

-
儿童社区获得性肺炎(community acquired pneumonia,CAP)在全球具有较高发病率及死亡率,尤其在5岁以下小儿中发病率最高,是导致其死亡首要原因[1-3]。依照不同感染性病原体所致肺炎特点,分为病毒性肺炎、非典型病原体及细菌性肺炎,有学者[4]对CAP临床特征进行分析发现,细菌性肺炎检出率占41.2%,主要累及肺实质部位,细菌病原菌侵袭肺泡壁、支气管,造成肺泡内充满炎性渗出物,血液中经典炎症标志物如白细胞计数(WBC)、C反应蛋白(CRP)、降钙素原(PCT)发生变化[5-6]。近年来,有学者提出肿瘤坏死因子相关激活蛋白(CD40L)与细菌性肺炎相关,已有研究证实其在肺炎、支气管哮喘等疾病中均有所表达[7-8]。既往临床实践中,血清白细胞介素-4(IL-4)、CD4+/CD8+水平与肺损伤关系研究较多,而与经典炎症标志物的关系研究较少[9-11]。鉴于此,本研究旨在探讨CD40L、CD4+/CD8+、IL-4与儿童细菌性CAP经典炎症标志物的关系及预测抗菌治疗效果的效能,以期为临床诊疗提供参考。现作报道。
-
选取2017年1月至2020年3月我院收治的300例细菌性CAP患儿,其中43例治疗无效(观察组)及257例治疗有效(对照组)。纳入标准:(1)经临床体征、胸部X线片、痰标本培养及血常规检查等证实为细菌性肺炎;(2)年龄1~12岁;(3)符合《社区获得性肺炎中西医综合治疗指南(2015年上海市基层版)》相关诊断标准[12];(4)均可遵循医嘱完成相关检查、治疗。排除标准:(1)伴血液系统疾病者;(2)非细菌性肺炎者、合并其他病原菌性肺炎者;(3)多器官功能障碍;(4)伴免疫系统疾病者;(5)合并支气管哮喘、支气管炎、肺结核及支气管异物等其他肺部疾病者;(6)严重肝肾功能异常及伴有明显精神异常者;(7)呼吸道畸形者;(8)合并肺寄生虫病、营养不良者;(9)既往患有免疫缺陷疾病;(10)未能遵医嘱完成相关检查、治疗或检查过程中伴有严重并发症者。本研究经我院医学伦理委员会批准,入组者均为自愿参加,由监护人签署知情同意书。
-
收集细菌性CAP患儿年龄、发病至入院时间、住院时间、病情程度、体质量、性别、病原菌类型等临床资料。
-
所有入选对象均给予吸氧、化痰、止咳、平喘等对症治疗,并根据药敏试验结果积极给予敏感抗菌药物抗感染治疗。治疗1周后患儿咳嗽、发热等临床症状及肺部啰音等阳性体征完全消失,WBC计数恢复至(5.0~12.0)×109/L为显效;临床症状、体征明显改善,WBC计数趋于(5.0~12.0)×109/L为好转;临床症状、体征及WBC计数无显著改善,甚至加重为无效[13]。显效、好转纳入治疗有效,300例儿童细菌性CAP患儿,其中43例治疗无效(观察组)及257例治疗有效(对照组)。
-
治疗前采集2组患儿空腹静脉血5 mL,选用低温离心机,以转速3500r/min、半径8cm,进行离心分离10 min,DTA-K2抗凝静脉血用于流式细胞仪检测,含分离胶试管分离血清用于WBC、CRP、PCT、IL-4检测。
-
采用FACSCalibur全自动流式细胞分析仪,定量检测外周血T淋巴细胞亚群。于试管中加入混匀全血50μL,后加入CD40L、CD4+/CD8+联合抗体5μL,涡旋混匀后静置15min,于试管中加入2mL的1×溶血素静置7 min,于试管中加入2mL的PBS缓冲液,离心5min,倒去上清液,再加入2mL的PBS缓冲液,再次离心5min,管底剩余液体涡旋混匀加PBS缓冲液0.5 mL,即可上机检测CD40L、CD4+/CD8+水平。流式细胞仪和试剂盒均购买自美国Coulter公司,型号为EpicsXL型。
-
取血清,采用免疫比浊法测定血清CRP水平,试剂盒购自上海江莱生物科技有限公司;采用双抗夹心免疫化学发光法检测血清PCT水平,试剂盒购自南京森贝伽生物科技有限公司;采用ELISA法检测血清IL-4水平,试剂盒购自北京百奥莱博科技有限公司;采用ADVIA70全自动血细胞分析仪(德国拜耳公司)及配套试剂盒检测WBC水平,由同一位具有丰富检验经验医师严格按照仪器及试剂盒说明书完成操作流程。
-
评估项目包括一般情况、意识障碍、低氧血症、发热、脱水症。重度者:一般情况差、有意识障碍、伴有低氧血症(发绀、氧饱和度 < 92%、间歇性呼吸暂停、呻吟、鼻扇、三凹征、呼吸增快呼吸频率>50次/分)、伴有发热(超高热、持续高热>5 d)、有脱水症;轻度者:一般情况好、无意识障碍、无低氧血症、伴有发热但未达重度标准,无脱水征。
-
(1) 比较2组经典炎症标志物水平。(2)比较2组CD40L、CD4+/CD8+、IL-4水平。(3)分析CD40L、CD4+/CD8+、IL-4与经典炎症标志物的关系。(4)CD40L、CD4+/CD8+、IL-4与疗效logistic回归方程分析。(5)分析CD40L、CD4+/CD8+、IL-4之间的关系。(6)CD40L、CD4+/CD8+、IL-4预测抗菌治疗效果的受试者工作特征(ROC)曲线。
-
采用单因素方差分析和q检验、t检验、Pearson相关分析、ROC曲线分析、DeLong检验、logistic二元回归拟合和返回预测概率logit(p)。
-
2组间年龄、发病至入院时间、体质量、性别、病原菌类型比较,差异均无统计学意义(P>0.05);观察组住院时间长于对照组(P < 0.01),病情程度重于对照组(P < 0.01),WBC、CRP与PCT水平均高于对照组(P < 0.01)(见表 1)。
变量 观察组(n=43) 对照组(n=257) t P 年龄/岁 6.44±2.65 6.51±2.70 0.16 >0.05 发病至入院时间/d 2.45±0.52 2.52±0.47 0.89 >0.05 体质量/kg 20.45±7.19 20.62±7.03 0.15 >0.05 性别 男
女25
18132
1250.68* >0.05 病原菌类型 肺炎链球菌 12 73 0.37* >0.05 铜绿假单胞菌 4 24 金黄色葡萄球菌 8 42 流感嗜血杆菌 9 40 肺炎克雷伯杆菌 10 78 住院时间/d 12.47±4.25 5.86±2.33 14.94 < 0.01 病情程度 轻度
重度23
20215
4220.45* < 0.01 经典炎症标志物 WBC/(×109/L) 16.98±4.07 12.55±3.89 6.87 < 0.01 CRP/(mg/L) 35.64±10.29 24.18±8.65 7.82 < 0.01 PCT/(μg/L) 2.36±0.54 1.22±0.41 16.07 < 0.01 *示χ2值 表 1 一般资料及经典炎症标志物水平比较(x±s)
-
观察组CD40L与IL-4水平均高于对照组,CD4+/CD8+低于对照组(P < 0.01)(见表 2)。
分组 n CD40L/(ng/mL) CD4+/CD8+ IL-4/(pg/mL) 观察组 43 3.19±0.52 0.86±0.27 19.55±5.68 对照组 257 2.47±0.49 1.03±0.35 10.16±4.37 t — 8.84 3.04 12.45 P — < 0.01 < 0.01 < 0.01 表 2 2组CD40L、CD4+/CD8+、IL-4水平比较(x±s)
-
CD40L与WBC(r=0.720,P < 0.01)、CRP(r=0.433,P < 0.01)、PCT(r=0.832,P < 0.01)呈正相关;CD4+/CD8+与WBC(r=-0.709,P < 0.01)、CRP(r=-0.449,P < 0.01)、PCT(r=-0.698,P < 0.01)呈负相关;IL-4与WBC(r=0.889,P < 0.01)、CRP(r=0.760,P < 0.01)、PCT(r=0.723,P < 0.01)呈正相关。
-
CD40L、CD4+/CD8+、IL-4均与治疗无效相关,具有统计学意义(P < 0.01)(见表 3)。
影响因素 B SE Waldχ2 P OR 95%CI CD40L 0.231 0.085 7.41 < 0.01 1.260 1.146~1.386 CD4+/CD8+ -1.815 0.512 12.56 < 0.01 0.163 0.132~0.201 IL-4 1.351 0.326 17.18 < 0.01 3.861 2.897~5.147 表 3 CD40L、CD4+/CD8+、IL-4与治疗无效的logistic回归方程分析
-
CD40L与CD4+/CD8+呈负相关(r=-0.776,P < 0.01),与IL-4呈正相关(r=0.554,P < 0.01);CD4+/CD8+与IL-4呈负相关(r=-0.538,P < 0.01)。
-
绘制CD40L、CD4+/CD8+、IL-4预测抗菌治疗效果(无效)的ROC,发现单一指标中IL-4预测抗菌治疗效果的曲线下面积(AUC)最大(0.805),各指标联合预测抗菌治疗效果的AUC为0.867,大于任一单一指标(P < 0.01)(见图 1、表 4)。
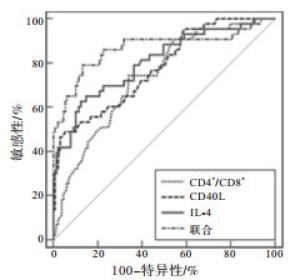
图 1 CD40L、CD4+/CD8+、IL-4预测无效的ROC分析
指标 AUC 95%CI Z P 截断值 敏感度/% 特异度/% CD40L 0.779 0.698~0.859 6.78 < 0.01 >3.15 ng/mL 48.84 94.57 CD4+/CD8+ 0.737 0.654~0.819 5.64 < 0.01 ≤0.97 74.42 65.89 IL-4 0.805 0.725~0.886 7.45 < 0.01 >16.42 pg/mL 65.12 85.27 联合 0.867 0.789~0.945 9.22 < 0.01 — 79.07 86.82 表 4 各指标预测无效的ROC分析结果
-
近年来儿童细菌性CAP发生率呈逐渐上升趋势,巨大疾病负担已构成全球公共卫生问题,成为临床研究热点之一[14-15]。评估儿童细菌性CAP抗菌治疗效果在CAP诊治中极其重要,近年来越来越多学者将生物标志物水平作为判断抗菌治疗效果的指标。
WBC、CRP、PCT为临床评价感染性疾病经典炎症标志物,近些年来,研究者尝试应用PCT区分细菌性感染、非细菌性感染,国外研究[16]发现,PCT与肺炎严重程度密切关联,PCT水平同CAP严重程度及预后具有显著相关性。CRP为急性时相反应蛋白,感染存在时由炎性淋巴因子刺激上皮细胞和肝脏产生,有学者研究[17]发现,CRP水平波动还同非感染性疾病相关,如冠心病、脑梗死、恶性肿瘤等,故其特异性并不高。WBC作为评估炎症存在指标,临床普遍认为其为初步判断病毒感染、细菌感染的常规鉴别诊断指标,结合其他感染指标(如CRP、PCT)综合分析对细菌感染性肺炎患儿诊断具有良好临床价值[18]。本研究结果显示,观察组WBC、CRP、PCT高于对照组(P < 0.01),提示治疗前检测血清WBC、CRP、PCT能为临床评估患儿病情提供更多依据,有利于制定更为精准的治疗方案。另有研究[19]证实,不同病原感染CAP患儿临床特征各异,相同病原感染后疾病进展及转归亦存在差异,目前儿童细菌性CAP抗菌治疗效果研究重点除经典炎症标志物外,探究参与调控的炎症因子及相关因子激活蛋白在儿童细菌性CAP反应中的应用逐渐引起关注。
CD40L是在NK细胞、活化T淋巴细胞及其他细胞上表达的跨膜糖蛋白,主要调节机体细胞免疫、体液免疫应答过程中的炎症反应,CD40L同CD40结合后可激活T细胞参与炎症反应[20]。本研究数据显示,观察组CD40L水平较对照组高,与卞相丽等[21]研究结果一致。这可能与CD40L与CD40作为一对协同刺激因子,在细菌性CAP治疗无效患儿体内可引起机体炎性反应发生有关。李艳霞等[22]研究证实,IL-4理化特性、生物学效应同儿童呼吸系统炎症性疾病密切相关。本研究指出,细菌性CAP治疗无效患儿IL-4呈高表达水平,与陈萍等[23]研究结果基本一致,考虑其原因,IL-4作为Th2细胞的特征细胞因子,在Th2细胞活化后产生,能够刺激B细胞增殖,介导机体免疫应答产生,Th1亚群平衡失调,加重机体炎症发生趋势。范芸等[24]对不同类型肺炎患儿外周血T细胞免疫指标进行检测发现,细菌性肺炎重症患儿外周血中CD4+/CD8+低于健康儿童。本研究数据显示,观察组CD4+/CD8+低于对照组(P < 0.01),CD4+/CD8+为人体内环境稳定重要指标,其比值降低提示细菌性CAP治疗无效患儿细胞免疫受到抑制,比例失衡引发机体免疫功能紊乱。本研究经相关性分析发现,细菌性CAP患儿WBC、CRP、PCT水平与CD40L、IL-4间存在正相关关系,与CD4+/CD8+间存在负相关关系,提示CD40L、IL-4、CD4+/CD8+可在一定程度上反映细菌性CAP患儿治疗效果、肺组织损伤程度。
儿童细菌性CAP本质上为慢性呼吸道炎症疾病,治疗效果受多个方面因素影响,免疫紊乱为影响患儿治疗效果关键环节[25]。我们通过logistic回归方程分析发现,CD40L、CD4+/CD8+、IL-4均与治疗无效显著相关,因此,我们推测可通过检测CD40L、CD4+/CD8+、IL-4水平可能辅助临床评估儿童细菌性CAP抗菌治疗效果。进一步分析CD40L、CD4+/CD8+、IL-4之间的关系,CD40L与CD4+/CD8+呈负相关,CD40L与IL-4呈正相关,CD4+/CD8+与IL-4呈负相关,推测其原因:(1)细菌具有荚膜结构,具有抗吞噬、抗体液免疫及内化作用,于患儿体内增殖、释放内毒素脂多糖等物质,激活机体CD40-CD40L系统信号分子,参与调节机体免疫,致使T细胞亚群变化,常见的包括CD4+、CD8+、CD3+、CD19+等,CD4+减少致使机体逐渐丧失对于抗原的免疫反应,感染肺组织中CD4+减少,不利于CD8+细胞进一步扩增,对细菌监控、杀伤能力下降。(2)可能与肺炎链球菌、流感嗜血杆菌等作用于中性粒细胞有关,通过激活CD40L,进而释放大量细胞因子,直接参与炎症发生发展,促进炎症因子IL-4释放,并随着感染加重不断升高,致使疾病治疗难度增加[26]。(3)细菌性感染发生后,可黏附于气道黏膜表面,促使气道上皮细胞变性、坏死,诱发机体免疫反应过度表达,CD4+/CD8+反映机体免疫功能,其水平低下,造成机体呼吸系统防御脆弱,内部炎症因子过度释放,IL-4表达水平升高[27]。本研究将三者用于预测儿童细菌性CAP抗菌治疗效果,结果显示,单一指标中IL-4预测抗菌治疗效果的AUC最大在0.805,具有较高预测价值。但儿童细菌性CAP致病机制复杂,需结合多个指标综合评价治疗效果及预后[28]。CD4+/CD8+、IL-4、CD40L联合预测抗菌治疗效果的AUC为0.867,敏感度达79.07%,大于任一单一指标,能够提高抗菌治疗效果预测效能,为临床评估疾病转归提供更加准确数据支持,且多种生物标志物水平联合检测能够更加全面评估患儿治疗效果,对指导临床更加合理地开展治疗措施具有积极作用。但本研究未详细探究其他病原菌肺炎患儿血清CD40L、CD4+/CD8+、IL-4水平,对此还需作进一步分析与探究,以获取更为全面的数据支持。
综上,WBC、CRP、PCT、CD40L、IL-4在细菌性CAP治疗无效患儿中表达水平明显升高,CD4+/CD8+表达明显降低,CD40L、IL-4、CD4+/CD8+与经典炎症标志物存在一定相关性,可在一定程度上反应细菌性CAP患儿病情程度,及早预测细菌性CAP患儿抗菌治疗效果,对临床判断细菌性CAP患儿治疗效果及预后具有指导意义。
肿瘤坏死因子相关激活蛋白、CD4+/CD8+、IL-4与儿童细菌性社区获得性肺炎经典炎症标志物的关系研究
Relationship between CD40L, CD4+/CD8+, IL-4 and the classic inflammation biomarkers for bacterial pediatric community acquired pneumonia and the predictive performance in antibacterial therapy
-
摘要:
目的探讨肿瘤坏死因子相关激活蛋白(CD40L)、CD4+/CD8+、白细胞介素-4(IL-4)与儿童细菌性社区获得性肺炎(CAP)经典炎症标志物的关系及预测抗菌治疗效果的效能。 方法选取300例儿童细菌性CAP患儿,均给予化痰、止咳、平喘及抗感染治疗, 其中43例治疗无效(观察组)及257例治疗有效(对照组),比较2组治疗前白细胞计数(WBC)、C反应蛋白(CRP)、降钙素原(PCT)及CD40L、CD4+/CD8+、IL-4,采用Pearson分析CD40L、CD4+/CD8+、IL-4与经典炎症标志物的关系及CD40L、CD4+/CD8+、IL-4之间的关系,采用logistic回归方程分析CD40L、CD4+/CD8+、IL-4与治疗无效的关系,采用受试者工作特征曲线(ROC)及ROC下面积(AUC)分析CD40L、CD4+/CD8+、IL-4预测抗菌治疗效果的效能。 结果观察组WBC、CRP、PCT、CD40L、IL-4水平均高于对照组(P < 0.01),CD4+/CD8+低于对照组(P < 0.01);CD40L与WBC、CRP、PCT均呈正相关(r=0.720、0.433、0.832,P < 0.01),CD4+/CD8+与WBC、CRP、PCT呈负相关(r=-0.709、-0.449、-0.698,P < 0.01),IL-4与WBC、CRP、PCT呈正相关(r=0.889、0.760、0.723,P < 0.01);CD40L、CD4+/CD8+、IL-4均与治疗无效的相关性具有统计学意义(P < 0.01);CD40L与CD4+/CD8+呈负相关(r=-0.776,P < 0.01),与IL-4呈正相关(r=0.554,P < 0.01);CD4+/CD8+与IL-4呈负相关(r=-0.538,P < 0.01);单一指标中IL-4预测抗菌治疗效果的AUC最大为0.805,各指标联合预测抗菌治疗效果的AUC为0.867,敏感度达79.07%,大于任一单一指标(P < 0.01)。 结论CD40L、IL-4、CD4+/CD8+与经典炎症标志物存在一定相关性,可在一定程度上反映细菌性CAP患儿病情程度,治疗期间进行动态监测可及早预测疗效,为细菌性CAP患儿后续治疗提供参考依据。 -
关键词:
- 社区获得性肺炎 /
- 肿瘤坏死因子相关激活蛋白 /
- 白细胞介素-4 /
- 炎症标志物
Abstract:ObjectiveTo investigate the relationship between tumor necrosis factor-related activator protein(CD40L), CD4+/CD8+, interleukin-4(IL-4) and classic inflammatory biomarkers of bacterial pediatric community acquired pneumonia(CAP) and the predictive efficacy in antibacterial therapy. MethodsA total of 300 children with bacterial CAP were selected for treatment of phlegm removing, cough relieving, asthma reducing and anti-infection.The non-response cases were set as observation group(n=43) and the improved cases were set as control group(n=257).The white blood cell count(WBC), C-reactive protein(CRP), procalcitonin(PCT), CD40L, CD4+/CD8+ and IL-4 were detected before treatment.Pearson correlation analysis was used to analyze the relationship between CD40L, CD4+/CD8+, IL-4 and classic inflammation markers and the relationship between CD40L, CD4+/CD8+, IL-4.The logistic regression equation was used to analyze the relationship between CD40L, CD4+/CD8+, IL-4 and non-response treatment.The receiver operating characteristic(ROC) curve and the area under the ROC cure(AUC) were used to analyze the predictive efficacy of CD40L, CD4+/CD8+ and IL-4 of antibacterial treatment. ResultsWBC, CRP, PCT, CD40L and IL-4 in the observation group were higher than those in the control group(P < 0.01) and CD4+/CD8+ was lower than that in the control group(P < 0.01).CD40L was positively correlated with WBC, CRP and PCT(r=0.720, 0.433, 0.832, P < 0.01), CD4+/CD8+ was negatively correlated with WBC, CRP and PCT(r=-0.709, -0.449, -0.698, P < 0.01), IL-4 was positively correlated with WBC, CRP and PCT(r=0.889, 0.760, 0.723, P < 0.01).CD40L, CD4+/CD8+, IL-4 were all significantly correlated with treatment failure(P < 0.01).CD40L was negatively correlated with CD4+/CD8+, and positively correlated with IL-4(r=-0.776, 0.554, P < 0.01).CD4+/CD8+ was negatively correlated with IL-4(r=-0.538, P < 0.01).Among the single indicators, the maximum AUC of IL-4 predicting the effect of antibacterial treatment was 0.805, the AUC of each indicator combined to predict the effect of antibacterial treatment was 0.867, and the sensitivity was 79.07%, which was greater than any single indicator(P < 0.05). ConclusionsThere is a certain correlation between CD40L, IL-4, CD4+/CD8+ and classic inflammatory biomarkers, which can reflect the severity of disease in bacterial pediatric CAP to a certain extent.Dynamic monitoring will provide timely predictive value and better reference for the follow-up treatment of bacterial pediatric CAP. -
表 1 一般资料及经典炎症标志物水平比较(x±s)
变量 观察组(n=43) 对照组(n=257) t P 年龄/岁 6.44±2.65 6.51±2.70 0.16 >0.05 发病至入院时间/d 2.45±0.52 2.52±0.47 0.89 >0.05 体质量/kg 20.45±7.19 20.62±7.03 0.15 >0.05 性别 男
女25
18132
1250.68* >0.05 病原菌类型 肺炎链球菌 12 73 0.37* >0.05 铜绿假单胞菌 4 24 金黄色葡萄球菌 8 42 流感嗜血杆菌 9 40 肺炎克雷伯杆菌 10 78 住院时间/d 12.47±4.25 5.86±2.33 14.94 < 0.01 病情程度 轻度
重度23
20215
4220.45* < 0.01 经典炎症标志物 WBC/(×109/L) 16.98±4.07 12.55±3.89 6.87 < 0.01 CRP/(mg/L) 35.64±10.29 24.18±8.65 7.82 < 0.01 PCT/(μg/L) 2.36±0.54 1.22±0.41 16.07 < 0.01 *示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 2组CD40L、CD4+/CD8+、IL-4水平比较(x±s)
分组 n CD40L/(ng/mL) CD4+/CD8+ IL-4/(pg/mL) 观察组 43 3.19±0.52 0.86±0.27 19.55±5.68 对照组 257 2.47±0.49 1.03±0.35 10.16±4.37 t — 8.84 3.04 12.45 P — < 0.01 < 0.01 < 0.01
下载: 导出CSV
表 3 CD40L、CD4+/CD8+、IL-4与治疗无效的logistic回归方程分析
影响因素 B SE Waldχ2 P OR 95%CI CD40L 0.231 0.085 7.41 < 0.01 1.260 1.146~1.386 CD4+/CD8+ -1.815 0.512 12.56 < 0.01 0.163 0.132~0.201 IL-4 1.351 0.326 17.18 < 0.01 3.861 2.897~5.147
下载: 导出CSV
表 4 各指标预测无效的ROC分析结果
指标 AUC 95%CI Z P 截断值 敏感度/% 特异度/% CD40L 0.779 0.698~0.859 6.78 < 0.01 >3.15 ng/mL 48.84 94.57 CD4+/CD8+ 0.737 0.654~0.819 5.64 < 0.01 ≤0.97 74.42 65.89 IL-4 0.805 0.725~0.886 7.45 < 0.01 >16.42 pg/mL 65.12 85.27 联合 0.867 0.789~0.945 9.22 < 0.01 — 79.07 86.82
下载: 导出CSV
-
[1] LANKS CW, MUSANI AI, HSIA DW. Community-acquired pneumonia and hospital-acquired pneumonia[J]. Med Clin North Am, 2019, 103(3): 487. doi: 10.1016/j.mcna.2018.12.008 [2] 宁桂军, 王旭霞, 刘世文, 等. 2015-2016年甘肃省白银市5岁以下儿童社区获得性肺炎疾病负担回顾性调查[J]. 中国疫苗和免疫, 2017, 23(1): 18. [3] ANDRONIKOU S, GOUSSARD P, SORANTIN E. Computed tomography in children with community-acquired pneumonia[J]. Pediatr Radiol, 2017, 47(11): 143. [4] 唐晓燕. 儿童社区获得性肺炎临床特征分析[D]. 新乡: 新乡医学院, 2016. [5] 陈金锦, 朱光明, 车惠琴, 等. 儿童社区获得性肺炎流行病学特点及血清降钙素原水平临床分析[J]. 中国卫生检验杂志, 2018, 28(4): 478. [6] CECCATO A, FERRER M, BARBETA E, et al. Adjunctive therapies for community-acquired pneumonia[J]. Clin Chest Med, 2018, 39(4): 753. doi: 10.1016/j.ccm.2018.07.008 [7] 王月红, 张娅杰, 谷强. 肺炎支原体感染的哮喘患儿血清CD40L、VCAM-1水平变化及其意义[J]. 山东医药, 2017, 57(46): 78. doi: 10.3969/j.issn.1002-266X.2017.46.024 [8] 孙磊, 刘奉琴, 赵鹏鹏. 血清CD40L, VCAM-1表达与儿童细菌性肺炎严重程度的相关性[J]. 广东医学, 2019, 40(17): 2495. [9] MEDJO B, ATANASKOVIC-MARKOVIC M, NIKOLIC D, et al. Increased serum interleukin-10 but not interleukin-4 level in children with mycoplasma pneumoniae pneumonia[J]. J Trop Pediatr, 2017, 63(4): 294. [10] 郭孝红, 胡玉杰, 李俊梅, 等. 儿童难治性肺炎支原体肺炎的临床特点及血清IL-4、IL-6、IL-10、IFN-γ的变化分析[J]. 现代生物医学进展, 2018, 18(24), 4768. [11] 赵庆鹏, 韩广强, 赵庆珍. 小儿支原体肺炎合并肝功损害与心肌功能, CD4+/CD8+的关系及甘草酸苷的效用[J]. 西北药学杂志, 2019, 34(6): 818. doi: 10.3969/j.issn.1004-2407.2019.06.025 [12] 上海市中西医结合学会急救专业委员会, 中国呼吸科专家组(统称). 社区获得性肺炎中西医综合治疗指南(2015年上海市基层版)[J]. 上海中医药杂志, 2016, 50(7): 15. [13] 中华医学会儿科学分会呼吸组. 儿童社区获得性肺炎管理指南(2013修订)(上)[J]. 中华儿科杂志, 2013, 51(10): 745. doi: 10.3760/cma.j.issn.0578-1310.2013.10.006 [14] 许莉, 王仁媛. 海口市6~12岁儿童肺炎支原体感染的流行病学特征及健康教育效果[J]. 中国妇幼保健, 2018, 33(13): 3017. [15] 许沙沙, 郭连峰, 吴妍, 等. 儿童肺炎支原体肺炎临床特征和流行病学分析[J]. 中华医院感染学杂志, 2017, 27(14): 3307. [16] GUO S, MAO X, LIANG M. The moderate predictive value of serial serum CRP and PCT levels for the prognosis of hospitalized community-acquired pneumonia[J]. Respir Res, 2018, 19(1): 193. doi: 10.1186/s12931-018-0877-x [17] 庄金宝, 刘天明, 刘彩红, 等. 不同肺炎患儿降钙素原、超敏C反应蛋白及T细胞亚群变化的临床意义[J]. 中国实验诊断学, 2018, 22(11): 1960. doi: 10.3969/j.issn.1007-4287.2018.11.029 [18] 黎艺. PCT、CRP和WBC计数在小儿感染性肺炎诊断中的应用研究[J]. 临床医学工程, 2019, 26(4): 4890. [19] 夏厚才, 彭惠轩, 罗小兵, 等. 广州市南沙区儿童社区获得性肺炎病原调查及临床特点分析[J]. 中国实用医药, 2017, 12(20): 6. [20] 张铷涓, 程安春, 汪铭书. CD40/CD40L在抗病毒免疫应答过程中的作用[J]. 细胞与分子免疫学杂志, 2018, 34(1): 90. [21] 卞相丽, 国志, 张金萍. 肺炎支原体感染的哮喘患儿发病中血清CD40L、VCAM-1水平的意义[J]. 实用药物与临床, 2018, 21(4): 395. [22] 李艳霞, 柴燕玲. γ干扰素和白介素-4的特点及其在慢性阻塞性肺疾病发病过程中的作用[J]. 临床肺科杂志, 2019, 24(6): 1139. doi: 10.3969/j.issn.1009-6663.2019.06.045 [23] 陈萍, 夏训和. 匹多莫德辅助治疗细菌感染性肺炎的疗效及其对患儿血清炎性因子和Th1/Th2细胞因子的影响[J]. 海南医学, 2019, 30(5): 566. doi: 10.3969/j.issn.1003-6350.2019.05.007 [24] 范芸, 归巧娣, 施瑞洁, 等. 不同类型肺炎患儿血清hs-CRP和PCT及部分外周血T细胞免疫指标的变化[J]. 贵州医科大学学报, 2020, 45(1): 108. [25] MÉNDEZ R, MENÉNDEZ R, AMARA-ELORI I, et al. Lymphopenic community-acquired pneumonia is associated with a dysregulated immune response and increased severity and mortality[J]. J Infect, 2019, 78(6): 423. doi: 10.1016/j.jinf.2019.04.006 [26] 唐国英, 张连花. 儿童细菌性肺炎患儿血清CD40L, VCAM-1表达变化与其疾病严重程度相关关系研究[J]. 临床肺科杂志, 2019, 24(5): 827. doi: 10.3969/j.issn.1009-6663.2019.05.013 [27] 冯雪, 田庆玲, 张双, 等. 儿童社区获得性肺炎病原体分析及对患儿T细胞水平的影响[J]. 中国免疫学杂志, 2019, 35(3): 104. [28] 甘文磊, 黄静, 朱家馨, 等. 血清中五种炎症标志物在社区获得性肺炎感染与危重度评估中的价值[J]. 结核病与肺部健康杂志, 2017, 6(1): 41. -

 点击查看大图
点击查看大图

图(1)表(4)
计量
- 文章访问数: 2859
- HTML全文浏览量: 1556
- PDF下载量: 20
- 被引次数: 0
