

-
膝前痛(anterior knee pain, AKP)包括髌股关节疼痛综合征在内的多种情况,典型症状是膝关节前的疼痛,下跪、下蹲和跑步等可使髌股关节压力增大的动作会诱发或加重症状[1]。AKP目前主要采用非手术治疗,但保守治疗如非甾体类消炎药、物理疗法、针灸、膝关节矫形器、足弓垫、肌内效贴等方法疗效不佳[2-8],而运动疗法对减轻AKP病人的疼痛有积极作用[9-12]。股四头肌作为髌股关节运动最主要的原动肌,其柔韧性的改善从运动解剖学和生物力学机制上分析,对于改善髌股关节的不良应力和稳定性有重要作用。研究[13]证实,AKP的发生与股四头肌柔韧性不足明显相关。但目前尚无股四头肌拉伸训练对AKP康复效果研究的相关报道。基于此,本研究拟探讨股四头肌拉伸训练对于AKP不同诱发因素的干预效果,以期为AKP病人选择具有针对性的康复训练方案提供参考。现作报道。
-
选择2018年1月至2019年1月于四川省骨科医院门诊就诊的AKP病人42例。其中男24例,女18例;年龄18~44岁;身高150~185 cm;体质量44~90 kg。将病人随机分为观察组和对照组,各21例,2组病人性别、年龄、身高、体质量以及患肢柔韧性具有可比性。
AKP诊断参考《英国运动医学杂志》和《美国运动医学杂志》发表的相关研究[3, 14]中的诊断标准。(1)膝前或者髌后的隐匿性疼痛≥6周;(2)疼痛可由以下至少1种动作诱发:屈膝久坐、跪、下蹲、跑、跳、上/下楼梯、髌骨触诊;(3)排除明确的膝关节结构性(如肌腱、韧带、半月板等)损伤,排除明确诊断的膝关节疾患(如骨折、髌骨脱位或半脱位、退行性骨关节炎等)。
纳入标准:(1)符合上述AKP诊断标准;(2)年龄18~40岁;(3)情绪、心智正常,能配合临床实验;(4)签署知情同意书。排除标准:(1)膝关节手术史;(2)膝关节有积液、肿胀;(3)由髋关节、腰椎或其他骨关节系统伤病引起的下肢的疼痛;(4)合并相关心、肺、肾等严重脏腑病变,无法接受实验方案的其他疾病(如精神病等)。
-
本研究设计为随机、单盲、临床对照试验,治疗前避免向病人透露分组、治疗等相关信息,研究过程中避免向测试人员透露分组、治疗等信息。第一次揭盲时,将样本分配序列号与分组情况记录表进行核对,按不同组将结果资料分类以供分析。数据分析结束后进行第二次揭盲,各组样本分配序列号所记录的治疗措施与分组情况记录表核对,确定观察组和对照组2组,查看分析结果。
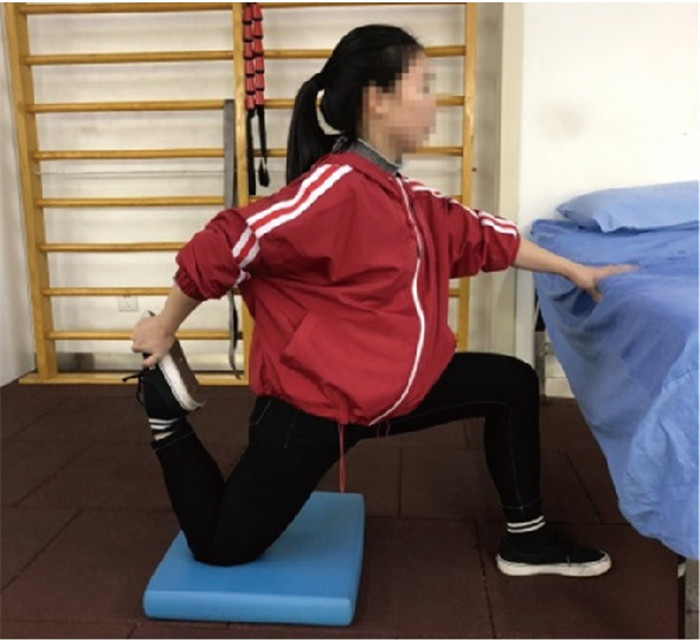
2组病人均于治疗前进行股四头肌柔韧性的测试,均接受门诊常规康复治疗,治疗方案为口服双氯芬酸钠缓释片,每日1片;中医电针治疗每周3次,循经及局部取穴:血海、梁丘、内膝眼、外膝眼、足三里、风市;行针手法:平补平泻。观察组加用弓步跪姿拉伸股四头肌训练,操作方式为保持核心稳定,禁止塌腰;支撑侧腿弓步在前,小腿垂直地面,大腿平行地面;拉伸侧髋关节最大幅度后伸,大腿远端跪贴于软垫上固定,同侧手尽量拉足跟贴近臀部,股四头肌充分拉伸感;均匀呼吸,每组保持30 s,共3组,组间休息30 s(见图 1)。由经过培训的专业治疗师教授动作,嘱病人回家进行每周5次、连续6周的训练。为了保证治疗方案实施质量,建立微信群,要求病人每次训练拍照上传,由专人监督动作完成质量,并记录,要求病人每2周到医院进行一次动作质量检查和改善。

图 1 股四头肌拉伸训练
-
分别在初次治疗前和全部治疗结束后,对病人进行Kujala评分(anterior knee pain scale, AKPS)问卷调查和日常生活、屈膝久坐、上楼梯、下楼梯、下蹲、10 km/h跑步机慢跑动作的疼痛VAS评分。指定一名经过专业培训的测试人员对所有入组病人进行治疗前后的评估测试,测试人员除评估外不参与入组病人、康复治疗等其他试验过程。
-
采用t检验、χ2检验和秩和检验。
-
2组均无提前退出试验者和不良事件发生。2组病人治疗前AKPS评分和各项VAS评分差异均无统计学意义(P>0.05)。治疗后,观察组病人AKPS评分较治疗前升高(P < 0.05),除屈膝久坐VAS评分(P>0.05)外,其他各项VAS评分均较治疗前降低(P < 0.05),而对照组治疗前后各项评分差异均无统计学意义(P>0.05);且治疗后观察组AKPS评分明显高于对照组(P < 0.01),除屈膝久坐VAS评分与对照组差异无统计学意义(P>0.05)外,其他各项VAS评分均明显低于对照组(P < 0.01)(见表 1)。
分组 AKPS 日常VAS 屈膝久坐VAS 上楼梯VAS 下楼梯VAS 下蹲VAS 慢跑VAS 治疗前 对照组 77.76±11.08 2.0(2.0,3.5) 1.0(0.0,1.0) 2.0(0.5,3.0) 3.0(2.0,4.0) 3.0(2.0,3.0) 4.0(3.0,5.0) 观察组 76.67±12.09 3.0(2.0,4.0) 0.0(0.0,2.0) 3.0(2.0,4.0) 3.0(1.0,4.0) 3.0(2.0,4.5) 4.0(3.5,6.0) uc 1.98△ 1.11 0.07 1.38 0.28 1.53 1.72 P >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 治疗后 对照组 78.29±10.91 2.0(1.5,3.0) 0.0(0.0,1.0) 2.0(1.0,3.0) 3.0(2.0,3.5) 3.0(2.0,3.0) 3.0(3.0,4.5) 观察组 84.86±6.51* 1.0(0.0, 1.0)* 0.0(0.0, 0.5) 1.0(0.0, 1.0)* 0.0(0.0, 1.0)* 1.0(0.0, 1.0)* 1.0(0.0, 2.0)* uc 2.37△ 4.11 1.17 3.46 4.58 4.52 4.21 P < 0.01 < 0.01 >0.05 < 0.01 < 0.01 < 0.01 < 0.01 △示t值;组内配对比较*P < 0.05 表 1 2组治疗前后AKPS评分和VAS评分比较(n=12;分)
-
AKPS是量化AKP病人功能障碍的最常用的量表之一,由13个选择题组成,用于衡量AKP病人临床症状和相关功能活动的受限程度。整体评分最低得分为0,表示膝关节症状和功能受限很严重。最高得分为100,表示膝关节既无任何疼痛症状,也没有任何日常功能受限。AKPS用于评价AKP病人膝关节疼痛和功能状况,有很好的信效度,已被广泛用于临床试验。在常用的膝关节评分量表中,AKPS囊括了关于影响AKP病人的常见症状和功能限制的具体问题,所以是可用于评估膝关节特殊运动状况的量表[15]。研究[16]证明,中国病人在心理上能够接受AKPS的中文翻译版本,且其测量结果是可靠和有效的。本研究结果显示,观察组病人治疗后AKPS有明显升高,且治疗后高于对照组,提示拉伸训练可有效改善AKP病人临床症状和相关功能活动受限。
由各种功能活动诱发膝关节疼痛是AKP最主要的病理特征和临床症状,严重影响病人生活质量。目前尚无研究证明非甾体类消炎药对于减轻AKP病人的疼痛症状有效果,且目前关于硫酸氨基葡萄糖和皮质类药物在膝关节内的效果也尚不能确定[14]。中医治疗方面,针对股四头肌扳机点部位的针刺治疗效果亦欠佳[3]。本研究结果表明,对照组病人临床疼痛症状改善效果不佳,而股四头肌拉伸训练对于AKP病人上楼梯、下楼梯、下蹲和慢跑动作诱发的疼痛症状都有较好的缓解作用,观察组病人改善程度大于常规治疗组,但在屈膝久坐疼痛方面,2组病人均无明显改善,可能是由于屈膝久坐是一种静态姿势,对于股四头肌本身功能要求不高,故股四头肌拉伸对于其疼痛症状改善无明显效果,其有效治疗方式还需进一步试验研究。
综上所述,股四头肌拉伸训练对AKP病人疼痛和功能受限有较好改善作用,对于其疼痛常见诱因亦有积极的干预作用,可以作为临床上AKP病人康复治疗的选择。
股四头肌拉伸训练对膝前痛的康复效果
Rehabilitation effects of quadriceps stretch training on anterior knee pain
-
摘要:
目的探讨股四头肌拉伸训练对膝前痛(anterior knee pain,AKP)病人症状和不同诱因的康复作用。 方法选取AKP病人42例,随机分为对照组和观察组,各21例。2组均给予常规康复治疗,观察组加用股四头肌拉伸训练。分别于治疗前后对2组病人进行Kujala评分(anterior knee pain scale,AKPS)和常见功能动作疼痛的VAS评分。 结果2组病人治疗前AKPS评分和日常生活、屈膝久坐、上楼梯、下楼梯、下蹲、慢跑动作的疼痛VAS评分差异均无统计学意义(P>0.05)。治疗6周后,对照组病人AKPS评分和各项VAS评分与治疗前差异均无统计学意义(P>0.05);观察组病人AKPS评分较治疗前升高(P < 0.05),且明显高于对照组治疗后(P < 0.01),除屈膝久坐VAS评分外,其他各项VAS评分均较治疗前降低(P < 0.05),且均明显低于对照组治疗后(P < 0.01)。 结论股四头肌拉伸训练对AKP病人临床疼痛症和功能受限有较好改善效果,对于常见诱因亦有积极的干预作用,可作为临床上AKP病人康复治疗的选择。 Abstract:ObjectiveTo investigate the rehabilitation effects of quadriceps stretch training on symptoms and different incentives of anterior knee pain(AKP). MethodsForty-two patients with AKP were randomly divided into the control group and observation group(21 cases in each group).Two groups were treated with routine rehabilitation method, and the observation group was additionally treated with quadriceps stretch training.The Kujala score(Anterior Knee Pain Scale, AKPS) and VAS scores of common functional movement-induced pain were evaluated before and after treatment. ResultsThe differences of AKPS scores, and pain VAS scores of daily life, knee-bending sedentary, up stairs, down stairs and squatting, jogging movements between two groups were not statistically significant before treatment(P>0.05).The differences of the AKPS scores and VAS scores in control group between before treatment and after 6 weeks of treatment were not statistically significant(P>0.05).After treatment, the AKPS score in the observation group increased compared with before treatment(P < 0.05), and which was significantly higher than that in control group(P < 0.01).Except for the knee-bending sedentary, the other items' scores in observation group after treatment decreased compared with before treatment(P < 0.05), and which was significantly lower than that in control group(P < 0.01). ConclusionsThe quadriceps stretch training has a good effect on the improvement of clinical pain and function limitation in AKP patients, and also has a positive intervention effect on common incentives, so it can be used as the choice of clinical rehabilitation treatment for AKP patients. -
表 1 2组治疗前后AKPS评分和VAS评分比较(n=12;分)
分组 AKPS 日常VAS 屈膝久坐VAS 上楼梯VAS 下楼梯VAS 下蹲VAS 慢跑VAS 治疗前 对照组 77.76±11.08 2.0(2.0,3.5) 1.0(0.0,1.0) 2.0(0.5,3.0) 3.0(2.0,4.0) 3.0(2.0,3.0) 4.0(3.0,5.0) 观察组 76.67±12.09 3.0(2.0,4.0) 0.0(0.0,2.0) 3.0(2.0,4.0) 3.0(1.0,4.0) 3.0(2.0,4.5) 4.0(3.5,6.0) uc 1.98△ 1.11 0.07 1.38 0.28 1.53 1.72 P >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 治疗后 对照组 78.29±10.91 2.0(1.5,3.0) 0.0(0.0,1.0) 2.0(1.0,3.0) 3.0(2.0,3.5) 3.0(2.0,3.0) 3.0(3.0,4.5) 观察组 84.86±6.51* 1.0(0.0, 1.0)* 0.0(0.0, 0.5) 1.0(0.0, 1.0)* 0.0(0.0, 1.0)* 1.0(0.0, 1.0)* 1.0(0.0, 2.0)* uc 2.37△ 4.11 1.17 3.46 4.58 4.52 4.21 P < 0.01 < 0.01 >0.05 < 0.01 < 0.01 < 0.01 < 0.01 △示t值;组内配对比较*P < 0.05  下载: 导出CSV
下载: 导出CSV
-
[1] CROSSLEY KM, STEFANIK JJ, SELFE J, et al. Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures[J]. Br J Sports Med, 2016, 50(14): 839. doi: 10.1136/bjsports-2016-096384 [2] HICKEY A, HOPPER D, HALL T, et al. The effect of the mulligan knee taping technique on patellofemoral pain and lower limb biomechanics[J]. Am J Sports Med, 2016, 44(5): 1179. doi: 10.1177/0363546516629418 [3] SUTLIVE TG, GOLDEN A, KING K, et al. Short-term effects of trigger point dry needling on pain and disability in subjects with patellofemoral pain syndeome[J]. The Int J Sports Physic Ther, 2018, 3(13): 462. [4] DRAPER CE, FREDERICSON M, GOLD GE, et al. Patients with patellofemoral pain exhibit elevated bone metabolic activity at the patellofemoral joint[J]. J Orthop Res, 2012, 30(2): 209. doi: 10.1002/jor.21523 [5] BARTON CJ, LEVINGER P, CROSSLEY KM, et al. The relationship between rearfoot, tibial and hip kinematics in individuals with patellofemoral pain syndrome[J]. Clin Biomech(Bristol, Avon), 2012, 27(7): 702. doi: 10.1016/j.clinbiomech.2012.02.007 [6] BARTON CJ, MENZ HB, LEVINGER P, et al. Greater peak rearfoot eversion predicts foot orthoses efficacy in individuals with patellofemoral pain syndrome[J]. Br J Sports Med, 2011, 45(9): 697. doi: 10.1136/bjsm.2010.077644 [7] COLLINS N, CROSSLEY K, BELLER E, et al. Foot orthoses and physiotherapy in the treatment of patellofemoral pain syndrome: randomised clinical trial[J]. Br J Sports Med, 2009, 43(3): 169. [8] PETERSEN W, ELLERMANN A, GOSELE-KOPPENBURG A, et al. Patellofemoral pain syndrome[J]. Knee Surg Sports Traumatol Arthrosc, 2014, 22(10): 2264. doi: 10.1007/s00167-013-2759-6 [9] KETTUNEN JA, HARILAINEN A, SANDELIN J, et al. Knee arthroscopy and exercise versus exercise only for chronic patellofemoral pain syndrome: a randomized controlled trial[J]. BMC Med, 2007, 13(5): 38. [10] SALTYCHEV M, DUTTON RA, LAIMI K, et al. Effectiveness of conservative treatment for patellofemoral pain syndrome: a systematic review and meta-analysis[J]. J Rehabil Med, 2018, 50(5): 393. doi: 10.2340/16501977-2295 [11] KOOIKER L, VAN DE PORT IG, WEIR A, et al. Effects of physical therapist-guided quadriceps-strengthening exercises for the treatment of patellofemoral pain syndrome: a systematic review[J]. J Orthop Sports Phys Ther, 2014, 44(6): 391. doi: 10.2519/jospt.2014.4127 [12] VAN DER HEIJDEN RA, LANKHORST NE, VAN LINSCHOTEN R, et al. Exercise for treating patellofemoral pain syndrome[J]. Cochrane Database Syst Rev, 2015, 20(1): CD010387. [13] WITVROUW E, LYSENS R, BELLEMANS J, et al. Intrinsic risk factors for the development of anterior knee pain in an athletic population. A two-year prospective study[J]. Am J Sports Med, 2000, 28(4): 480. doi: 10.1177/03635465000280040701 [14] HEINTJES E, BERGER MY, BIERMA-ZEINSTRA SM, et al. Pharmacotherapy for patellofemoral pain syndrome[J]. Cochrane Database Syst Rev, 2004, 2004(3): CD003470. [15] ESCULIER JF, ROY JS, BOUYER LJ. Psychometric evidence of self-reported questionnaires for patellofemoral pain syndrome: a systematic review[J]. Disabil Rehabil, 2013, 35(26): 2181. doi: 10.3109/09638288.2013.774061 [16] CHEUNG RT, NGAI SP, LAM PL, et al. Chinese translation and validation of the Kujala scale for patients with patellofemoral pain[J]. Disabil Rehabil, 2012, 34(6): 510. doi: 10.3109/09638288.2011.610494 -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 3495
- HTML全文浏览量: 1963
- PDF下载量: 5
- 被引次数: 0
