderly CAD patients were treated with intervention, and the CFS scores of the patients before treatment were evaluated.According to the short-term prognosis, the patients were divided into the good prognosis group(survivors without events) and poor prognosis group(death or serious adverse event patients).The CFS score between two groups was compared, and the receiver operating characteristic curve(ROC) was drawn to analyze the predictive value of CFS score for the poor short-term prognosis of elderly CAD patients, and the area under the curve(AUC) and optimal boundary value were determined.According to the CFS score, the patients were divided into the weak group and nonweak group, and the relationship between frailty and patients' clinical characteristics were analyzed. ResultsAmong 120 patients, the prognosis of 28(23.33%)patients were poor, and the prognosis of 92(76.67%) patients were good.Among 28 patients with poor prognosis, 4 cases(14.29%) died in hospital(including 3 cases with heart failure and 1 casewith cardiogenic shock), 9(32.14%) cases were urinary tract infection, 5(17.86%) cases were severe bleeding, and 10(35.71%) cases were upper respiratory tract infection.The CFS score in good prognosis group(4.13±0.56) was significantly lower than that in poor prognosis group(6.02±1.61)(P < 0.01).The AUC of CFS was 0.704(standard error=0.055, P < 0.01, 95% CI=0.597-0.811), and the optimal boundary value was 5.475.The differences of the types of disease and number of lesions between the weak group and nonweak group were statistically significant(P < 0.01), and the proportios of unstable angina pectoris, double-branch lesions and three-branch lesions in weak group were higher than those in nonweak group(P < 0.01).The differences of the lesion site, hyperlipidemia rate, diabetes rate, hypertension rate and smoking rate between weak group and nonweak group were not statistically significant(P>0.05). ConclusionsCompared with the patients with good short-term prognosis, the CFS scores of e patients with poor prognosis significantly increase.The CFS score has a certain predictive value for the short-term prognosis of the elderly patients with CHD, and the CFS score may be affected by the type of CHD and number of lesions. -
Key words:
- coronary heart disease /
- clinical asthenia score /
- prognosis /
- lesion characteristics /
- number of lesion
-
表 1 CFS评分与疾病类型、病变数量、病变特点的关系[n;百分率(%)]
分组 n CAD类型 病变数量 病变特点 稳定型心绞痛 不稳定型心绞痛 心肌梗死 单支病变 双支病变 三支病变 分叉病变 三叉病变 钙化病变 长病变 无衰弱组 79 45(56.96) 20(25.32) 14(17.72) 63(79.75) 14(17.72) 2(2.53) 61(77.22) 7(8.86) 6(7.59) 5(6.33) 衰弱组 41 10(24.39) 22(53.66) 9(21.95) 16(39.02) 19(46.34) 6(14.63) 30(73.17) 5(12.20) 4(9.76) 2(4.88) χ2 — 12.70 20.77 0.61 P — < 0.01 < 0.01 > 0.05  下载: 导出CSV
下载: 导出CSV
表 2 CFS评分与与病变部位及是否合并基础疾病的关系[n;百分率(%)]
分组 n 病变部位 高脂血症 糖尿病 高血压 吸烟史 左主干 回旋支 左前降支 右冠状动脉 有 无 有 无 有 无 是 否 无衰弱组 79 9(11.39) 19(24.05) 32(40.51) 19(24.05) 17(21.52) 62(78.48) 24(30.38) 55(69.62) 21(26.58) 58(73.42) 13(16.46) 66(83.54) 衰弱组 41 4(9.76) 8(19.51) 16(39.02) 13(31.71) 5(12.20) 36(87.80) 7(17.07) 34(82.93) 6(14.63) 35(85.37) 12(29.27) 29(70.73) χ2 — 0.92 1.57 2.49 2.21 2.69 P — > 0.05 > 0.05 > 0.05 > 0.05 > 0.05
下载: 导出CSV
-
[1] 高洁, 王琳, 汪贵清, 等. 缺氧诱导因子-1α基因1772C/T多态性与冠心病患者侧枝循环形成关系的Meta分析[J]. 重庆医学, 2018, 47(12): 1650. doi: 10.3969/j.issn.1671-8348.2018.12.021 [2] MANGIACAPRA F, COLAIORI I, RICOTTINI E, et al. Heart Rate reduction by IVabradine for improvement of ENDothELial function in patients with coronary artery disease: the RIVENDEL study[J]. Clin Res Cardiol, 2016, 106(1): 69. [3] 赵海珍, 孙蕊, 沈犁, 等. 老年心血管疾病住院患者衰弱情况及影响因素研究[J]. 中华现代护理杂志, 2018, 24(33): 3987. doi: 10.3760/cma.j.issn.1674-2907.2018.33.004 [4] 张宁, 朱文玲, 刘晓红, 等. 衰弱与老年患者急性冠状动脉综合征的研究进展[J]. 中华心血管病杂志, 2017, 45(2): 174. doi: 10.3760/cma.j.issn.0253-3758.2017.02.022 [5] 龚洁. 冠心病防治指南[M]. 湖北: 湖北科学技术出版社, 2012: 60. [6] JUNG H, YOO H J, PARK S Y, et al. The Korean version of the FRAIL scale: Clinical feasibility and validity of assessing the frailty status of Korean elderly[J]. Korean J Intern Med, 2015, 31(3): 594. [7] FERRARI R, FOX K. Heart rate reduction in coronary artery disease and heart failure[J]. Nat Rev Cardiol, 2016, 13(8): 493. doi: 10.1038/nrcardio.2016.84 [8] 杨帆, 王双, 覃海, 等. 社区老年人衰弱状态的过渡及其恶化影响因素分析的前瞻性研究[J]. 中华流行病学杂志, 2019, 40(2): 186. doi: 10.3760/cma.j.issn.0254-6450.2019.02.012 [9] 郭朝唤, 侯莉明, 王宁, 等. 西安市某社区老年人群衰弱的相关危险因素分析[J]. 中华老年多器官疾病杂志, 2019, 18(8): 561. [10] 韩雅玲, 王斌. 稳定性冠心病临床治疗策略[J]. 中国实用内科杂志, 2018, 38(1): 1. [11] 杨影红, 曾幸坤, 褚娇娇, 等. 门诊老年患者衰弱现状调查及相关影响因素分析[J]. 浙江医学, 2018, 40(10): 1050. doi: 10.12056/j.issn.1006-2785.2018.40.10.2017-2092 [12] 罗如珍, 杨洋, 张春梅, 等. 社区老年人衰弱水平及影响因素研究[J]. 中国实用护理杂志, 2017, 33(15): 1169. doi: 10.3760/cma.j.issn.1672-7088.2017.15.012 [13] 奚桓, 石婧, 孟丽, 等. 衰弱指数模型在老年人综合评估中的初步应用[J]. 中华流行病学杂志, 2016, 37(5): 718. doi: 10.3760/cma.j.issn.0254-6450.2016.05.027 [14] 陈冲, 郑宝石, 陈绪军, 等. 冠状动脉多支病变合并糖尿病患者临床预后分析[J]. 中国心血管病研究, 2019, 17(1): 48. doi: 10.3969/j.issn.1672-5301.2019.01.011 [15] 雷新宇. 高龄冠心病患者应用经皮冠状动脉介入治疗的预后及影响因素分析[J]. 中国药物与临床, 2019, 19(16): 2787. [16] 刘春霄, 李令娟, 许慧. 老年冠心病患者合并危险因素及冠状动脉病变特点[J]. 中国循证心血管医学杂志, 2016, 8(3): 323. doi: 10.3969/j.issn.1674-4055.2016.03.19 -

 点击查看大图
点击查看大图
图(1)表(2)
计量
- 文章访问数: 3784
- HTML全文浏览量: 1655
- PDF下载量: 14
- 被引次数: 0
