



-
脱出型黏膜下肌瘤是带蒂黏膜下肌瘤沿宫腔向下延伸至宫颈管或脱入阴道形成的[1]。经阴道二维超声(2D-TVS)对脱出型黏膜下肌瘤有较高的检出率,但是在与其他宫腔病变鉴别上存在一定困难,经验不足者易误诊。三维超声(3D-TVS)能立体直观地显示瘤体全貌,血流显像(3D-DUS)则能显示瘤体内血流走行,有助于判断肌瘤蒂部位置,之前未见相关报道。本研究通过分析脱出型黏膜下肌瘤的2D-TVS、3D-TVS及3D-DUS声像图特点,并将检查结果与手术病理结果进行比较,以提高该病的检出率及诊断准确性。现作报道。
-
选择2016年1月至2019年11月因不规则阴道出血、不孕等原因来我院就诊,临床妇检发现宫颈赘生物,可疑脱出型黏膜下肌瘤并要求手术的病人57例。年龄20~51岁,平均年龄(46±6.4)岁。其中21例有不同程度贫血。
-
2D-TVS:采用GE Voluson E8、E10型超声诊断仪,配有腔内探头,频率5~9 MHz。病人排尿后取膀胱截石位,阴道探头外套无菌安全套,置入阴道。观察并记录子宫大小形态,宫腔内病灶大小、形态、边界、位置及内部回声,有无“Ⅰ”形蒂部结构,以及蒂部在宫腔的位置。彩色多普勒血流显像(color doppler flow image, CDFI)或彩色多普勒能量图(color doppler energy, CDE)观察病灶内部及周边血流情况,获取血流频谱,做出诊断。
3D-TVS:采用GE Voluson E8、E10型超声诊断仪,配有RIC-5-9-D探头,频率5~9 MHz。选择宫腔内病灶显示最佳的子宫长轴切面为中心平面,采用表面成像方法,获取三维容积图像。根据瘤体形态,通过调整X、Y、Z轴角度,显示最佳病灶冠状切面。重点观察宫腔病变与内膜及肌层的关系,占据宫腔及宫颈的情况,基底部大小及来源。3D-DUS选择子宫长轴切面,将彩色取样框放置于感兴趣区,启动3D功能,获取三维血流容积图像。主要查看病灶内的供血情况、血流走行及血流来源,做出诊断。
所有病例均在我院行宫腔镜或经腹手术治疗,以病理检查结果作为金标准。将2D-TVS与3D-TVS诊断结果分别与病理结果进行对比。并根据手术结果,将脱出型黏膜下肌瘤病人作为确诊组,非肌瘤性病变病人作为疑似组,比较2组病人的“低回声为主”“Ⅰ形蒂部结构”等声像图特点。
-
采用χ2检验。
-
57例病人经手术病理诊断为脱出型黏膜下肌瘤34例,宫颈炎性息肉20例(含息肉样腺肌瘤3例),宫颈癌1例,子宫内膜癌1例,宫颈肌瘤1例。一致性检验表明,2D-TVS和3D-TVS均能检出脱出型黏膜下肌瘤,2种方法诊断灵敏度差异无统计学意义(χ2=0.25,P > 0.05),3D-TVS诊断特异度高于2D-TVS(χ2=5.14,P < 0.05)(见表 1)。
方法 灵敏度/% 特异度/% 误诊率/% 漏诊率/% Youden指数 一致百分率/% 阳性似然比 阴性似然比 2D-TVS 88.2 54.5 45.5 11.8 0.427 75 1.939 0.217 3D-TVS 94.1 86.4 13.6 5.9 0.805 91 6.919 0.068 表 1 2D-TVS与3D-TVS的诊断准确率比较
-
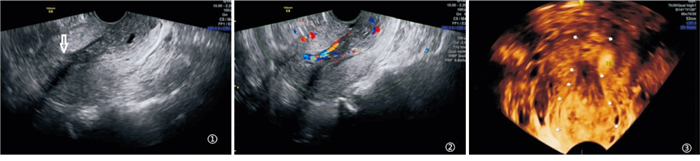
2D-TVS示宫腔及宫颈管内见低回声团,呈长条状,上小下大,与肌层分界较为清晰,宫颈管增粗。瘤体上端可见稍高或低回声的条状结构与肌层相延续,即“Ⅰ”形蒂部结构。CDFI/CDE:瘤体血供丰富,沿宫体长轴走行的数个条状血流,至蒂部血流汇聚。2D-TVS冠状面宫腔及宫颈管内见“梨形”或“哑铃形”混合回声团,边界清晰,瘤体上端与肌层延续。3D-DUS瘤体内见数条沿宫腔长轴走行的血流,血流上端汇聚呈束状。典型病例声像图表现见图 1~3。
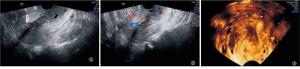
图 1 典型病例1, 手术病理示子宫-宫颈黏膜下肌瘤
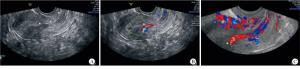
图 2 典型病例2, 手术病理示子宫-宫颈黏膜下肌瘤
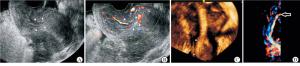
图 3 典型病例3, 手术病理示子宫-宫颈黏膜下肌瘤
在2D-TVS的低回声为主、“Ⅰ”形蒂部结构、丰富条状血流和3D-TVS的“梨形”团块及3D-DUS的蒂部条束状血流方面,确诊组病人检出率均高于疑似组(P < 0.05~P < 0.01)(见表 2)。
特征表现 确诊组
(n=34)疑似组
(n=23)χ2 P 灵敏度/% 特异度/% 2D-TVS 低回声为主 是
否31
315
85.94 < 0.05 91.2 33.3 “Ⅰ”形蒂部结构 是
否26
811
124.94 < 0.05 76.5 52.0 丰富条状血流 是
否31
316
74.43 < 0.05 91.2 30.4 3D-TVS 团块呈“梨形” 是
否19
154
198.44 < 0.01 55.9 83.0 3D-DUS 蒂部条束状血流 是
否26
811
124.94 < 0.05 76.5 52.2 表 2 特征性声像图在确诊组与疑似组病人中表现比较
-
黏膜下肌瘤向宫腔内继续生长如异物一般可引起子宫收缩,迫使肌瘤逐渐下移至宫颈管内,甚至排入阴道[2]。由于脱出型黏膜下肌瘤使内膜面积增加,且对宫腔造成一定的压迫,影响子宫收缩,往往导致经期延长、经量过多,甚至出现失血性贫血[3-4]。若瘤体脱出进入阴道内常容易合并感染伴有脓性分泌物等,对病人的健康及生活都产生严重影响,因此,及早诊断及治疗非常重要。
诊断性刮宫和宫腔镜是临床用来检查和治疗的常用方法,在宫腔镜下瘤体的大小、形态及起始位置一目了然[5],但由于属于侵入性操作,具有创伤性和风险性,不宜作为常规筛查方法。2D-TVS是目前临床诊断宫腔及宫颈管内占位的有效方法[6-7],其探头频率高,检查视野广,可以清晰显示宫腔内部结构,CDFI/CDE可以敏感显示瘤体内的血流信息。3D-TVS除了有2D-TVS的优势外还能获得子宫冠状面图像,在立体、全方位地观察瘤体形态的同时,还能更好地显示宫腔病变与内膜基底层和肌层的关系[8]。3D-DUS是一种新型多普勒技术,可以进行多个层面的血流信息重建,解决了CDFI/CDE因瘤体血流不在同一切面而呈断续状的问题,直观、立体地显示瘤体内血流的走行和分布。
脱出型黏膜下肌瘤瘤体大小及基底部位置的确定可为临床手术方式的选择提供重要依据。脱出型黏膜下肌瘤的蒂部是肌瘤附着点,也是血流发出点,血管较粗,当合并感染时血流会更加丰富。本研究确诊病例CDFI/CDE瘤体内条状血流出现率为91.2%(31/34),诊断敏感度91.2%,特异度30.4%。3D-DUS蒂部束状血流出现率为76.5%(26/34),诊断敏感度76.5%,特异度为52.2%。可见以上2种方法对瘤体内丰富条状血流及蒂部束状血流的显示均较敏感的,这与徐繁华等[1]研究结果一致,但在判断瘤体起始位置上3D-DUS较CDFI/CDE有更高的特异度。
当黏膜下肌瘤的超声表现不典型、宫腔内回声粗糙时,声像图易与其他宫腔病变相混淆。本研究误诊的1例子宫内膜癌,2D、3D-TVS声像图表现为长条状及低回声为主的瘤体形态,但瘤体边界欠清晰、无“Ⅰ”形蒂状结构、内部血流呈散在点状、短棒状。当黏膜下肌瘤脱入宫颈管或阴道内时,宫颈位置低,易受阴道气体干扰,且宫颈内膜随月经周期变化小,还易与宫颈息肉、宫颈肌瘤及宫颈癌相混淆。本组有7例误诊为宫颈管息肉,其中3例病理类型为腺肌瘤样息肉,息肉体积较大,有蒂,可见条状血流,与脱出型黏膜下肌瘤类似。但仔细分析,7例瘤体中4例呈等回声,3例呈稍高回声,追踪其蒂部血流多终止于子宫下段或宫颈内口处。而黏膜下肌瘤以低回声为主,蒂部位置多位于宫体部,存在差异。本研究误诊的1例宫颈癌和1例宫颈肌瘤,瘤体大部分位于宫颈管内,下端脱出宫颈外口,其形态及回声类型存在相似之处,但瘤体内血流呈散在的短棒状,且未显示蒂部结构。因此,通过上述误诊病例的回顾性分析可以看出,在诊断思路上不能简单以某一个或几个征象进行诊断,需要多个征象综合分析才能提高诊断的准确率。
三维成像以二维图像提供的灰阶信息为基础,二维图像的质量直接影响三维成像效果[9-10]。获得优质三维图像的前提就是改善二维模式下感兴趣区图像的对比度。笔者认为通过以下方法有助于改善二维图像质量:首先,建议选择病人分泌期进行三维检查,此时内膜较厚、回声增强,可与肌层形成良好的对比,有利于显示瘤体边界及宫腔形态;第二,对于瘤体过大且突出宫颈外口者,3D-TVS取样框过大会影响图像质量,可以分段采集;第三,当宫体与宫颈存在过度前倾、后屈时,人为纠正子宫位置,使感兴趣区尽量与声束垂直,改善二维图像质量。本组1例中位子宫,宫体位于远场;1例剖宫产后子宫前壁与腹壁粘连,宫体位置高、移动度差。笔者通过按压腹壁,在改变子宫位置的同时还能排挤肠管气体,二维图像质量得到明显改善,顺利完成三维图像采集。
综上所述,2D-TVS与3D-TVS均能对脱出型黏膜下肌瘤进行诊断,3D-TVS诊断特异度更高。“Ⅰ”形蒂部结构、瘤体内条状血流及蒂部束状血流等特征可以作为诊断的敏感指标,有助于鉴别诊断。三种方法联合将进一步提高脱出型黏膜下肌瘤的超声检出率,具有较高的临床应用价值。
经阴道二维超声、三维容积超声及血流显像在脱出型黏膜下肌瘤诊断中应用价值
Application value of two-dimensional transvaginal ultrasonography, three-dimensional ultrasonography volumetric imaging and three-dimensional Doppler ultrasound in the diagnosis of prolapsed submucosal myoma
-
摘要:
目的探讨经阴道二维超声(2D-TVS)、三维超声(3D-TVS)容积成像及血流显像(3D-DUS)在脱出型黏膜下肌瘤诊断及起始部定位中的价值。 方法临床可疑脱出型黏膜下肌瘤并决定手术治疗病人57例,均行2D-TVS检查,术前再行3D-TVS检查。以手术病理结果为金标准,比较2种方法的诊断准确率。并根据手术结果,将脱出型黏膜下肌瘤病人作为确诊组,非肌瘤性病变病人作为疑似组,比较2组病人的"低回声为主""Ⅰ形蒂部结构"等声像图特点。 结果经手术病理确诊脱出型黏膜下肌瘤34例,宫颈息肉20例,宫颈癌、子宫内膜癌、宫颈肌瘤各1例。2D-TVS和3D-TVS诊断灵敏度分别为88.2%、94.1%,差异无统计学意义(P > 0.05);特异度分别为54.5%、86.4%,3D-TVS特异度高于2D-TVS(P < 0.05);一致性百分率分别为75%、91%。在2D-TVS的低回声为主、"Ⅰ"形蒂部结构、丰富条状血流和3D-TVS的"梨形"团块及3D-DUS的蒂部条束状血流方面,确诊组病人检出率均高于疑似组(P < 0.05~P < 0.01)。 结论2D-TVS与3D-TVS均能检查脱出型黏膜下肌瘤,但后者诊断特异度高于前者;2D-TVS、3D-TVS及3D-DUS显示的瘤体形态及血流的声像图特征可以作为诊断及鉴别诊断指标,提高诊断准确率,减少误诊及漏诊。 Abstract:ObjectiveTo evaluate the application value of two-dimensional transvaginal ultrasonography(2D-TVS), three-dimensional transvaginal ultrasonography(3D-TVS) volumetric imaging and three-dimensional Doppler ultrasound(3D-DUS) in the diagnosis and initial location of submucous myoma of prolapsed type. MethodsFifty-seven patients with suspected prolapsed submucosal myoma deciding on surgical treatment were detected using 2D-TVS and 3D-TVS before operation. Taking the surgery results as golden standard, the diagnostic accuracy was compared between the two methods. According to the surgical results, the patients with protuberant submucosal myoma and patients with non-myomatous disease were divided into the confirmed group and suspected group, respectively. The ultrasonographic characteristics of "low echo" and "Ⅰ shaped pedicle structure" were compared between two groups. ResultsThere were 34 cases of prolapsive submucosal myoma, 20 cases of cervical polyp, 1 case of cervical cancer, 1 case of endometrial cancer and 1 case of cervical myom according to the results of the surgery and pathology. The diagnostic sensitivity of 2D-TVS and 3D-TVS was 88.2% and 94.1%, respectively, and the difference of which was not statistically significant(P > 0.05). The specificity of 2D-TVS and 3D-TVS was 54.5% and 86.4%, respectively, and which of 3D-TVS was higher than that of 2D-TVS(P < 0.05). The percentage of consistency in 2D-TVS and 3D-TVS was 75% and 91%, respectively. In terms of the low echo, "Ⅰ shaped" pedicle structure and rich strip blood flow in 2D-TVS, and pear-shaped" mass of 3D-TVS and strip bundle blood flow of 3D-DUS, the detection rate of which in confirmed group was higher than that in suspected group(P < 0.05 to P < 0.01). Conclusions2D-TVS and 3D-TVS can be used to diagnose the submucous myoma of prolapsed type, and the diagnostic specificity of the 3D-TVS is higher than that of the 2D-TVS. The sonographic characteristics of tumor morphology and blood flow displayed by 2D-TVS, 3D-TVS and 3D-DUS can be used as the diagnostic and differential diagnostic indicators, which can improve the diagnostic accuracy and reduce misdiagnosis and missed diagnosis. -
表 1 2D-TVS与3D-TVS的诊断准确率比较
方法 灵敏度/% 特异度/% 误诊率/% 漏诊率/% Youden指数 一致百分率/% 阳性似然比 阴性似然比 2D-TVS 88.2 54.5 45.5 11.8 0.427 75 1.939 0.217 3D-TVS 94.1 86.4 13.6 5.9 0.805 91 6.919 0.068  下载: 导出CSV
下载: 导出CSV
表 2 特征性声像图在确诊组与疑似组病人中表现比较
特征表现 确诊组
(n=34)疑似组
(n=23)χ2 P 灵敏度/% 特异度/% 2D-TVS 低回声为主 是
否31
315
85.94 < 0.05 91.2 33.3 “Ⅰ”形蒂部结构 是
否26
811
124.94 < 0.05 76.5 52.0 丰富条状血流 是
否31
316
74.43 < 0.05 91.2 30.4 3D-TVS 团块呈“梨形” 是
否19
154
198.44 < 0.01 55.9 83.0 3D-DUS 蒂部条束状血流 是
否26
811
124.94 < 0.05 76.5 52.2
下载: 导出CSV
-
[1] 徐繁华, 张玉娟, 石秋玲, 等. 宫颈管内黏膜下肌瘤的超声诊断价值[J]. 临床超声医学杂志, 2013, 15(6): 418. doi: 10.3969/j.issn.1008-6978.2013.06.024 [2] 周洁莉, 罗红凤, 韩文玲. LEEP术治疗宫颈粘膜下肌瘤的临床研究[J]. 赣南医学院学报, 2013, 33(6): 880. [3] 王翠翠, 宋宁, 马晓欣. 宫颈管内黏膜下肌瘤经阴道摘除术的临床应用[J]. 中国医科大学学报, 2011, 40(7): 658. [4] 钟冬鸾. 宫腔镜治疗子宫黏膜下肌瘤及子宫颈息肉的可行性评估[J/CD]. 实用妇科内分泌电子杂志, 2016, 3(16): 76. [5] 许锋, 顾小燕, 王素敏, 等. 子宫黏膜下肌瘤89例宫腔镜手术效果[J]. 江苏医药, 2018, 44(12): 1431. [6] 焦阳, 范海波, 甘晗靖, 等. 黏膜下肌瘤脱出型的超声诊断及鉴别[J]. 中国妇幼保健, 2013, 28(4): 702. [7] 许锦富, 谢玉珏, 刘佳, 等. 经阴道彩色多普勒超声对带蒂子宫黏膜下肌瘤的诊断意义[J]. 深圳中西医结合杂志, 2015, 25(22): 71. [8] 张丽珍, 毛韧. 经阴道二维超声联合经阴道三维超声对宫腔粘连的诊断价值[J]. 医学影像学杂志, 2016, 26(1): 180. [9] 徐秋栋, 徐丽萍, 王磊, 等. 经阴道三维超声诊断子宫粘膜下肌瘤与肌壁间肌瘤临床分析[J]. 医学影像学杂志, 2016, 26(3): 557. [10] 南凤娟, 张静, 李琪, 等. 三维超声Omniview联合VCI成像技术在黏膜下子宫肌瘤分型中的价值[J]. 医学影像学杂志, 2019, 29(7): 1188. -

 点击查看大图
点击查看大图
图(3)表(2)
计量
- 文章访问数: 3572
- HTML全文浏览量: 1769
- PDF下载量: 5
- 被引次数: 0
