



-
前列腺癌位居世界男性肿瘤疾病谱前列,影响着男性的生活质量[1]。我国的肿瘤监测数据[2-3]显示,前列腺癌位列我国肿瘤发病谱第7位和肿瘤死因谱第12位。前列腺癌早期临床表现不明显,多数病人就诊时已至中晚期。因此,对中晚期前列腺癌的治疗提出更高的临床需求。T3期前列腺癌属于局部晚期的一种,分为T3a期和T3b期,T3a期代表前列腺包膜切缘阳性,T3b期则表示病灶突破包膜至精囊。多参数MRI(multi-parameter MRI,mp-MRI)对前列腺疾病的诊断具有重要的参考价值[4-5],但对 < 1 mm的病灶检查效果不够理想。由于前列腺包膜与精囊在解剖上位置较接近,很难精确地在MRI图像上判断精囊是否被侵及。本研究引入影像组学技术,提取T2WI及ADC图像下T3a和T3b期前列腺癌病灶的影像组学特征,探究mp-MRI影像组学在鉴别诊断T3a、T3b期前列腺癌中的价值。
-
回顾性分析2017年6月至2020年7月于蚌埠医学院第一附属医院因怀疑前列腺癌而行MR扫描的302例病人的影像资料,其中256例经手术后组织病理学证实为前列腺癌,并获得病理分期,筛选出T3期病人151例。纳入标准: (1)mp-MRI在术前4个月内完成;(2)前列腺mp-MRI检查按PI-RADS v2标准[6]常规进行;(3)所有病人均经手术后组织病理学证实并获得病理分期;(4)无MRI检查禁忌证,检查前签署知情同意书。排除标准: (1)术前新辅助治疗;(2)有凝血障碍、感染性疾病、严重心脑血管疾病的病人;(3)在一周内接受直肠指诊和导尿的病人;(4)病灶显示欠佳,不能准确勾画感兴趣区(regions of interest, ROI);(5)病灶的病理诊断取样部位与T2WI图像位置不匹配。依照病理结果,将151例病人分为T3a组110例和T3b组41例。
-
采用Philips Achieva 3.0T TX MR成像仪,16通道腹部相控阵线圈进行扫描。通过Extended MR Work Space后处理工作站,由b=800 s/mm2图像自动重建出ADC图。
扫描前告知病人检查流程及方式,包括检查前适度充盈膀胱,检查时取仰卧位,足先进,适度呼吸等。扫描内容按PI-RADS v2标准[6]常规进行。包括横轴位T1WI(TR 674 ms,TE 20 ms;层厚4.0 mm;层间距0;FOV=260 mm×260 mm);T2WI(TR 4 682 ms,TE 100 ms);DWI序列b值选用0、800 s/mm2(TR 3 000 ms,TE 56 ms)。扫描序列还包括矢状位及冠状位T1WI、T2WI。
-
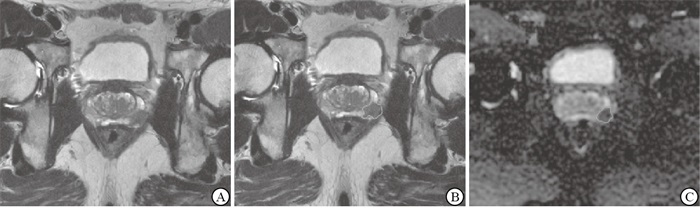
两名经PI-RADS v2培训后的医师在双盲条件下对T2WI及ADC图像上前列腺癌病灶进行分割,当意见不统一时经协商得出结论。勾画时选取病灶最大层面,共得到302个目标区域(见图 1、2)。

图 1 病人男,75岁,T3a期前列腺癌

图 2 病人男,64岁,T3b期前列腺癌
利用达尔文智能科研平台(http://www.yizhun-ai.com),从每个病灶中自动提取基于mp-MRI的影像学特征并筛选。筛选按照以下顺序进行:(1)最大最小值归一化:将每个特征缩放至[1]范围并预筛。(2)方差分析:计算预筛特征与T3a和T3b的线性相关性,相关性以F表示,并对所有F值进行排序,保留前100个特征;(3)利用LASSO算法对特征进行自动筛选。
-
采用分层抽样方法,将ADC图像、T2WI图像、ADC图像联合T2WI图像三种模式下的影像组学特征资料分为两个独立的数据集,即训练集和验证集,其比率为3∶1,既保持了两个数据集中数据分布的一致性,又避免了在数据处理过程中引入额外偏差而对最终结果产生影响。由于本研究中T3a期前列腺癌和T3b期前列腺癌的数量不平衡。因此,我们创建了10个随机试验来评估现有模型的稳定性。分类器通过支持向量机(support-vector machine,SVM)评估特征的重要性,并去除每个训练集末尾的特征,保留最优子集,直至分类性能下降或达到最小特征数。利用剩余特征进行五折交叉验证,并以网格搜索的方式搜索最优的SVM模型参数。
-
采用t检验、秩和检验和ROC曲线分析。
-
本研究共纳入病例151例,训练集113例,其中T3a期82例,T3b期31例;验证集38例,其中T3a期28例,T3b期10例。训练集与验证集年龄、前列腺特异抗原(PSA)水平差异均无统计学意义(P>0.05)(见表 1)。
分组 n 年龄/岁 PSA/(ng/mL) 训练集 113 69.2±6.9 26.0(24.2) 验证集 38 68.6±7.5 22.5(12.4) t — 0.45 1.05 P — >0.05 >0.05 表 1 训练集与验证集一般资料比较(x±s)
-
通过DARWIN智能科研平台在T2WI及ADC图像上共提取影像组学特征1 878个。通过最大最小值归一化、方差分析及SVM对特征进行筛选,得到最优的6个特征。将6个影像组学特征纳入组学模型,其中包括2个ADC图像特征,4个T2WI图像特征(见图 3)。

图 3 DARWIN智能科研平台筛选影像组学特征
-
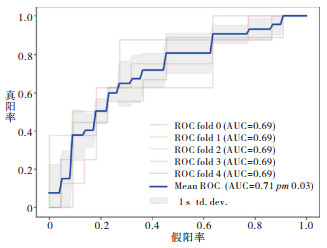
通过ADC图像和T2WI图像提取影像组学特征所建模型效能相对较低,训练集AUC值分别为0.71、0.79;验证集AUC值分别为0.70、0.59。通过ADC联合T2WI图像提取影像组学特征所建模型鉴别性能最优,训练集AUC值为0.79,验证集AUC值为0.73(见表 2)。使用SVM进行五折交叉验证最优模型,结果显示ADC联合T2WI图像影像组学模型校准度良好(见图 4)。
模型 训练集 验证集 AUC(95%CI) 敏感性/% 特异性/% 准确性/% AUC(95%CI) 敏感性/% 特异性/% 准确性/% ADC 0.71(0.55~0.87) 61.3 80.5 78.8 0.70(0.40~0.96) 90.0 60.7 68.4 T2WI 0.79(0.66~0.92) 80.6 65.9 72.6 0.59(0.30~0.89) 90.0 53.6 73.7 ADC+T2WI 0.79(0.64~0.95) 61.3 96.3 81.4 0.73(0.47~1.00) 80.0 67.9 76.3 表 2 3种模型在训练集和验证集中的统计学参数

图 4 ADC联合T2WI图像影像组学模型五折交叉验证
-
泌尿生殖系统肿瘤谱中,前列腺癌位居前列[7],严重影响着男性的身体及心理健康。由于前列腺癌早期临床表现较少,常被病人忽略,尽管近年来PSA筛查已广泛的在临床应用,但仍有很多病人就诊时已进入中晚期,甚至远处转移。本研究所收集256例病人中,中晚期达151例,占一半以上,亦从另一角度证明临床中晚期前列腺癌病人数量较其他期数多。因此,对中晚期前列腺癌的治疗提出更高的临床需要。
前列腺癌的治疗方式包括根治性切除术、放射治疗、内分泌治疗、化学治疗及联合治疗等[8],不同病理分期所使用的治疗方式各不相同。T1及T2期病灶局限于前列腺内,T4期病灶远处转移。传统观点认为T1、T2期肿瘤适用根治性切除术,T4期病人一般以姑息治疗,如去势治疗为主[9]。不同于局限在前列腺包膜内的T1、T2期前列腺癌,也异于远处转移的T4期前列腺癌,T3期前列腺癌属于局部晚期的一种。传统观点将此期的治疗方式划分至姑息治疗,随着对盆底解剖结构的研究及临床治疗方式的进步与发展,根治性切除术在T3a期使用的越来越广泛,常见方案为根治性切除术联合放射治疗及内分泌治疗[10]。2018年EAU指南将局部晚期前列腺癌采取根治性切除术的推荐等级由2014年的推荐修改为强烈推荐。同时,越来越多的研究证明对T3期病人进行根治性切除术并联合放射治疗或内分泌治疗等辅助治疗能够延长预期寿命,降低生化复发率。如SCHULMAN等[11]对T3期病人采用根治切除术联合放射治疗,结果表明该治疗方式可延长病人生化无进展生存率。MAKAREWICZ等[12]对431例T3期前列腺癌病人采用根治切除术联合放射治疗,结果同样显示联合治疗组生化复发率低于单独放射治疗组。T3期分为T3a和T3b,T3a代表病灶突破前列腺包膜但未侵犯精囊,T3b则表示病灶突破包膜至精囊。根治性切除术前了解是否侵犯精囊,有助于手术方案的制定及精准手术的进行,减少术中出血及术后尿失禁的风险。
mp-MRI具有高分辨、广参数、平面广的优势,可以清晰地显示前列腺的解剖结构、毗邻组织器官的形态及淋巴结转移情况,可用于术前定位、分期及危险度分层[13-14],对前列腺疾病的诊断具有重要的参考价值。但MRI对 < 1 mm的病灶检查效果不够理想,而前列腺包膜与精囊在解剖上位置十分接近,因此很难精确的在MRI图像上判断精囊是否被侵及。影像组学通过计算机软件将医学图像转化为定量的数据信息,实现了影像图像向影像数据转化的可能,可重复、客观的描述病灶的异质性,挖掘人眼无法分辨的图像细节信息,且无需增加扫描,弥补了医师根据影像图像诊断的不足,在前列腺癌的研究中已有大量工作发表。多项研究结果表明,基于T2WI和或DWI的影像组学模型可用于前列腺癌的诊断、危险度评估等,如XU等[15]研究纳入331例病人,结果表明,基于MRI的影像组学的预测模型诊断效能优于基于临床因素的诊断模型。但少有研究探究其在T3期前列腺癌中的应用。
本研究中,通过达尔文智能科研平台对T2WI及ADC图像进行影像组学特征提取、筛选及建模。分别建立ADC图像、T2WI图像、ADC图像联合T2WI图像三种模式下的影像组学模型,结果显示,其中ADC图像模式下的模型诊断效能一般,其AUC值为0.70;T2WI图像模式下的模型诊断效能不够理想,为0.59;ADC图像联合T2WI图像模式下的模型诊断效能较好,AUC值为0.73。ADC图像由弥散加权成像重建得到,弥散加权成像的基础是布朗运动,即水分子的微观流动。水分子存在于组织细胞内,正常组织细胞内水分子由于受到细胞膜的阻隔,扩散受限,方向局限,在DWI上信号不高。而被肿瘤侵犯正常组织结构被肿瘤替代并破坏,随着肿瘤细胞不断地病态分裂,细胞膜破损,其内水分子扩散范围变大,方向不受限,因此,在DWI上呈高信号。ADC直观体现扩散受限的程度,间接提示ROI组织的恶性风险度。前列腺癌病人病灶DWI明显升高,ADC随之减低[16]。ADC联合T2WI影像组学模型良好的诊断效能可在术前为准备采取根治性切除术的临床T3期病人提供更加详实的资料,协助临床医生制定更为精确的手术方案,对MRI在观察 < 1 mm病灶时的局限性有很好的补充作用。
本研究样本量小,还应纳入更多病例,深入研究。此外,所建模型仅进行内部验证,未进行外部验证,模型的普遍适用性无法得到证实。
综上所述,ADC联合T2WI图像模式下的影像组学模型对T3a及T3b期前列腺癌具有一定的鉴别能力,可协助临床术前获得更加详实的资料,为制定更精准的手术方案提供指导。
多参数MRI影像组学在鉴别诊断T3a与T3b期前列腺癌中的价值
Value of multi-parameter MRI-based radiomics in distinguishing T3a stage from T3b stage of prostate cancer
-
摘要:
目的探讨多参数MRI(multi-parameter MRI, mp-MRI)影像组学在鉴别诊断T3a、T3b期前列腺癌中的价值。 方法回顾性分析151例T3期前列腺癌病人的影像资料, 其中T3a期110例, T3b期41例。使用达尔文智能科研平台在T2WI及ADC横轴位图像上手动勾画感兴趣区, 提取影像组学特征。按照3:1的比例分别将ADC图像、T2WI图像、ADC图像联合T2WI图像三种模式下的影像组学特征分为训练集和验证集, 依次对3组训练集构建模型, 使用相应验证集进行内部验证。通过ROC曲线对模型进行分析, 并评价不同序列的诊断效能。 结果通过达尔文科研平台共提取1878个影像组学特征, 最终保留6个(ADC相关2个, T2WI相关4个)(P < 0.05), 单独T2WI和ADC图像下训练集AUC值分别为0.79、0.71, 验证集AUC值为0.59、0.70;ADC图像联合T2WI图像下训练集AUC值为0.79, 验证集AUC值为0.73。 结论T2WI图像联合ADC图像影像组学对术前鉴别T3a、T3b期前列腺癌具有较好诊断价值, 可在一定程度上弥补MRI对 < 1 mm病灶检查效果欠佳的缺陷, 为癌灶是否侵犯精囊提供补充, 协助临床术前获得更加详实的资料, 为精准手术提供指导。 Abstract:ObjectiveTo investigate the value of radiomic features of multi-parameter MRI(mp-MRI) for distinguishing T3a stage from T3b stage of prostate cancer. MethodsThe imaging data of 151 patients with T3 stage prostate cancer were retrospectively analyzed, including 110 patients with T3a stage and 41 patients with T3b stage.Using DARWIN research platform, regions of interest(ROI) were manually sketched on the transverse T2WI and ADC images to extract the radiomic features of image.The imaging data of ADC, T2WI and ADC combined with T2WI were divided into training group and verification group at the ratio of 3:1.Then the model of three groups of training group was built, and the corresponding tests were used for internal verification.The diagnostic efficacy of different sequences was analyzed by the ROC curve. ResultsA total of 1878 imaging features were extracted by DARWIN research platform, and 6 features(2 features of ADC and 4 features of T2WI) were retained(P < 0.05).The AUC values of training group and validation group under simple T2WI or ADC sequence were 0.79, 0.71, 0.59, 0.70.The AUC value of training group under ADC combined with T2WI sequence was 0.79, and that of validation group was 0.73. ConclusionsT2WI combined with ADC imaging radiomics has a good auxiliary value in the preoperative differential diagnosis of T3a and T3b prostate cancer, which can make up for the defect of MRI in the diagnosis of lesions less than 1 mm and provide the supplement for the invasion of seminal vesicle to obtain more clinical preoperative detailed information and provide the guidance for accurate surgery. -
Key words:
- prostate neoplasms /
- radiomics /
- multi-parameter MRI /
- T3a stage /
- T3b stage
-
表 1 训练集与验证集一般资料比较(x±s)
分组 n 年龄/岁 PSA/(ng/mL) 训练集 113 69.2±6.9 26.0(24.2) 验证集 38 68.6±7.5 22.5(12.4) t — 0.45 1.05 P — >0.05 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 3种模型在训练集和验证集中的统计学参数
模型 训练集 验证集 AUC(95%CI) 敏感性/% 特异性/% 准确性/% AUC(95%CI) 敏感性/% 特异性/% 准确性/% ADC 0.71(0.55~0.87) 61.3 80.5 78.8 0.70(0.40~0.96) 90.0 60.7 68.4 T2WI 0.79(0.66~0.92) 80.6 65.9 72.6 0.59(0.30~0.89) 90.0 53.6 73.7 ADC+T2WI 0.79(0.64~0.95) 61.3 96.3 81.4 0.73(0.47~1.00) 80.0 67.9 76.3
下载: 导出CSV
-
[1] SIEGEL RL, MILLER KD, JEMAL A. Cancer statistics, 2017[J]. CA Cancer J Clin, 2017, 65(1): 5. [2] JAGAI JS, MESSER LC, RAPPAZZO KM, et al. County-level cumulative environmental quality associated with cancer incidence[J]. Cancer, 2017, 123(15): 2901. doi: 10.1002/cncr.30709 [3] CHEN W, ZHENG R, BAADE PD, et al. Cancer statistics in China, 2015[J]. CA Cancer J Clin, 2016, 66(2): 115. doi: 10.3322/caac.21338 [4] BJURLIN MA, MENDHIRATTA N, TANEJA SS. Multiparametric MRI of the prostate as a tool for prostate cancer detection, localization, and risk assessment[J]. Cent Eur J Urol, 2016, 69(1): 9. doi: 10.1016/j.eururo.2015.07.004 [5] 汪维, 张青, 张冰, 等. 自由臂经会阴多参数磁共振-超声影像融合引导靶向穿刺诊断前列腺癌的前瞻性研究[J]. 中华泌尿外科杂志, 2018, 39(3): 192. doi: 10.3760/cma.j.issn.1000-6702.2018.03.009 [6] WEINREB JC, BARENTSZ JO, CHOYKE PL, et al. PI-RADS prostate imaging reporting and data system: 2015, Version 2[J]. Eur Urol, 2016, 69: 16. doi: 10.1016/j.eururo.2015.08.052 [7] 韩苏军, 张思维, 陈万青, 等. 中国前列腺癌发病现状和流行趋势分析[J]. 临床肿瘤学杂志, 2013, 18(4): 330. doi: 10.3969/j.issn.1009-0460.2013.04.009 [8] 熊升远, 阮同德. T3期前列腺癌治疗进展[J]. 国际泌尿系统杂志, 2015, 35(2): 279. doi: 10.3760/cma.j.issn.1673-4416.2015.02.038 [9] 罗超. T3期前列腺癌治疗的进展[J]. 世界最新医学信息文摘, 2019, 19(55): 36. [10] 李鑫, 王丽丽, 汪浩, 等. 去势抵抗性前列腺癌新型内分泌药物治疗次序的研究进展[J]. 肿瘤, 2017, 37(9): 995. [11] SCHULMAN C, CORNEL E, MATVEEV V, et al. Intermittent versus continuous androgen deprivation therapy in patients with relapsing or locally advanced prostate cancer: a phase 3b randomised study[J]. Eur Urol, 2016, 69(4): 720. doi: 10.1016/j.eururo.2015.10.007 [12] MAKAREWICZ R, ROSZKOWSKI K, LEBIODA A, et al. PSA bounces after brachytherapy HDR and external beam radiation therapy for prostate cancer[J]. Rep Pract Oncol Radioth, 2006, 11(5): 217. doi: 10.1016/S1507-1367(06)71066-5 [13] 陆黎, 孙宗琼, 李超凡, 等. 对比MRI与CT诊断不同病理分期前列腺癌的准确率[J]. 中国性科学, 2018, 27(12): 12. doi: 10.3969/j.issn.1672-1993.2018.12.003 [14] POLANEC SH, BICKEL H, WENGERT GJ, et al. Can the addition of clinical information improve the accuracy of PI-RADS version2 for the diagnosis of clinically significant prostate cancer in positive MRI?[J]. Clin Radiol, 2020, 75(2): 1. [15] XU M, FANG M, ZOU J, et al. Using biparametric MRI radiomics signature to differentiate between benign and malignant prostate lesions[J]. Eur J Radiol, 2019, 114(5): 38. [16] 张永生, 刘海明, 叶裕丰, 等. MR动态增强、DWI/ADC值等多参数成像与前列腺癌Gleason分级相关性研究[J]. 国际泌尿系统杂志, 2017, 37(6): 842. doi: 10.3760/cma.j.issn.1673-4416.2017.06.013 -

 点击查看大图
点击查看大图
图(4)表(2)
计量
- 文章访问数: 2916
- HTML全文浏览量: 1488
- PDF下载量: 9
- 被引次数: 0
