


-
ST段抬高型心肌梗死(ST elevation myocardial infarction,STEMI)为临床常见心脏急性事件,以剧烈而持久的胸骨后疼痛,经休息或硝酸酯类药物无法完全缓解为临床表现,同时伴有心电图ST段抬高[1-3]。平均血小板体积(meam platelet volume, MPV)与血小板活化程度呈负相关,在多种心血管疾病的风险评估、诊断及预后预测方面均得到广泛的应用[1, 4]。虽然近年来随着溶栓、经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)、主动脉球囊反搏等技术的发展,STEMI的病死率有所下降,但全球每年因缺血性心脏病死亡的病人数仍在百万以上,因此对STEMI死亡预测具有重要的意义[5]。目前关于STEMI病人死亡预测指标有高敏C反应蛋白、冠状动脉钙化积分、D-二聚体等,但在基层医院中多不涉及上述指标[6-7]。MPV为血常规检查中常用的指标,具有较高的普及率,研究证实MPV可用于STEMI病人住院期间死亡事件预测[8],但关于MPV对STEMI病人远期预后预测方面研究较少,同时关于MPV及STEMI病人治疗后再灌注损伤预测未见相关报道,心肌缺血再灌注损伤为STEMI病人远期预后的重要影响因素,对心肌缺血再灌注损伤的预测有助于提高预后预测的准确性,因此本研究旨在通过相关分析以期为STEMI病人的远期死亡预测提供新的思路。
-
选择2015-2016年在我院接受住院治疗的STEMI病人193例进行研究。纳入标准:(1)符合《2015年中国急性ST段抬高型心肌梗死诊断及治疗指南》[9]中的相关诊断,且均为首次发病;(2)无血液系统恶性疾病(以病史记载为依据);(3)病人均由同一组医护人员在发病12 h内完成PCI治疗且成功开通梗死相关血管;(4)病人或其家属已获知情同意。排除标准:(1)终末期肝病病人;(2)终末期肾病病人;(3)感染、肺栓塞、风湿结缔组织疾病病人;(4)心脏瓣膜病病人;(5)既往陈旧性心肌梗死病人;(6)冠状动脉旁路移植术病人;(7)肥厚型心肌病及扩张型心肌病等心脏疾病病人。
-
(1) MPV检测:受试者入组当日行抗凝治疗及PCI术前抽取肘正中静脉血5 mL,置含抗凝剂标管中,采用Sysmex XE-2100型全自动五分类血细胞分析仪及其配套试剂对MPV进行检测,所有检测均在采血后120 min内完成。(2)随访:对于好转出院者,以门诊、电话、微信等方式对病人本人或其家属进行随访,随访期间均有同一组医师严格按《2015年中国急性ST段抬高型心肌梗死诊断及治疗指南》[9]对病人进行治疗,记录预后及心脏不良事件情况,以全因死亡为终点事件。对比随访存活及死亡组病人MPV水平,以ROC法分析MPV对急性心肌梗死病人死亡预测截断值,并比较不同MPV水平病人心脏不良反应发生情况及进行生存分析。(3)心肌缺血再灌注损伤判断标准:在直接PCI开通梗死相关血管后数分钟内出现严重心动过缓及低血压,或需要电复律的严重室性心律失常,梗死相关动脉前向血流TIMI分级在2级及以下且除外因造影可见的血栓、栓塞、夹层或痉挛所致的急性闭塞均认为是心肌缺血再灌注损伤。根据心肌缺血再灌注损伤发生情况将STEMI病人分为2组,比较2组病人MPV水平。
-
采用t检验、多因素logistic回归分析、受试者工作曲线(ROC)、Kaplan-Meier曲线生存分析和Log-Rank检验。
-
本组193例病人中男99例,女94例;年龄45~71岁,平均(58.19±12.06)岁;体质量指数19.43~28.02 kg/m2,平均(24.10±3.16)kg/m2;有吸烟史84例,高血压103例,糖尿病75例;病变血管:左冠状动脉前降支96例,左回旋支31例,右冠状动脉102例;血管病变单支81例,多支112例。所有病人均在STEMI后随诊至2019年10月8日,平均随诊时间(35.02±7.13)个月,164例完成随访,随访率85.0%,其中心源性死亡35例(18.1%),非心源性死亡3例(1.6%)。
-
存活组病人中性粒细胞、嗜碱性粒细胞与MPV水平均低于死亡组病人(P < 0.05~P < 0.01),而嗜酸性粒细胞水平高于死亡组病人(P < 0.01)(见表 1)。
分组 n 红细胞/ (×1012/L) 白细胞/ (×109/L) 中性粒细胞/ (×109/L) 淋巴细胞/ (×109/L) 嗜酸性粒细胞/ (×109/L) 嗜碱性粒细胞/ (×109/L) 红细胞分布宽度 MPV/fL 血小板/ (×103/μL) 存活组 126 5.33±1.61 7.59±2.35 3.72±1.46 2.79±0.83 0.26±0.01 0.07±0.02 35.58±5.39 12.93±3.17 225.84±126.75 死亡组 38 5.38±1.75 7.32±2.61 5.39±1.51 2.57±0.69 0.13±0.01 0.08±0.02 36.27±5.19 14.87±3.42 233.09±127.59 t — 0.16 0.61 6.13 1.49 70.24 2.70 0.70 3.25 0.31 P — >0.05 >0.05 < 0.01 >0.05 < 0.01 < 0.05 >0.05 < 0.05 >0.05 表 1 不同预后情况病人血常规指标的比较(x±s)
-
以表 1中具有统计学意义的变量为自变量,STEMI病人远期预后情况为因变量进行多因素logistic回归分析,自变量均为连续型变量,均按实际值进入回归,因变量赋值:死亡=0,存活=1,结果显示:MPV低为STEMI病人存活的保护性因素(P < 0.05)(见表 2)。
变量 B SE Waldχ2 P OR 95%CI 中性粒细胞 -0.274 0.162 2.86 >0.05 0.760 0.553 ~1.044 嗜酸性粒细胞 0.195 0.117 2.78 >0.05 1.215 0.966 ~1.529 嗜碱性粒细胞 -0.203 0.129 2.48 >0.05 0.816 0.634 ~1.051 MPV -0.377 0.162 5.42 < 0.05 0.686 0.499 ~0.942 表 2 血常规指标及MPV对STEMI病人远期预后多因素分析
-
MPV对STEMI病人远期死亡预测截断值为13.14 fL,ROC曲线下面积(AUC)为0.741,95%CI:0.658~0.824,灵敏度为78.94%(30/38),特异度为83.33%(105/126),准确度为82.32%(135/164),阳性预测值为58.82%(30/51),阴性预测值为92.92%(105/113)(见图 1、表 3)。
MPV 随访结果 合计 生存 死亡 < 13.14 fL 105 8 113 ≥13.14 fL 21 30 51 合计 126 38 164 表 3 MPV对STEMI病人远期死亡的预测价值(n)
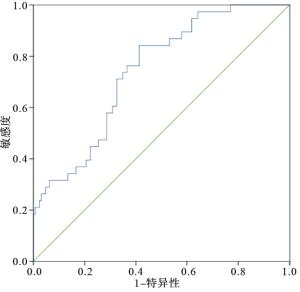
图 1 ROC曲线分析
-
根据ROC分析结果,将病人分为MPV低水平组(MPV < 13.14 fL)113例,死亡8例;MPV高水平组(MPV≥13.14 fL)51例,死亡30例。以Kaplan-Meier分析法对STEMI病人入院时MPV水平与远期生存关系进行分析,MPV低水平组中位生存时间为33个月(95%CI:31.092~34.263)长于MPV高水平组的25个月(95%CI:22.132~27.291)(χ2=70.27,P < 0.01)(见图 2)。
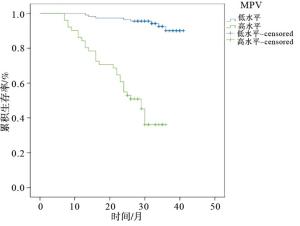
图 2 STEMI病人生存分析图
-
MPV低水平组(MPV < 13.14 fL)心脑血管事件共发生28例,其中心源性死亡5例,再发心肌梗死4例,再发心绞痛8例,再次血运重建8例,脑卒中3例;MPV高水平组(MPV≥13.14 fL)出现心脑血管事件39例,其中心源性死亡30例,再发心肌梗死5例,再发心绞痛3例,脑卒中1例。MPV低水平组脑血管事件发生率24.78%(28/113)低于高水平组的76.47%(39/51)(χ2=38.86,P < 0.01)。
-
193例STEMI病人中,共有98例(50.78%)出现不同程度的心肌缺血再灌注损伤,心肌缺血再灌注损伤组病人MPV水平为(14.72±3.27)fL,高于无心肌缺血再灌注损伤的(13.06±3.11)fL(t=3.61,P < 0.01)。
-
目前关于STEMI病人远期死亡率预测指标的研究多集中于C反应蛋白、B型尿钠肽等血液生化分析指标,但上述指标检测费用较高且在国内基层医院中普及度不高,因而对于基层医院的应用价值不高[10-11]。血小板为巨核细胞发育的最后阶段,多项研究证实血小板计数、形态及分泌均与血栓的发生密不可分,血小板高反应性信号通路失调在STEMI病人血栓形成中起着关键的作用,在众多的血小板高反应性指标中MPV因获取简单、普及度高、与血小板活化倾向相关性强等优势受到关注最多[12]。MPV为血常规检查项目,在国内大部分基层医院均有开展相关检测,过去MPV多用于出血倾向及骨髓造血功能的判断,MPV水平升高,血小板体积增大,活性增强,研究[13]证实MPV升高与心血管疾病的发生发展具有密切的关系。关于血小板参与STEMI的机制方面研究较多,研究[14]证实动脉粥样硬化斑块在破裂后1 min,血小板即可迅速与胶原蛋白、纤维蛋白等结合在破损的斑块表面聚集、黏附,在3 min后血小板周围即可出现成型纤维蛋白及凝血酶,导致血栓的形成;活化的血小板细胞质中的反应酶、蛋白及细胞膜上的血小板生长因子受体α、β等受体的表达增加,使血小板的体积随之增大,MPV水平上升,MPV水平的升高又可导致血小板活性增强,引起血栓形成风险上升最终导致STEMI的发生,形成恶性循环。另外,有研究[15]显示,血小板体积分布宽度(PDW)、血小板计数(PLT)等指标也被证实可用于STEMI病人的预后预测,PDW主要反映血小板体积变化程度,PLT则反映血小板数量,STEMI发生发展过程中血栓形成需要消耗大量血小板,使PLT水平下降,PLT下降可使巨核细胞释放大量较大的新生血小板至外周血,新生血小板体积较大、代谢更为活跃,MPV可反映骨髓巨噬细胞增生及血小板生成情况,较PLT及PDW可更为直观地反映血小板高反应性。
STEMI病人的临床转归对临床治疗决策具有重要的影响,STEMI的高病死率要求对此类病人早期需进行溶栓、PCI等治疗,同时在改善远期预后方面需合理地进行针对性的抗凝、降血脂等预防性治疗,以降低STEMI病人的心源性死亡率。梗死相关血管的快速、充分开通对于挽救严重缺血的心肌、缩小梗死面积降低病人死亡率具有重要的意义,但梗死相关血管开通后并非所有病人均可从中获益,甚至有部分病人因出现急性血流动力学障碍而死亡,心肌缺血再灌注损伤是引起病人出现上述情况的主要原因。关于MPV对STEMI病人住院死亡率预测方面的研究已有相关报道,该研究[16]证实MPV与STEMI病人的院内死亡率存在显著的正相关关系,但关于MPV与STEMI病人远期死亡率及心肌缺血再灌注损伤的关系方面的报道较少。本研究通过随访分析结果显示:MPV为STEMI病人远期预后独立影响因素。可能与以下几方面因素有关:(1)血小板体积的增加使其伪足数量明显增加,增强血小板黏附及聚集能力,MPV水平较高的STEMI病人在治疗后再次出现血栓而引起心源性死亡事件的风险越大[17]。(2)血小板体积较大者凝血潜能更强,其膜表面经糖蛋白表达的GPⅠb及GPⅡb/Ⅲa受体数量更多,同时大体积血小板对于血栓素A2的释放有促进作用,上述改变可增加病人再次血栓的风险。再者体积较大的血小板其细胞质内的α-颗粒等细胞内储存颗粒含量更多,α-颗粒是血小板衍生生长因子、黏附因子及凝血因子的主要储存池,血小板释放上述颗粒至细胞外环境中,可有效激活邻近血小板而放大聚集、黏附效应[18]。(3)血小板体积增大还可增加血小板与纤维蛋白原的亲和力,使血小板的聚集效应增强,同时MPV较高者还可提高病人溶栓治疗的抵抗性,使药效降低而增加病人死亡风险[19]。
进一步分析结果显示,193例STEMI病人中,共有98例(50.78%)出现不同程度的心肌缺血再灌注损伤,心肌缺血再灌注损伤组病人MPV水平,高于无心肌缺血再灌注损伤者。提示高水平MPV可增加PCI术后病人心肌缺血再灌注损伤的风险,目前对于此问题的相关研究较少,MPV水平较高者可放大血小板聚集及黏附效应,可能是MPV水平升高增加心肌缺血再灌注损伤的原因之一,至于具体机制尚有待进一步研究。
综上所述,MPV可作为STEMI病人远期预后的评价指标,当STEMI病人MPV≥13.14 fL时病人的远期死亡风险明显增加,同时MPV水平升高心肌缺血再灌注风险上升。但本研究样本量有限,随访时间不长,取得的结果可能出现一定的偏差,下步将扩大样本量、增加中心,延长随访时间以进一步证实本研究结果。
ST段抬高型心肌梗死病人远期死亡率与入院首次化验时平均血小板体积的关系
Study on the relationship between long-term mortality and mean platelet volume at the first test in patients with ST-segment elevation myocardial infarction
-
摘要:
目的探讨ST段抬高型心肌梗死(STEMI)病人远期死亡率与入院首次化验时平均血小板体积(MPV)的关系。 方法选择STEMI病人193例进行研究,病人均在STEMI后随诊至2019年10月8日,根据随访结果将病人分为存活组及死亡组,对比2组血常规指标水平,采用多元线性回归对血常规指标与STEMI远期预后关系进行分析,以ROC分析MPV对STEMI远期死亡的预测截断值,以Kaplan-Meier曲线进行生存分析,采用Log-Rank检验。 结果血常规指标比较显示,存活组病人中性粒细胞、嗜碱性粒细胞与MPV水平均低于死亡组病人(P < 0.05~P < 0.01),嗜酸性粒细胞高于死亡组病人(P < 0.01)。MPV对STEMI病人远期死亡预测截断值为13.14 fL,AUC为0.741,95%CI:0.658~0.824,灵敏度为78.94%(30/38),特异度为83.33%(105/126),准确度为82.32%(135/164),阳性预测值为58.82%(30/51),阴性预测值为92.92%(105/113)。ROC分析结果显示,MPV低水平组(MPV < 13.14 fL)病人113例,死亡8例;MPV高水平组(MPV ≥ 13.14 fL)51例,死亡30例。Kaplan-Meier分析显示,MPV低水平组中位生存时间为33个月(95%CI:31.09~34.26),高于MPV高水平组的25个月(95%CI:22.13~27.29)(P < 0.01)。MPV低水平组脑血管事件发生率24.78%低于高水平组的76.47%(P < 0.01)。193例STEMI病人中,共有98例(50.78%)出现不同程度的心肌缺血再灌注损伤,心肌缺血再灌注损伤病人MPV水平高于无心肌缺血再灌注损伤病人(P < 0.01)。 结论STEMI病人入院首次化验时MPV水平明显高于健康人群,MPV可作为STEMI病人远期预后的评价指标,当STEMI病人MPV ≥ 13.14 fL时病人的远期死亡风险明显增加,同时MPV水平升高心肌缺血再灌注风险上升。 -
关键词:
- ST段抬高型心肌梗死 /
- 平均血小板体积 /
- 死亡率 /
- 生存分析
Abstract:ObjectiveTo investigate the relationship between long-term mortality and mean platelet volume(MPV) at the first test in patients with ST-segment elevation myocardial infarction(STEMI). MethodsA total of 193 STEMI patients were followed up until October 8, 2019 after STEMI.According to the results of following up, the patients were divided into the survival group and death group.The blood routine indexes between the two groups were compared.The relationship between the blood routine indexes and long-term prognosis of STEMI was analyzed using multiple linear regression analysis, the cut-off value of MPV to long-term mortality of STEMI was analyzed using ROC analysis, the survival analysis was conducted by Kaplan-Meier curve, and the Log-Rank test was used. ResultsThe results of blood routine indicators analysis showed that the levels of neutrophils, eosinophils, basophils and MPV in survival group were significantly lower than those in death group(P < 0.05 to P < 0.01).The cut-off value of MPV predicting long-term death in STEMI patients was 13.14 fL, the AUC was 0.741, the 95%CI was 0.658-0.824, the sensitivity was 78.94%(30/38), the specificity was 83.33%(105/126), the accuracy was 82.32% (135/164), the positive predictive value was 58.82% (30/51), and the negative predictive value was 92.92%(105/113).The results of ROC analysis showed that 8 patients died in the low-level MPV group(113 cases, MPV < 13.14 fL), and 30 patients died in the high level MPV group(51 cases, MPV ≥ 13.14 fL).The results of Kaplan-Meier analysis showed that the median survival time in low-level MPV group was 33 months(95%CI: 31.09-34.26), which was higher than that in high-level MPV group[25 months, (95%CI: 22.13-27.29)] (P < 0.01).The incidence rates of cerebrovascular events in low-level MPV group(24.78%) was lower than that in high-level MPV group(76.47%)(P < 0.01).Among 193 STEMI patients, 98 patients (50.78%) with different degrees of myocardial ischemia reperfusion injury were identified, and the level of MPV in patients with myocardial ischemia reperfusion injury was higher than that in patients without myocardial ischemia reperfusion injury(P < 0.01). ConclusionsThe level of MPV in STEMI patients is significantly higher than that in healthy people at the first test, and the MPV can be used as an indicator for the long-term prognosis of STEMI patients.When the MPV is more than or equal to 13.14 fL, the risk of long-term death in patients with STEMI significantly increases, and the risk of myocardial ischemia reperfusion increases with the increasing of MPV level. -
Key words:
- ST elevation myocardial infarction /
- mean platelet volume /
- mortality /
- survival analysis
-
表 1 不同预后情况病人血常规指标的比较(x±s)
分组 n 红细胞/ (×1012/L) 白细胞/ (×109/L) 中性粒细胞/ (×109/L) 淋巴细胞/ (×109/L) 嗜酸性粒细胞/ (×109/L) 嗜碱性粒细胞/ (×109/L) 红细胞分布宽度 MPV/fL 血小板/ (×103/μL) 存活组 126 5.33±1.61 7.59±2.35 3.72±1.46 2.79±0.83 0.26±0.01 0.07±0.02 35.58±5.39 12.93±3.17 225.84±126.75 死亡组 38 5.38±1.75 7.32±2.61 5.39±1.51 2.57±0.69 0.13±0.01 0.08±0.02 36.27±5.19 14.87±3.42 233.09±127.59 t — 0.16 0.61 6.13 1.49 70.24 2.70 0.70 3.25 0.31 P — >0.05 >0.05 < 0.01 >0.05 < 0.01 < 0.05 >0.05 < 0.05 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 血常规指标及MPV对STEMI病人远期预后多因素分析
变量 B SE Waldχ2 P OR 95%CI 中性粒细胞 -0.274 0.162 2.86 >0.05 0.760 0.553 ~1.044 嗜酸性粒细胞 0.195 0.117 2.78 >0.05 1.215 0.966 ~1.529 嗜碱性粒细胞 -0.203 0.129 2.48 >0.05 0.816 0.634 ~1.051 MPV -0.377 0.162 5.42 < 0.05 0.686 0.499 ~0.942
下载: 导出CSV
表 3 MPV对STEMI病人远期死亡的预测价值(n)
MPV 随访结果 合计 生存 死亡 < 13.14 fL 105 8 113 ≥13.14 fL 21 30 51 合计 126 38 164
下载: 导出CSV
-
[1] LIU X, WANG S, YUAN L, et al. Increased mean platelet volume is associated with higher in-hospital mortality rate in patients with acute myocardial infarction[J]. Clin Lab, 2017, 63(1): 163. [2] JIANG P, SONG Y, XU JJ, et al. Two-year prognostic value of mean platelet volume in patients with diabetes and stable coronary artery disease undergoing elective percutaneous coronary intervention[J]. Cardiol J, 2019, 26(2): 138. [3] ORAK M, KARAKOÇ Y, VSTVNDAG M, et al. An investigation of the effects of the mean platelet volume, platelet distribution width, platelet/lymphocyte ratio, and platelet counts on mortality in patents with sepsis who applied to the emergency department[J]. Niger J Clin Pract, 2018, 21(5): 667. doi: 10.4103/njcp.njcp_44_17 [4] HUDZIK B, KORZONEK-SZLACHETA I, SZKODZIŃSKI J, et al. Association between multimorbidity and mean platelet volume in diabetic patients with acute myocardial infarction[J]. Acta Diabetol, 2018, 55(2): 175. doi: 10.1007/s00592-017-1079-6 [5] MEERSHOEK AJA, LEUNISSEN TC, VAN WAES JAR, et al. Reticulated platelets as predictor of myocardial injury and 30 day mortality after non-cardiac surgery[J]. Eur J Vasc Endovasc, 2020, 59(2): 309. doi: 10.1016/j.ejvs.2019.06.027 [6] 唐小勇, 钟万芬. D-二聚体水平评价急性心肌梗死危险程度及对预后的预测[J]. 现代医学, 2016(5): 697. [7] PAFILI K, PENLIOGLOU T, MIKHAILIDIS DP, et al. Mean platelet volume and coronary artery disease[J]. Curr Opin Cardiol, 2019, 34(4): 390. doi: 10.1097/HCO.0000000000000624 [8] GUO TM, CHENG B, KE L, et al. Prognostic value of neutrophil to lymphocyte ratio for in-hospital mortality in elderly patients with acute myocardial infarction[J]. Curr Med Sci, 2018, 38(2): 354. doi: 10.1007/s11596-018-1887-0 [9] 袁晋青, 宋莹. 《2015年中国急性ST段抬高型心肌梗死诊断及治疗指南》——更新要点解读[J]. 中国循环杂志, 2016, 31(4): 318. doi: 10.3969/j.issn.1000-3614.2016.04.002 [10] MARTIN-GARCIA AC, ARACHCHILLAGE DRJ, KEMPNY A, et al. Platelet count and mean platelet volume predict outcome in adults with Eisenmenger syndrome[J]. Heart, 2018, 104(1): 45. doi: 10.1136/heartjnl-2016-311144 [11] HAMEED A, RUBAB Z, RIZVI SKA, et al. Levels of platelet-derived microparticles and soluble p-selectin in patients of acute myocardial infarction (Case control study)[J]. J Pak Med Assoc, 2017, 67(7): 998. [12] LI YH, WANG LH, LI Q, et al. Effects of rosuvastatin on pentraxin 3 level and platelet aggregation rate in elderly patients with acute myocardial infarction undergoing elective interventional therapy: a double-blind controlled study[J]. Eur Rev Med Pharmacol Sci, 2017, 21(16): 3730. [13] EL-BATTRAWY I, BORGGREFE M, AKIN I. β-Blockers and outcome after acute myocardial infarction[J]. J Am Coll Cardiol, 2017, 70(13): 1685. [14] 杨华, 陈枝琼. 血小板参数在判断强直性脊柱炎疾病活动中的价值[J]. 蚌埠医学院学报, 2018, 265(1): 52. [15] 许丽娇, 黄东平, 汪云霞. 红细胞分布宽度及血小板参数在急性心肌梗死诊断中的应用研究[J]. 临床医学工程, 2016, 23(11): 1515. doi: 10.3969/j.issn.1674-4659.2016.11.1515 [16] MUBANG R, TERZIAN WH, CIPOLLA J, et al. Acute myocardial infarction following right coronary artery dissection due to blunt trauma[J]. Heart Views, 2016, 17(1): 35. doi: 10.4103/1995-705X.182646 [17] BESLI F, ILTER A, GUNGOREN F. The link between mean platelet volume to lymphocyte ratio and complexity of coronary artery disease[J]. Angiology, 2018, 69(4): 358. doi: 10.1177/0003319717743315 [18] OMAR M, TANRIVERDI O, COKMERT S, et al. Role of increased mean platelet volume (MPV) and decreased MPV/platelet count ratio as poor prognostic factors in lung cancer[J]. Clin Respir J, 2018, 12(3): 922. doi: 10.1111/crj.12605 [19] PENG F, ZHENG W, LI F, et al. Elevated mean platelet volume is associated with poor outcome after mechanical thrombectomy[J]. J Neurointerv Surg, 2018, 10(1): 25. doi: 10.1136/neurintsurg-2016-012849 -

 点击查看大图
点击查看大图

图(2)表(3)
计量
- 文章访问数: 3428
- HTML全文浏览量: 1716
- PDF下载量: 4
- 被引次数: 0
