


-
急性胰腺炎(acute pancreatitis, AP)是急诊科常见的急危重症,其发病原因是病人体内胰酶蛋白被各种因素激活活化,进而导致胰腺组织出现自身消化现象的炎症性疾病,具有病情严重和疾病发展迅速等特点。目前临床上将AP分为轻度AP(mild acute pancreatitis, MAP)、中度AP(moderately severe acute pancreatitis, MSAP)及重度AP(severe acute pancreatitis, SAP),由于上述不同分级AP病人存在截然不同的临床特点及预后,故准确评估AP病人病情严重程度及预后对于指导治疗有着重要的意义[1-2]。CT严重指数(CT severity index, CTSI)是根据CT扫描检测结果用于评估AP病人病情严重程度的方法,其可有效观察胰腺实质及其周围坏死组织的病理改变,进而有助于评估AP病人的病情严重程度[3],近些年有研究认为改良CT严重指数(modified CT severity index, MCTSI)诊断SAP的敏感性和特异性优于CTSI[4]。抗凝血酶-Ⅲ(antithrombin-Ⅲ, AT-Ⅲ)是一种单链糖蛋白分子,主要由肝细胞、血管内皮细胞分泌和释放,研究发现脓毒血症及SAP病人疾病早期血清AT-Ⅲ表达水平明显下降[5-6]。因此本研究拟探讨血清AT-Ⅲ联合MCTSI在AP病人病情严重程度及预后评估中的价值。
-
选择本院急诊科和普外肝胆科2016年1月至2019年10月收治的124例AP病人作为研究对象,根据病情严重程度分为MAP组(38例)、MSAP组(46例)、SAP组(40例),根据预后不同分为存活组(110例)、死亡组(14例)。MAP组:男26例,女12例,年龄(42.3±12.5)岁,病因为胆源性24例、酒精性10例、其他4例,发病至入院时间为4~12 h;MSAP组:男32例,女14例,年龄(43.0±12.3)岁,病因为胆源性28例、酒精性12例、其他6例,发病至入院时间为5~12 h;SAP组:男28例,女12例,年龄(42.8±12.2)岁,病因为胆源性24例、酒精性11例、其他5例,发病至入院时间为4~11 h。存活组:男76例,女34例,年龄为(43.3±12.7)岁,病因为胆源性67例、酒精性30例、其他13例,发病至入院时间为5~12 h;死亡组:男10例,女4例,年龄(42.4±12.1)岁,病因为胆源性9例、酒精性3例、其他2例,发病至入院时间为4~11 h。各组病人性别、年龄、病因、发病时间等临床资料均具有可比性,本研究方案已通过院伦理委员会批准。
-
纳入标准:(1)所有病人均符合AP诊断标准及疾病分组标准;(2)所有病人入院前未采取任何治疗措施;(3)年龄均>18岁;(4)所有病人或家属已签署知情同意书。排除标准:(1)合并有胰腺或其他脏器组织恶性肿瘤疾病的病人;(2)合并有严重贫血或营养状态不佳的病人;(3)伴随有急慢性感染性疾病的病人;(4)妊娠或哺乳期妇女。
-
所有病人均在入院24 h内采用Philips 64排多层螺旋CT仪器进行检查,平扫检查后通过静脉注射碘造影剂,从膈顶至耻骨联合水平实施多期增强扫描检查,相关参数为:120 kV,100 mA,螺距1.172:1,重建厚度5 mm,层间距5 mm。根据胰腺炎性反应、胰腺组织坏死、胰外并发症等影像学图像形态的严重程度予以MCTSI评分,总分为0~10分,评分分值越高提示病人病情程度越严重。由两名副主任医师进行评分,如评分存在差异则取平均值作为最终评分数值。
-
所有病人入院24 h内在清晨空腹状态时抽取4 mL肘部静脉血液,3 000 r/min离心处理10 min后留取上清液,采用发色底物法检测血清AT-Ⅲ表达水平,试剂盒购自美国BECKMAN COULTER公司,由检验科医生按照说明书进行操作。
-
采用t(或t′)检验、χ2检验、方差分析和q检验。采用ROC曲线分析临床价值。
-
不同病情严重程度AP病人血清AT-Ⅲ水平及MCTSI评分比较差异均有统计学意义(P < 0.01),AP病人随着病情严重程度增加,血清AT-Ⅲ水平降低,而MCTSI评分增加(见表 1)。
分组 n AT-Ⅲ/(mg/L) MCTSI评分/分 MAP组 38 256.75±60.43 3.67±0.74 MSAP组 46 187.31±42.35** 5.05±1.13** SAP组 40 132.62±35.54**△△ 7.22±1.47**△△ F — 68.75 93.82 P — < 0.01 < 0.01 MS组内 — 2 190.786 1.338 q检验:与MAP组比较**P < 0.01;与MSAP组比较△△P < 0.01 表 1 不同病情严重程度AP病人血清AT-Ⅲ水平及MCTSI评分比较(x±s)
-
死亡组病人血清AT-Ⅲ水平低于存活组,而MCTSI评分高于存活组(P < 0.01)(见表 2)。
分组 n AT-Ⅲ/(mg/L) MCTSI评分/分 存活组 110 193.87±73.32 4.76±1.47 死亡组 14 101.15±31.20* 7.93±1.17 t — 8.52 7.75 P — < 0.01 < 0.01 *示t′值 表 2 不同预后AP病人血清AT-Ⅲ水平及MCTSI评分比较(x±s)
-
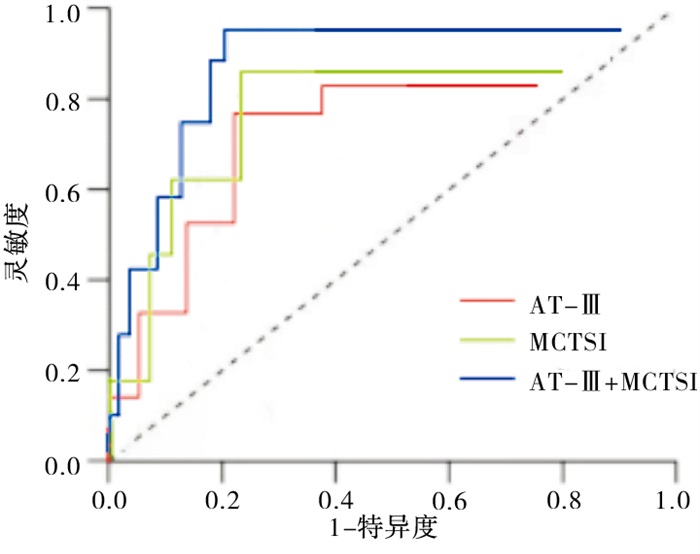
采用ROC曲线分析血清AT-Ⅲ、MCTSI评分单一及联合检测诊断SAP的临床价值,结果显示血清AT-Ⅲ联合MCTSI评分诊断SAP的AUC、敏感度及特异度均优于单一检测(见表 3、图 1)。
指标 截断值 敏感度/% 特异度/% 约登指数 AUC AT-Ⅲ/(mg/L) 150.72 80.0 71.4 0.51 0.782 MCTSI/分 6.05 82.5 76.2 0.59 0.815 AT-Ⅲ+MCTSI — 92.5 85.7 0.78 0.897 表 3 血清AT-Ⅲ联合MCTSI评分诊断SAP的价值分析
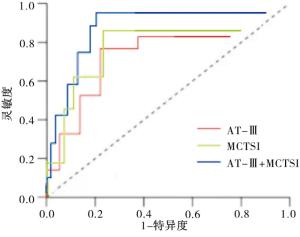
图 1 血清AT-Ⅲ联合MCTSI评分诊断SAP的ROC曲线
-
采用ROC曲线分析血清AT-Ⅲ、MCTSI评分单一及联合检测预测AP病人死亡的临床价值,结果显示血清AT-Ⅲ联合MCTSI评分预测AP病人死亡的AUC、敏感度及特异度均优于单一检测(见表 4及图 2)。
指标 截断值 敏感度/% 特异度/% 约登指数 AUC AT-Ⅲ/(mg/L) 125.84 78.6 70.0 0.49 0.760 MCTSI/分 6.31 85.7 74.5 0.60 0.821 AT-Ⅲ+MCTSI — 92.9 81.8 0.75 0.875 表 4 血清AT-Ⅲ联合MCTSI预测AP病人死亡的价值分析
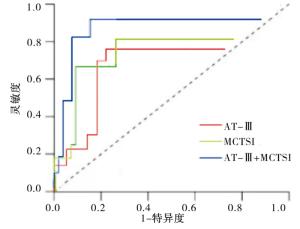
图 2 血清AT-Ⅲ联合MCTSI预测AP病人死亡的ROC曲线
-
AP临床分级是对病人诊治期间胰腺及全身并发症发生、发展情况予以综合判断,进而作出的最终诊断,不同AP分级有着差异性明显的临床特点及预后[7]。如果在疾病早期阶段即准确诊断出AP病人病情严重程度和预测病人预后情况,对于临床诊治指导及改善预后有着重要意义[8-9]。目前医务人员主要根据临床评分系统、影像学评分系统和实验室指标评估AP病人病情严重程度及预后,其中影像学评分系统尤其是CT增强扫描对AP病人具有重要的作用[10]。CTSI是广泛应用于AP诊断的影像学评分系统,其从胰腺炎性反应及胰腺组织坏死影像学图像表现对AP病人病情严重程度予以评估,对病人预后也具有较高的预测价值[11-12]。而MCTSI在CTSI的评分基础上增加对胰外并发症影像学图像表现的评估,可更加准确和全面评估AP病人的病情严重程度及预后[13-14]。本研究显示,不同病情严重程度及预后的AP病人MCTSI评分比较存在明显的差异性(P < 0.01),且随着病情加重和预后不佳MCTSI评分明显升高(P < 0.01),提示MCTSI评分在评估AP病人病情严重程度及预后方面具有重要的临床价值。
SAP起病急骤,进展迅速、死亡率极高,疾病早期阶段常伴随出现多器官功能障碍综合征,难以用胰酶蛋白激活活化和胰腺组织自身消化等发病机制解释,近些年研究认为,SAP与全身炎症反应综合征(systemic inflammatory response syndrome, SIRS)之间存在着密切的联系,细胞因子合成和释放增多使得机体内稳态失衡,从而在SAP发生、发展中起着关键性的作用[15]。同时SAP还可诱导炎症细胞合成和释放大量炎症介质因子和细胞毒素,且以瀑布效应进展,反过来诱导激活更多的炎症细胞,最终加重SIRS[16-17]。SIRS可严重损伤血管内皮细胞,激活中性粒细胞和单核细胞,合成和释放大量有害氧自由基分子,进而加重全身炎症/凝血反应,使得凝血酶过量产生,导致纤溶系统激活、血管内血栓广泛形成和凝血因子大量消耗,最终出现异常高凝状态、微循环状态严重障碍,加重胰腺组织病变程度[18]。AT-Ⅲ是一种具有抗凝血及抗炎症反应的糖蛋白,可使机体内激活活化的凝血酶失去活性,不但可阻止弥散性血管内凝血的发生,减少脏器组织出血的风险性,明显缓解脏器组织缺血、缺氧等病理损伤,而且还可有效抑制凝血因子的促炎症反应作用,间接缓解炎症反应严重程度,同时AT-Ⅲ可通过多种途径抑制炎性细胞合成和释放炎性介质因子,最终起到抗炎症反应的作用[19]。研究[20-21]发现,AP病人血清AT-Ⅲ水平及功能活性均明显下降。本研究显示,不同病情严重程度及预后的AP病人血清AT-Ⅲ水平比较存在明显的差异性(P < 0.01),且随着病情加重和预后不佳血清AT-Ⅲ水平明显降低(P < 0.01),提示血清AT-Ⅲ在评估AP病人病情严重程度及预后方面具有重要的临床价值。
本研究选择血清AT-Ⅲ联合MCTSI作为评估AP病人病情严重程度及预后的指标,采用ROC曲线分析血清AT-Ⅲ联合MCTSI评分诊断AP和预测AP病人死亡的价值,结果显示:血清AT-Ⅲ联合MCTSI评分评估AP严重程度和预测AP病人死亡的AUC、敏感度及特异度均优于单一检测。由此可知,血清AT-Ⅲ联合MCTSI在评估AP病人病情严重程度及预后方面具有较高的临床价值。本研究还存在较多不足,如病例数相对较少,需继续扩大研究样本量,此外还需探讨动态监测两种指标的临床价值。
血清抗凝血酶Ⅲ联合改良CT严重指数评估急性胰腺炎严重程度及预后的价值
Value of serum antithrombin-Ⅲ combined with modified CT severity index in the evaluation of severity and prognosis of patients with acute pancreatitis
-
摘要:
目的探讨血清抗凝血酶-Ⅲ(AT-Ⅲ)联合改良CT严重指数(MCTSI)评估急性胰腺炎(AP)病人病情严重程度及预后的价值。 方法124例AP病人根据病情严重程度分为MAP组(38例)、MSAP组(46例)、SAP组(40例),根据预后不同分为存活组(110例)、死亡组(14例)。比较各组AP病人血清AT-Ⅲ水平及MCTSI评分,采用ROC曲线分析血清AT-Ⅲ联合MCTSI评分诊断SAP和预测AP病人死亡的价值。 结果不同病情严重程度AP病人血清AT-Ⅲ水平及MCTSI评分比较差异均有统计学意义(P < 0.01),AP病人随着病情严重程度增加,血清AT-Ⅲ水平降低,而MCTSI评分增加(P < 0.01);死亡组病人血清AT-Ⅲ水平低于存活组,而MCTSI评分高于存活组,差异均有统计学意义(P < 0.01);血清AT-Ⅲ联合MCTSI评分评估AP严重程度和预测AP病人死亡的AUC、敏感度及特异度均优于单一检测。 结论血清AT-Ⅲ联合MCTSI在评估AP病人病情严重程度及预后方面具有较高的临床价值。 Abstract:ObjectiveTo study the value of the serum antithrombin-Ⅲ(AT-Ⅲ) combined with modified CT severity index(MCTSI) in the evaluation of severity and prognosis of patients with acute pancreatitis(AP). MethodsOne hundred and twenty-four AP patients were divided into the MAP group(38 cases), MSAP group(46 cases) and SAP group(40 cases) according to the severity of the disease, and the survival group(110 cases) and death group(14 cases) according to the prognosis.The serum levels of AT-Ⅲ and MCTSI scores among the groups were compared.The value of serum AT-Ⅲ combined with MCTSI in the diagnosis of SAP and predicting the death in patients with AP were analyzed using the ROC curve. ResultsThe differences of the serum levels of AT-Ⅲ and MCTSI scores among different disease severity of AP patients were statistically significant(P < 0.01).With the severity of disease increasing, the serum levels of AT-Ⅲ decreased, and the MCTSI scores increased(P < 0.01).The serum level of AT-Ⅲ in death group was significantly lower than that in survival group(P < 0.01), while the MCTSI score was significantly higher than that in survival group(P < 0.01).The AUC, sensitivity and specific degrees of serum AT-Ⅲ combined with MCTSI in the evaluation of AP severity and predicting of death in patients with AP were superior to single detection. ConclusionsThe serum AT-Ⅲ combined with MCTSI in the assessment of disease severity and prognosis of patients with AP has a higher clinical value. -
Key words:
- acute pancreatitis /
- antithrombin-Ⅲ /
- modified CT severity index
-
表 1 不同病情严重程度AP病人血清AT-Ⅲ水平及MCTSI评分比较(x±s)
分组 n AT-Ⅲ/(mg/L) MCTSI评分/分 MAP组 38 256.75±60.43 3.67±0.74 MSAP组 46 187.31±42.35** 5.05±1.13** SAP组 40 132.62±35.54**△△ 7.22±1.47**△△ F — 68.75 93.82 P — < 0.01 < 0.01 MS组内 — 2 190.786 1.338 q检验:与MAP组比较**P < 0.01;与MSAP组比较△△P < 0.01  下载: 导出CSV
下载: 导出CSV
表 2 不同预后AP病人血清AT-Ⅲ水平及MCTSI评分比较(x±s)
分组 n AT-Ⅲ/(mg/L) MCTSI评分/分 存活组 110 193.87±73.32 4.76±1.47 死亡组 14 101.15±31.20* 7.93±1.17 t — 8.52 7.75 P — < 0.01 < 0.01 *示t′值
下载: 导出CSV
表 3 血清AT-Ⅲ联合MCTSI评分诊断SAP的价值分析
指标 截断值 敏感度/% 特异度/% 约登指数 AUC AT-Ⅲ/(mg/L) 150.72 80.0 71.4 0.51 0.782 MCTSI/分 6.05 82.5 76.2 0.59 0.815 AT-Ⅲ+MCTSI — 92.5 85.7 0.78 0.897
下载: 导出CSV
表 4 血清AT-Ⅲ联合MCTSI预测AP病人死亡的价值分析
指标 截断值 敏感度/% 特异度/% 约登指数 AUC AT-Ⅲ/(mg/L) 125.84 78.6 70.0 0.49 0.760 MCTSI/分 6.31 85.7 74.5 0.60 0.821 AT-Ⅲ+MCTSI — 92.9 81.8 0.75 0.875
下载: 导出CSV
-
[1] BANKS PA, BOLLEN TL, DERVENIS C, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus[J]. Gut, 2013, 62(1): 102. doi: 10.1136/gutjnl-2012-302779 [2] GREENBERG JA, HSU J, BAWAZEER M, et al. Clinical practice guideline: management of acute pancreatitis[J]. Can J Surg, 2016, 59(2): 128. doi: 10.1503/cjs.015015 [3] SHAHZAD N, KHAN MR, INAM PAL KM, et al. Role of early contmst enhanced CT scan in severity prediction of acute pancreatitis[J]. J Pak Med Assoc, 2017, 67(6): 923. [4] 王健, 郁毅刚, 林庆斌. 改良CT严重指数和CT严重指数对急性胰腺炎严重程度和预后的预测价值[J]. 中国医师进修杂志, 2018, 41(1): 21. doi: 10.3760/cma.j.issn.1673-4904.2018.01.006 [5] SAMRA N, ALGHWASS M, ELGAWHARY S, et al. Serum level of antithrombin Ⅲ(ATⅢ) could serve as a prognostic biomarker in neonatal sepsis[J]. Fetal Pediatr Pathol, 2019, 38(4): 290. doi: 10.1080/15513815.2019.1587118 [6] FIDAN S, ERKUT M, COSAR AM, et al. Higher thrombin-antithrombin Ⅲ complex levels may indicate severe acute pancreatitis[J]. Dig Dis, 2018, 36(3): 244. doi: 10.1159/000485613 [7] 袁涛, 全冠民, 石伟, 等. 急性胰腺炎新分类相关术语和并发症及MCTSI评分[J]. 放射学实践, 2015, 30(10): 1005. [8] TSUJI Y, TAKAHASHI N, ISODA H, et al. Early diagnosis of pancreatic necrosis based on perfusion CT to predict the severity of acute pancreatitis[J]. J Gastroenterol, 2017, 52(10): 1147. doi: 10.1007/s00535-017-1343-0 [9] GUI J, XIONG J, ZHANG Y, et al. Serum lactate dehydrogenase is predictive of persistent organ failure in acute pancreatitis[J]. J Crit Care, 2017, 41: 161. doi: 10.1016/j.jcrc.2017.05.001 [10] YADAV AK, SHARMA R, KANDASAMY D, et al. Perfusion CT: can it predict the development of pancreatic necrosis in early stage of severe acute pancreatitis?[J]. Abdom Imaging, 2015, 40(3): 488. doi: 10.1007/s00261-014-0226-6 [11] 邹金艳, 林军, 易三凤, 等. BISAP、Ranson's、APACHEП和CTSI评分系统在急性胰腺炎评估中的价值[J]. 中华消化外科杂志, 2014, 13(1): 39. doi: 10.3760/cma.j.issn.1673-9752.2014.01.012 [12] 蔡兆辉, 左爽, 李海山, 等. BISAP和CTSI评分变化用于判断急性胰腺炎病人病情严重程度的临床价值[J]. 解放军预防医学杂志, 2019, 37(2): 90. [13] BANDAY IA, GATTOO I, KHAN AM, et al. Modified computed tomography severity index for evaluation of acute pancreatitis and its correlation with clinical outcome: a tertiary care hospital based observational study[J]. J Clin Diagn Res, 2015, 9(8): TC01. [14] 闫媛媛, 张洁, 靳二虎. 改良CT和MR严重指数在急性胰腺炎诊断中的应用研究[J]. 临床和实验医学杂志, 2018, 17(10): 1037. doi: 10.3969/j.issn.1671-4695.2018.10.010 [15] 曹均强, 汤礼军. 全身炎症反应综合征在急性胰腺炎肺损伤中的研究进展[J]. 中华消化外科杂志, 2015, 14(11): 975. doi: 10.3760/cma.j.issn.1673-9752.2015.11.019 [16] BALK RA. Systemic inflammatory response syndrome(SIRS): where did it come from and is it still relevant today?[J]. Virulence, 2014, 5(1): 20. doi: 10.4161/viru.27135 [17] KAUKONEN KM, BAILEY M, PILCHER D, et al. Systemic inflammatory response syndrome criteria in defining severe sepsis[J]. N Engl J Med, 2015, 372(17): 1629. doi: 10.1056/NEJMoa1415236 [18] 郭晓钟. 重症急性胰腺炎致全身炎症反应综合征的诊治策略[J]. 中华消化杂志, 2019, 39(5): 289. doi: 10.3760/cma.j.issn.0254-1432.2019.05.001 [19] LESTARI IN, YOEL C, LUBIS M, et al. The association between the level of antithrombin Ⅲ and mortality in children with sepsis[J]. Open Access Maced J Med Sci, 2019, 7(6): 959. doi: 10.3889/oamjms.2019.211 [20] YANG N, HAO J, ZHANG D. Antithrombin Ⅲ and D-dimer levels as indicators of disease severity in patients with hyperlipidaemic or biliary acute pancreatitis[J]. J Int Med Res, 2017, 45(1): 147. doi: 10.1177/0300060516677929 [21] KONG Y, YIN J, CHENG D, et al. Antithrombin Ⅲ attenuates AKI following acute severe pancreatitis[J]. Shock, 2018, 49(5): 572. doi: 10.1097/SHK.0000000000000946 -

 点击查看大图
点击查看大图
图(2)表(4)
计量
- 文章访问数: 6316
- HTML全文浏览量: 3495
- PDF下载量: 5
- 被引次数: 0
