

-
带状疱疹(herpes zoster,HZ)是由长期潜伏于背根神经节的水痘-带状疱疹病毒(varicella zoster virus,VZV)感染复发所引起的,神经根相应皮肤部位会出现皮疹,并引起剧烈的皮肤疼痛[1]。带状疱疹后神经痛(post-herpetic neuralgia,PHN)是HZ常见临床并发症,其特点为皮疹消退后较长一段时间内,皮肤疼痛症状持续存在[2]。HZ病人并发PHN的风险为5%~30%,HZ在老年人中更为常见,且随着年龄的增长,PHN的发病率呈上升趋势[3]。随着人口老龄化的进展,HZ及PHN的发病率均呈上升趋势,PHN的存在则可使HZ的医疗负担进一步加重。此外,PHN可导致发病部位功能障碍,并且严重影响病人的生活质量[4],如何防治PHN是HZ病人亟须解决的问题。慢性病的相关神经性疼痛可能与病人痛苦及灾难性情绪相关[5],本研究通过对HZ病人早期疼痛及心理因素变化情况与PHN的相关性进行分析,为后续进一步疼痛干预提供参考。
-
将2018年6月至2019年6月就诊于我院住院治疗的377例带状疱疹病人纳入研究,诊断标准参照《带状疱疹中国专家共识》[6]。纳入标准:(1)诊断明确的带状疱疹病人;(2)在发病14 d内就诊;(3)就诊前未接受治疗的病人。排除标准:(1)合并严重精神系统疾病,不能配合研究者;(2)孕妇及哺乳期妇女。在随访过程中有16例病人失联,按脱落处理,最终351例病人纳入本研究,其中男157例,女204例;年龄50~80岁。
-
查阅相关文献,并结合笔者自身临床经验,采用自拟《带状疱疹后神经痛危险因素问答表》记录病人的年龄、性别、就诊时间、是否出现皮疹前疼痛、疱疹部位、疼痛评分及心理因素评分等相关指标。所有病人入院后均完善常规检查,并根据《带状疱疹中国专家共识》[6]要求积极予抗病毒、营养神经等标准化治疗,对于出现疼痛症状病人予止痛对症治疗。PHN诊断参照标准《带状疱疹后神经痛诊疗中国专家共识》[7]制定,对出院后病人进行为期6个月的随访,统计病人PHN发生情况。根据病人出院后是否合并PHN将其分为PHN组106例及对照组255例。
-
在病人入院次日抽取空腹静脉血,对病人的血脂、白蛋白/球蛋白(A/G)及CD4+/CD8+水平进行检测。
-
采用视觉模拟评分法(VAS)对病人的疼痛进行评分,满分10分,0~2分:舒适,3~4分:轻度不适,5~6分:中度不适,7~8分:重度不适,9~10分:极度不适。
-
(1) 皮肤病生活质量指标(DLQI),是目前国际上应用最广泛的适用于皮肤病病人的调查问卷,分值为0~30分,其中0~1分:无影响;2~5分:轻度影响;6~10分:中度影响;11~20分:重度影响;21~30分:极严重影响。(2)医院用焦虑抑郁量表(HADS),分别针对焦虑(A)及抑郁(D)问题各7题,焦虑及抑郁亚量表的分值0~7分:为无症状;8~10分:存在可疑;11~21分:肯定存在,其中评分是以8分为起点,即包括可疑及有症状者均为阳性。
-
采用χ2检验、t检验、多因素logistic回归分析、受试者工作特征(ROC)曲线和DeLong检验。
-
PHN组病人年龄、患糖尿病及自身免疫性疾病/恶性肿瘤的比例均高于对照组(P < 0.05~P < 0.01),而2组病人的性别、吸烟、饮酒史等指标差异无统计学意义(P>0.05)(见表 1)。
分组 n 年龄(x±s)/岁 男 女 合并基础疾病 吸烟史 饮酒史 高血压 冠心病 糖尿病 呼吸系统疾病 消化系统疾病 血液系统疾病 脑血管疾病 自身免疫性疾病/恶性肿瘤 PHN组 106 71.23±5.94 49(46.23) 57(53.77) 37(34.91) 16(15.09) 57(53.77) 30(28.30) 51(48.11) 35(33.02) 24(22.64) 49(46.23) 71(66.98) 51(48.11) 对照组 255 67.89±4.76 108(42.36) 147(57.64) 10(41.18) 59(23.14) 105(41.18) 79(30.98) 10(42.75) 92(36.08) 82(32.16) 89(34.90) 156(61.18) 128(50.20) χ2 — 5.63* 0.46 1.23 2.94 4.94 0.26 0.87 0.31 2.19 4.07 1.33 0.13 P — < 0.01 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 < 0.05 >0.05 >0.05 *示t值 表 1 2组病人一般资料的比较[n; 百分率(%)]
-
PHN组病人就诊时间、累计面积、VAS、DLQI、HADS焦虑抑郁评分及合并A/G比值及CD4+/CD8+异常比例均明显高于对照组(P < 0.01~P < 0.05),而2组病人的发病部位、疱疹类型等指标差异均无统计学意义(P>0.05)(见表 2)。
分组 n 就诊时间(x±s)/d 发病部位 疱疹类型 受累神经 头面部 胸背部 腰腹部 四肢 寻常型 大疱性 出血型 顿挫型 三叉神经 肋间神经 腰骸丛神经 颈臂丛神经 PHN组 106 4.75±1.02 39(36.79) 40(37.73) 18(16.98) 9(8.49) 69(65.09) 18(16.98) 15(14.15) 4(3.77) 37(34.91) 36(33.96) 24(22.64) 9(8.49) 对照组 255 4.23±0.87 68(26.67) 10(40.78) 61(23.92) 22(8.63) 18(74.12) 31(12.16) 15(5.88) 20(7.84) 79(30.98) 95(38.43) 62(24.31) 19(7.45) χ2 — 4.91* 4.41 0.78 3.34 P — < 0.01 >0.05 >0.05 >0.05 分组 n 累及面积(x±s)/% 发热 实验室指标异常 皮疹前疼痛 VAS(x±s)/分 DLQI(x±s)/分 HADS(x±s)/分 血脂 A/G比值 CD4+/CD8+ PHN组 106 5.23±1.12 78(73.58) 29(27.36) 54(50.94) 52(49.06) 71(66.98) 3.57±1.13 10.77±2.61 16.95±3.48 对照组 255 4.62±1.05 17(68.63) 59(23.14) 101(39.61) 96(37.65) 138(54.12) 2.96±0.78 9.25±2.37 15.01±3.13 χ2 — 4.79* 0.88 0.81 4.24 4.33 5.08 5.89* 5.39* 5.19* P — < 0.01 >0.05 >0.05 < 0.05 < 0.05 < 0.05 < 0.01 < 0.01 < 0.01 *示t值 表 2 2组病人疱疹相关指标的比较[n; 百分率(%)]
-
自变量为带状疱疹后神经痛,因变量为年龄、就诊时间、VAS、DLQI、HADS、自身免疫性疾病/恶性肿瘤、A/G比值、CD4+/CD8+、皮疹前疼痛及皮疹面积;其中年龄、就诊时间、VAS、DLQI、HADS、皮疹前疼痛及皮疹面积为连续变量;糖尿病、自身免疫性疾病/恶性肿瘤、A/G比值、CD4+/CD8+:1=有,0=无。多因素logistic分析结果表明,高龄,就诊时间过长,皮疹面积大及高VAS、DLQI、HADS评分是发生后神经痛的独立危险因素(OR=1.099, 1.438,1.920, 1.266, 1.210, 1.648;P < 0.05~P < 0.01),而无糖尿病则是后神经痛的保护因素(OR=0.101, P < 0.05)(见表 3)。
因素 B SE Waldχ2 P OR 95%CI 年龄 0.094 0.028 11.46 < 0.01 1.099 1.040~1.160 就诊时间 0.363 0.151 5.78 < 0.05 1.438 1.069~1.932 VAS 0.652 0.161 16.49 < 0.01 1.920 1.401~2.630 DLQI 0.236 0.063 14.22 < 0.01 1.266 1.120~1.431 HADS 0.191 0.047 16.64 < 0.01 1.210 1.104~1.326 糖尿病 -2.293 1.061 4.67 < 0.05 0.101 0.013~0.807 自身免疫性疾病/恶性肿瘤 -0.207 0.819 0.06 >0.05 0.813 0.163~4.046 A/G比值 1.282 1.441 0.79 >0.05 3.604 0.214~60.660 CD4+/CD8+ 0.416 1.335 0.10 >0.05 1.516 0.111~20.740 皮疹前疼痛 0.140 0.523 0.07 >0.05 1.150 0.412~3.207 皮疹面积 0.500 0.134 13.88 < 0.01 1.648 1.267~2.144 表 3 影响带状疱疹后神经痛的多因素logistic回归分析:
-
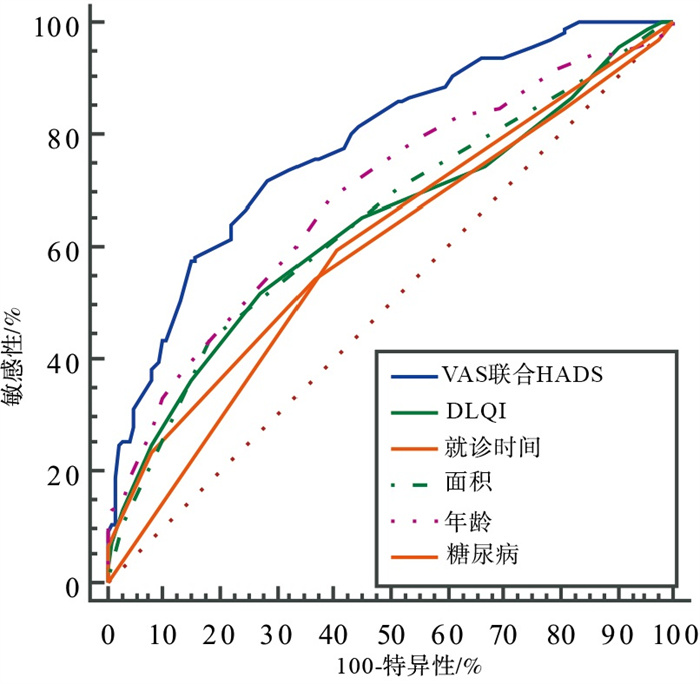
ROC曲线显示,VAS及HADS评分联合预测PHN的诊断效能明显高于单个指标年龄、就诊时间、DLQI评分、糖尿病及皮疹面积的诊断效能(Z=2.35,4.12, 3.06, 5.22,3.18;P < 0.05~P < 0.01)(见图 1和表 4)。
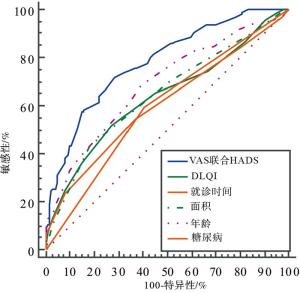
图 1 VAS4及HADS评分联合预测PHN的ROC曲线
变量 AUC SE 95%CI VAS联合HADS 0.780 0.026 5 0.733~0.822 DLQI 0.638 0.033 7 0.586~0.687 就诊时间 0.608 0.032 9 0.556~0.659 皮疹面积 0.855 0.032 0 0.594~0.695 年龄 0.689 0.031 6 0.638~0.736 合并糖尿病 0.595 0.028 5 0.543~0.646 表 4 不同指标预测PHN的ROC分析
-
PHN是带状疱疹病人最常见的并发症,是指疱疹愈合后出现持续1个月及以上的疼痛,HZ中约9%~34%的带状疱疹病人会并发PHN,且PHN的发病率随着年龄的增加而升高,约有65%的60岁及以上病人会出现PHN,而70岁及以上的HZ病人PHN的发病率可达75%[7]。PHN疼痛性质可表现为刀割样、闪电样或烧灼样,疼痛可为持续性,或缓解一段时间后再次出现,PHN病人的病情轻重不一,常伴情感、睡眠障碍,约有45%病人情感受到中-重度影响,出现紧张、焦虑等不良情绪,严重影响病人的生活质量。
PHN的发生机制尚未完全明确,神经可塑性是PHN发生的基础,此外,PHN的发生可能与外周神经敏化、中枢神经敏化、炎性反应及神经元去传入现象等相关。研究[8]表明PHN的高风险因素对于预防PHN尤为关键,目前认为高龄、疼痛程度及皮损严重程度较重是PHN发生的主要危险因素,而关于性别、病程等相关因素是否与PHN相关则存在较大争论[8]。本研究通过对就诊于我院的HZ病人进行分析,结果显示,PHN的发生率为29.36%(101/361),且病人年龄,就诊时间,皮疹面积,疼痛程度,焦虑、抑郁等情绪,生活质量及合并糖尿病均是影响HZ病人发生后神经痛的危险因素。
年龄是目前唯一公认的PHN危险因素,随着年龄增加,机体的免疫功能及应激状态下机体的反应能力随之下降,故高龄病人出现HZ及PHN的风险均会升高,且高龄病人常会合并多种基础疾病,进一步对病人的免疫功能及应激反应造成不良影响,形成恶性循环,故年龄越大,PHN的发生概率越高,且当高龄病人在发生HZ时,其皮损严重程度可能较低龄病人更为重[9]。
HZ急性期产生的疼痛系由周围神经炎性病变及皮肤损伤引起的,VZV在被激活后大量复制,导致神经纤维坏死,进而出现皮疹[10]。当病人的炎症反应越严重时,病人疼痛症状越剧烈,皮损程度越重,出现PHN的风险就越高[11]。本研究结果亦表明PHN病人的皮损面积、疼痛程度等均明显高于非PHN病人。而HZ病人急性期的疼痛症状会对病人的生活及情绪带来负面影响,使病人产生焦虑、抑郁等不良情绪,而不良情绪又会影响病人应对PHN的能力,故病人焦虑、抑郁程度越重,病人发生PHN的风险越高[10]。
糖尿病病人常因常年血糖控制欠佳,出现神经元损伤,当糖尿病病人合并感染VZV时,病毒复制诱发的神经元损伤可能使病人原有的神经损伤进一步加重,此外,血糖升高还会增强多元醇代谢通路的活性,使蛋白激酶C的活性下降,使得神经髓鞘肿胀,进而诱发神经的病变及坏死。且合并糖尿病的病人往往为老年病人,其应激能力、新陈代谢及损伤修复能力均明显下降,故其疼痛时间可能较非糖尿病病人更长,疼痛程度更重,出现PHN的风险更高[12]。
本研究还对病人疼痛及心理因素评分联合诊断PHN的诊断效能进行分析,ROC曲线显示VAS联合HADS预测PHN的曲线下面积明显高于其他指标,且明显高于目前公认的“年龄”这一危险因素,提示病人患病初期的疼痛程度及心理因素变化是PHN发生的主要危险因素,且可有效对PHN的发生进行预测。
此外,PHN的发生还与病人治疗时间相关,早期治疗可有效减少病人神经损伤,促进神经细胞恢复,有利于避免PHN发生,本研究亦证实及时就诊是避免出现PHN的保护因素。目前PHN的治疗尚无特效药物及特殊治疗,故在早期干预病人出现PHN的危险因素在防治PHN方面具有重要意义,而VAS及HADS联合诊断可有效对PHN进行预测,可以在病人早期识别出PHN的高风险人群,及时对其进行心理干预及对症治疗,降低其发生PHN的风险,提高病人预后的生活质量,且VAS及HADS量表简单易行,可供临床广泛使用。
早期疼痛和心理因素变化与带状疱疹后神经痛风险的相关性
Correlation analysis of the early pain and changes of psychological factors with risk of post-herpetic neuralgia
-
摘要:
目的分析带状疱疹病人早期疼痛及心理因素变化情况与带状疱疹后神经痛(PHN)风险的相关性。 方法选择377例带状疱疹病人,根据是否合并PHN分为PHN组及对照组,对病人的就诊时间、疱疹部位及病人入院时疼痛评分及焦虑抑郁评分等相关指标进行比较,采用多因素logistic回归对影响病人PHN的指标进行分析,并采用受试者工作特征曲线对影响PHN相关因素的诊断价值进行比较。 结果PHN组年龄,患糖尿病及自身免疫性疾病/恶性肿瘤的比例,就诊时间,累计面积,视觉模拟评分法(VAS)、皮肤病生活质量指标(DLQI)、焦虑抑郁量表(HADS)评分及合并A/G比值及CD4+/CD8+异常比例均高于对照组(P < 0.05~P < 0.01);而2组病人的性别、吸烟、饮酒史、发病部位及疱疹类型等指标间差异无统计学意义(P>0.05);多因素logistic分析示高龄、就诊时间过长、皮疹面积大及高VAS、DLQI、HADS评分是发生后神经痛的独立危险因素(P < 0.05~P < 0.01),而无糖尿病则是后神经痛的保护因素(P < 0.05);ROC曲线示,VAS及HADS评分联合预测PHN的诊断效能明显高于单独指标年龄、就诊时间、DLQI评分、糖尿病及皮疹面积的诊断效能(P < 0.05~P < 0.01)。 结论带状疱疹病人早期疼痛较重、合并焦虑、抑郁等不良心理因素是导致带状疱疹后神经痛风险独立危险因素,VAS联合HADS评分可有效对PHN进行预测。 Abstract:ObjectiveTo analyze the relationship between the early pain, changes of psychological factors and risk of post-herpetic neuralgia(PHN). MethodsThree hundred and seventy-seven patients with shingles were divided into the PHN group and control group according to whether or not the PHN was merged.The admission time, site of herpes, pain score, anxiety and depression scores were compared between the two groups.The indicators affecting PHN of patients were analyzed using the multivariate logistic regression analysis, and the ROC curve was used to compare the diagnostic value of related factors affecting PHN. ResultsThe age, proportion of diabetes mellitus, autoimmune disease to malignant tumor, visit time, cumulative area, visual analogue scale(VAS) score, dermatology life quality index(DLQI) score, hospital anxiety and depression scale(HADS) score, combined A/G ratio and CD4+/CD8+ abnormality ratio in PHN group were higher than those in control group(P < 0.05 to P < 0.01).There was no statistical significance in gender, smoking history, drinking history, site of disease and type of herpes between the two groups(P>0.05).The results of multivariate logistic analysis showed that the advanced age, long visit time, large rash area, high VAS, DLQI and HADS scores were the independent risk factors of the development of PHN(P < 0.05 to P < 0.01), while the absence of diabetes mellitus was a protective factor of the development of PHN(P < 0.05).The results of ROC curve showed that the diagnostic efficacy of VAS and HADS scores in predicting PHN was significantly higher than that of age, visit time, DLQI score, diabetes mellitus and rash area alone(P < 0.05 to P < 0.01). ConclusionsThe severe early pain, anxiety, depression and other negative psychological factors in patients with herpes zoster are the independent risk factors of the development of PHN, and the VAS combined with HADS score can effectively predict the PHN. -
Key words:
- herpes zoster /
- post-herpetic neuralgia /
- psychological factor /
- correlation analysis
-
表 1 2组病人一般资料的比较[n; 百分率(%)]
分组 n 年龄(x±s)/岁 男 女 合并基础疾病 吸烟史 饮酒史 高血压 冠心病 糖尿病 呼吸系统疾病 消化系统疾病 血液系统疾病 脑血管疾病 自身免疫性疾病/恶性肿瘤 PHN组 106 71.23±5.94 49(46.23) 57(53.77) 37(34.91) 16(15.09) 57(53.77) 30(28.30) 51(48.11) 35(33.02) 24(22.64) 49(46.23) 71(66.98) 51(48.11) 对照组 255 67.89±4.76 108(42.36) 147(57.64) 10(41.18) 59(23.14) 105(41.18) 79(30.98) 10(42.75) 92(36.08) 82(32.16) 89(34.90) 156(61.18) 128(50.20) χ2 — 5.63* 0.46 1.23 2.94 4.94 0.26 0.87 0.31 2.19 4.07 1.33 0.13 P — < 0.01 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 < 0.05 >0.05 >0.05 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 2组病人疱疹相关指标的比较[n; 百分率(%)]
分组 n 就诊时间(x±s)/d 发病部位 疱疹类型 受累神经 头面部 胸背部 腰腹部 四肢 寻常型 大疱性 出血型 顿挫型 三叉神经 肋间神经 腰骸丛神经 颈臂丛神经 PHN组 106 4.75±1.02 39(36.79) 40(37.73) 18(16.98) 9(8.49) 69(65.09) 18(16.98) 15(14.15) 4(3.77) 37(34.91) 36(33.96) 24(22.64) 9(8.49) 对照组 255 4.23±0.87 68(26.67) 10(40.78) 61(23.92) 22(8.63) 18(74.12) 31(12.16) 15(5.88) 20(7.84) 79(30.98) 95(38.43) 62(24.31) 19(7.45) χ2 — 4.91* 4.41 0.78 3.34 P — < 0.01 >0.05 >0.05 >0.05 分组 n 累及面积(x±s)/% 发热 实验室指标异常 皮疹前疼痛 VAS(x±s)/分 DLQI(x±s)/分 HADS(x±s)/分 血脂 A/G比值 CD4+/CD8+ PHN组 106 5.23±1.12 78(73.58) 29(27.36) 54(50.94) 52(49.06) 71(66.98) 3.57±1.13 10.77±2.61 16.95±3.48 对照组 255 4.62±1.05 17(68.63) 59(23.14) 101(39.61) 96(37.65) 138(54.12) 2.96±0.78 9.25±2.37 15.01±3.13 χ2 — 4.79* 0.88 0.81 4.24 4.33 5.08 5.89* 5.39* 5.19* P — < 0.01 >0.05 >0.05 < 0.05 < 0.05 < 0.05 < 0.01 < 0.01 < 0.01 *示t值
下载: 导出CSV
表 3 影响带状疱疹后神经痛的多因素logistic回归分析:
因素 B SE Waldχ2 P OR 95%CI 年龄 0.094 0.028 11.46 < 0.01 1.099 1.040~1.160 就诊时间 0.363 0.151 5.78 < 0.05 1.438 1.069~1.932 VAS 0.652 0.161 16.49 < 0.01 1.920 1.401~2.630 DLQI 0.236 0.063 14.22 < 0.01 1.266 1.120~1.431 HADS 0.191 0.047 16.64 < 0.01 1.210 1.104~1.326 糖尿病 -2.293 1.061 4.67 < 0.05 0.101 0.013~0.807 自身免疫性疾病/恶性肿瘤 -0.207 0.819 0.06 >0.05 0.813 0.163~4.046 A/G比值 1.282 1.441 0.79 >0.05 3.604 0.214~60.660 CD4+/CD8+ 0.416 1.335 0.10 >0.05 1.516 0.111~20.740 皮疹前疼痛 0.140 0.523 0.07 >0.05 1.150 0.412~3.207 皮疹面积 0.500 0.134 13.88 < 0.01 1.648 1.267~2.144
下载: 导出CSV
表 4 不同指标预测PHN的ROC分析
变量 AUC SE 95%CI VAS联合HADS 0.780 0.026 5 0.733~0.822 DLQI 0.638 0.033 7 0.586~0.687 就诊时间 0.608 0.032 9 0.556~0.659 皮疹面积 0.855 0.032 0 0.594~0.695 年龄 0.689 0.031 6 0.638~0.736 合并糖尿病 0.595 0.028 5 0.543~0.646
下载: 导出CSV
-
[1] YANG F, YU S, FAN B, et al. The epidemiology of herpes zoster and postherpetic neuralgia in China: results from a cross-sectional study[J]. Pain Ther, 2019, 8(2): 249. doi: 10.1007/s40122-019-0127-z [2] DEVOR M. Rethinking the causes of pain in herpes zoster and postherpetic neuralgia: the ectopic pacemaker hypothesis[J]. Pain Rep, 2018, 3(6): e702. doi: 10.1097/PR9.0000000000000702 [3] KAWAI K, GEBREMESKEL BG, ACOSTA CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective[J]. BMJ Open, 2014, 4(6): e004833. doi: 10.1136/bmjopen-2014-004833 [4] YU SY, FAN BF, YANG F, et al. Patient and economic burdens of postherpetic neuralgia in China[J]. Clinicoecon Outcomes Res, 2019, 11: 539. doi: 10.2147/CEOR.S203920 [5] RACINE M, MOULIN DE, NIELSON WR, et al. The reciprocal associations between catastrophizing and pain outcomes in patients being treated for neuropathic pain: a cross-lagged panel analysis study[J]. Pain, 2016, 157(9): 1946. doi: 10.1097/j.pain.0000000000000594 [6] 中国医师协会皮肤科医师分会带状疱疹专家共识工作组. 带状疱疹中国专家共识[J]. 中华皮肤科杂志, 2018, 51(6): 403. doi: 10.3760/cma.j.issn.0412-4030.2018.06.001 [7] 带状疱疹后神经痛诊疗共识编写专家组. 带状疱疹后神经痛诊疗中国专家共识[J]. 中国疼痛医学杂志, 2016, 22(3): 161. [8] GILDEN D, WHITE T, KHMELEVA N, et al. Blinded search for varicella zoster virus in giant cell arteritis(GCA)-positive and GCA-negative temporal arteries[J]. J Neurol Sci, 2016, 364: 141. doi: 10.1016/j.jns.2016.03.020 [9] 李玉秋, 徐文英, 潘南楠, 等. 带状疱疹后遗神经痛的危险因素分析[J]. 中国医药, 2019, 14(9): 1406. doi: 10.3760/j.issn.1673-4777.2019.09.031 [10] ITO, SHIN, YASUDA, et al. Clinical courses of herpes simplex virus-induced urethritis in men[J]. J Infect Chemother, 2017, 23(10): 717. doi: 10.1016/j.jiac.2017.03.017 [11] PARKER ZM, PASIEKA TJ, PARKER GA, et al. Immune- and nonimmune-compartment-specific interferon responses are critical determinants of herpes simplex virus-induced generalized infections and acute liver failure[J]. J Virol, 2016, 90(23): 10789. doi: 10.1128/JVI.01473-16 [12] KOGA R, YAMADA K, ISHIKAWA R, et al. Association between treatment-related early changes in psychological factors and development of postherpetic neuralgia[J]. J Anesth, 2019, 33(6): 636. doi: 10.1007/s00540-019-02679-5 -

 点击查看大图
点击查看大图
图(1)表(4)
计量
- 文章访问数: 3617
- HTML全文浏览量: 1931
- PDF下载量: 9
- 被引次数: 0
