

-
肩锁关节脱位主要发生于车祸、跌落伤等高能量创伤,对于Rockwood分型Ⅰ、Ⅱ型等轻度脱位,通过物理治疗一定程度上能恢复肩关节正常功能,但超过Ⅲ型为完全脱位型,多伴随肩锁韧带、喙锁韧带断裂,多需要手术治疗[1]。既往多采用锁骨钩钢板进行内固定治疗,但易发生内固定断裂、肩峰撞击综合征等。目前对于肩锁关节脱位的治疗主张喙锁韧带重建以恢复喙锁韧带的解剖结构及生理功能[2]。近年弹性固定得到快速发展,以带襻双钛板(Tight Rope)为代表,加之内镜技术的进步,内镜辅助下进行肩锁关节弹性固定成为新的治疗趋势[3]。内镜下Tight Rope内固定术具有微创优势,瘢痕小、出血少,且能够早期进行功能锻炼,肩关节功能恢复更快;Tight Rope具备良好生物相容性,重建喙锁韧带后强度较高,能够获得早期稳定性,能促进韧带愈合。故本研究纳入40例病人,探究关节镜辅助Tight Rope内固定治疗肩锁关节脱位的疗效。现作报道。
-
病例纳入标准:(1)急外伤致肩锁关节脱位;(2)年龄>18岁,7 d内入院手术;(3)Rockwood分型为Ⅲ型、Ⅳ型或Ⅴ型;(4)未合并其他部位严重创伤。排除标准:(1)合并肩上肢严重软组织损伤;(2)肩关节或上肢手术史; (3)合并严重的神经或血管损伤; (4)骨折史或肩周炎等病史。本研究对象为2014年5月至2017年5月安徽中医药大学第三附属医院收治的40例肩锁关节脱位者,Rockwood分型:Ⅲ型27例,Ⅳ型13例。分析其病历资料,其中20例采用关节镜辅助Tight Rope内固定治疗,设为观察组; 20例病人切开肩锁关节复位联合锁骨钩钢板内固定治疗,设为对照组。2组一般资料比较差异均无统计学意义(P>0.05)(见表 1), 具有可比性。
分组 n 男 女 年龄(x±s)/岁 受伤原因 Rockwood分型 交通事故 跌落伤 Ⅲ Ⅳ 观察组 20 12 8 36.77±5.93 14 6 14 6 对照组 20 13 7 38.01±5.32 16 4 15 52 χ2 — 0.11 0.70* 0.53 0.13 P — >0.05 >0.05 >0.05 >0.05 *示t值 表 1 2组一般资料的比较(n)
-
所有病人手术均由同一组医生完成。观察组采用关节镜辅助Tight Rope内固定治疗,采用标准肩关节镜(30°)及配套设备。取沙滩椅位,全麻后固定头部,进行消毒、铺巾等常规术前手术准备,连接、调试关节镜及相关设备。根据影像检查结果再肩后外侧软点做小切口并置入关节镜头检查肩关节腔,采用穿刺针(9号)定位并开通内侧入路,刨削器刨除入口处滑膜,以增大术野。开通外侧入路并采用射频电刀逐渐显露内侧接近喙肩韧带,以喙肩韧带方向逐渐显露,直至镜下观察到喙突基底部,基底部宽度约1 cm。“C”臂透视明确肩锁关节间隙位置,向内侧10~15 mm处做2 cm的横形开口,显露锁骨远端,在定位器辅助下以锁骨中心至喙突基底部置入克氏针,镜下确认克氏针位置优良;空心钻头做骨道并置入引线钢丝,选择锁骨向喙突为起点,小心进行Tight Rope牵引,内镜辅助下小心传递、翻转Tight Rope纽扣,随后手法完成肩锁关节复位,适当拉紧缝线,头侧纽扣打结,尾线切断。透视确认复位满意、纽扣位置良好。缝合切口,常规抗感染24 h,悬吊固定带。根据病人实际情况逐步开展功能锻炼。对照组采用切开肩锁关节复位联合锁骨钩钢板内固定治疗,病人取沙滩椅仰卧手术体位,全麻后固定头部,术野消毒、铺单,患肩下垫高。自肩峰上沿锁骨向内侧做约8 cm的弧形切,组成分离,暴露肩峰、锁骨外段以及肩锁关节。将钩端与肩峰下缘紧贴并插至肩锁关节后方肩峰下。钢板安置在患侧锁骨外侧段上缘,并通过钢板适当下压锁骨以此复位肩锁关节,用规格适宜的螺钉将钢板牢固固定在锁骨上。透视明确复位良好,缝合切口,常规抗感染24 h,悬吊固定带。根据病人实际情况逐步开展功能锻炼。
-
(1) 记录手术时间、平均失血量、住院时间等手术相关指标及术后并发症情况。(2)术前、术后1个月、24个月评价功能症状指标,包括:①疼痛视觉模拟(VAS)评分,病人在VAS卡尺评分, “0”表示无痛,“10”表示难以忍受的最严重疼痛;②肩关节评分系统(UCLA),包括疼痛、活动、前屈力量等,共35分,分值越高表明肩关节功能越好;③Constant-Murley肩关节评分, 包括活动度、肌力等10项,共100分,分值越高肩关节功能越良好。(3)术后24个月参照UCLA评分评价综合疗效, 其中,优:34~35分,良:29~33分,可:24~28分,差: < 24分。
-
采用χ2检验、t检验和q检验。
-
观察组平均失血量、住院时间均低于对照组,差异有统计学意义(P < 0.01), 2组手术时间差异无统计学意义(P>0.05)(见表 2)。
分组 n 手术时间/min 平均失血量/mL 住院时间/d 观察组 20 75.39±6.76 57.88±9.91 6.81±0.67 对照组 20 73.11±6.03 163.23±13.91 7.98±1.02 t — 1.13 27.59 4.29 P — >0.05 < 0.01 < 0.01 表 2 2组围手术期指标的比较(x ±s)
-
2组术后1个月、24个月疼痛VAS评分均低于术前,UCLA评分、Constant-Murley评分均高于术前,差异均有统计学意义(P < 0.05~P < 0.01);术前2组VAS评分、UCLA评分和Constant-Murley评分差异均无统计学意义(P>0.05),观察组术后1个月UCLA评分、Constant-Murley评分,术后24个月UCLA评分均高于对照组,差异均有统计学意义(P < 0.01)(见表 3)。
分组 n VAS评分 UCLA评分 Constant-Murley评分 术前 观察组 20 6.39±0.88 22.87±4.01 43.52±4.55 对照组 20 6.42±0.90 22.87±4.12 43.98±4.31 t — 0.11 0.00 0.33 P — >0.05 >0.05 >0.05 术后1个月 观察组 20 2.32±0.20** 30.61±2.11** 70.54±9.14** 对照组 20 2.38±0.21** 28.01±2.01** 62.22±7.10** t — 0.93 3.99 3.21 P — >0.05 < 0.01 < 0.01 术后24个月 观察组 20 1.41±0.16**△△ 33.13±1.57**△ 86.18±4.57**△△ 对照组 20 1.48±0.17**△△ 31.32±1.50**△ 84.87±5.33**△△ t — 1.34 3.73 0.83 P — >0.05 < 0.01 >0.05 q检验:与术前比较*P < 0.05, **P < 0.01;与术后1个月比较△P < 0.05, △△P < 0.01 表 3 2组功能指标比较(x ±s; 分)
-
术后24个月观察组手术疗效优14例, 良5例, 中1例,优良率为95.00%,对照组优12例, 良6例, 中2例,优良率为90.00%,2组差异无统计学意义(χ2=0.00,P>0.05);观察组并发症发生率为0.00%, 对照组为15.00%(3/20), 其中2例肩峰撞击症,1例切口感染,2组并发症发生率差异无统计学意义(χ2=1.44,P>0.05)。
-
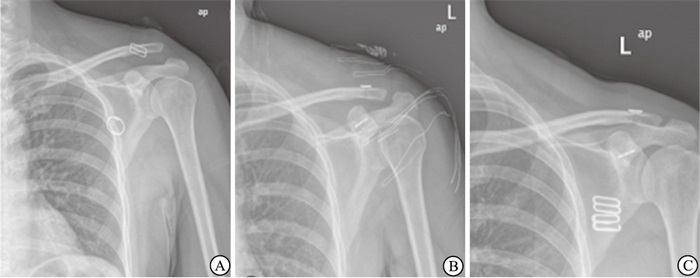
病人,女,40岁,高处摔下后左肩明显疼痛,肩关节功能障碍,受伤后当天入院;入院确诊肩锁关节Ⅲ型脱位,受伤后第2天行关节镜辅助Tight Rope内固定治疗(见图 1)。

图 1 典型病例X线片
-
肩锁关节脱位是骨科常见疾病,占肩关节损伤总病例数约12%,主要临床表现为肩部疼痛、活动受限。目前多数学者建议对RockWood Ⅲ型及以上肩锁关节脱位进行外科手术固定,以恢复肩锁关节正常的解剖结构及活动功能。常用术式包括克氏针固定、锁骨钩钢板固定、重建喙锁韧带、螺钉固定等,但各有优缺点。例如锁骨钩钢板固定钩部磨损肩峰下骨,肩峰与锁骨远端对钢板的撞击等,导致外展受限,甚至引起肩峰撞击综合征[6]。无论硬性固定、功能及解剖重建均易出现并发症。本研究结果亦显示,术后观察组无明显并发症, 对照组发生3例, 其中肩峰撞击症2例。Artherex公司近年研制的AC Tight Rope是专用于肩锁关节脱位的锁扣带襻双钛板,其内固定效果较好,且其弹性固定上述刚性固定相关并发症;亦能避免功能及解剖重建复杂的手术操作、腱-骨愈合差等缺点[7]。
本研究结构显示,观察组平均失血量、住院时间均显著低于对照组(P < 0.01),关节镜下手术较开放手术创伤更低,手术切口仅1~2 cm,具有微创优势。肩锁关节的功能在于提供肩峰、锁骨间滑动,保持锁骨、肩胛骨之间的相对旋转,其功能稳定性取决于韧带的正常结构。而Rockwood Ⅲ、Ⅳ型肩锁关节脱位喙锁韧带均完全撕裂,锁骨在上下、水平方向均失去稳定性,因此进行喙锁韧带的解剖重建对改善肩锁关节稳定性具有重要作用[8]。本研究结果显示,观察组术后1个月UCLA评分、Constant-Murley评分均高于对照组(P < 0.01),表明关节镜辅助Tight Rope治疗早期功能恢复效果更佳,总结其具有以下特点[9]:(1)Fiberwire线强度较高,其连接两块钢板,连续的环状无结结构被缝线牵拉收紧,肩锁关节准确复位,重建生物力学稳定性,且避免既往Endobutton钢板规格不适导致的复位不良; (2)非刚性固定能够确保肩锁关节能够保持微动,为早期功能锻炼提供基础,且无需再取出内固定,降低额外损伤;(3)Tight Rope的不可吸收Fberwire线具有具机体喙锁韧带相近的拉伸强度大致,能够完全满足对复位后肩锁关节的稳定性维持需要。
虽然关节镜辅助Tight Rope治疗肩锁关节脱位具有诸多优点, 但也需要注意以下事项,主要包括:(1)内镜下手术较开放性手术更复杂,术者需要具备丰富的手术经验,熟悉肩部组织的解剖结构,镜下操作时喙突基底部的暴露应适度,无需过度暴露,减少神经、血管损伤。(2)保证导针定位准确,避免反复钻孔,导针处于喙突正中位置时尽量一次穿过,避免反复钻孔、隧道偏移引发的骨折风险。(3)建立骨隧道时需准确判定锁骨的进针点,不可过偏,避免突破骨皮质;喙突骨隧道建立时要了解喙锁韧带走向,根据解剖位置进行骨隧道建立。(4)完整保留喙肩韧带,沿喙肩韧带进行喙突暴露时尽可能沿其表面操作,防止腱性组织损伤[10]。此外,其适应证包括[11]:(1)影像检查明确为单纯性肩锁关节脱位;(2)Rockwood分型Ⅲ~Ⅵ型;(3)新鲜损伤。禁忌证包括:(1)肩部软组织严重损伤不允许内镜手术;(2)陈旧性损伤;(3)合并严重骨质疏松症;(4)合并喙突骨折。
综上所述,关节镜辅助Tight Rope内固定治疗肩锁关节脱位能牢固固定脱位肩锁关节,降低疼痛症状、改善关节功能,还具有创伤小、并发症率低等优点。
内镜下带襻双钛板Tight Rope固定治疗肩锁关节脱位的临床疗效分析
Clinical effect analysis of double titanium plate with loop Tight Rope fixation under endoscopy in the treatment of acromioclavicular joint dislocation
-
摘要:
目的 探讨关节镜辅助带襻双钛板(Tight Rope)置入内固定治疗肩锁关节脱位的疗效。 方法 选择40例肩锁关节脱位病人作为研究对象,RockwoodⅢ型27例,Ⅳ型13例。其中20例采用关节镜辅助Tight Rope内固定治疗,设为观察组;20例采用切开复位锁骨钩钢板内固定治疗,设为对照组,均随访24个月以上。记录2组病人的手术相关指标及并发症情况,比较术前、术后1个月、24个月肩关节系统(UCLA)评分、疼痛视觉模拟(VAS)评分、Constant-Murley肩关节评分,术后24个月末参照UCLA评分评估综合疗效。 结果 观察组平均失血量、住院时间均低于对照组,差异有统计学意义(P < 0.01), 2组手术时间差异无统计学意义(P>0.05);2组术后1个月、24个月疼痛VAS评分均低于术前,UCLA评分、Constant-Murley评分均高于术前,差异均有统计学意义(P < 0.05~P < 0.01);术前2组VAS评分、UCLA评分和Constant-Murley评分差异无统计学意义(P>0.05),观察组术后1个月UCLA评分、Constant-Murley评分,术后24个月UCLA评分高于对照组,差异均有统计学意义(P < 0.01);术后24个月,2组手术疗效优良率、并发症发生率差异无统计学意义(P>0.05)。 结论 关节镜辅助Tight Rope内固定治疗肩锁关节脱位能牢固固定脱位肩锁关节,降低疼痛症状,改善关节功能,且具有创伤小、并发症率低等优点。 Abstract:Objective To study the effects of double titanium plate with loop(Tight Rope) fixation under endoscopy in the treatment of acromioclavicular joint dislocation. Methods Forty acromioclavicular joint dislocation patients included 27 cases of Rockwood type Ⅲ and 13 cases of type Ⅳ. Twenty cases treated with Tight Rope internal fixation under arthroscopy and 20 cases treated with open reduction and clavicular hook plate internal fixation were divided into the observation group and control group, respectively. Two groups were followed up for more than 24 months. The surgical indicators and complications in two groups were recorded. The comprehensive efficacy in two groups before operation, after 1 and 24 months of operation were evaluated using the shoulder joint system(UCLA), pain visual analogue(VAS) score and Constant-Murley shoulder score. Results The average blood loss and hospital stay in observation group were significantly lower than that in control group(P < 0.01), and the difference of the operation time between two groups was not statistically significant(P>0.05). The pain VAS scores in two groups after 1 and 24 months of surgery were lower than that before surgery, and the UCLA and Constant-Murley scores were higher than those before surgery(P < 0.05 to P < 0.01). The differences of the UCLA and Constant-Murley scores between two groups before operation were not statistically significant(P>0.05). The UCLA score and Constant-Murley score after 1 month of operation, and UCLA score after 24 months of operation in observation group were higher than those in control group(P < 0.01). The differences of the excellent and good rate of operation and in cidence rate of complications between two groups after 24 months of operation were not statistically significant(P>0.05). Conclusions The double titanium plate with loop fixation under endoscopy in the treatment of acromioclavicular joint dislocation can firmly fix the dislocated acromioclavicular joint, reduce pain symptoms and improve joint function, and also has the advantages of small trauma and low complication rate. -
表 1 2组一般资料的比较(n)
分组 n 男 女 年龄(x±s)/岁 受伤原因 Rockwood分型 交通事故 跌落伤 Ⅲ Ⅳ 观察组 20 12 8 36.77±5.93 14 6 14 6 对照组 20 13 7 38.01±5.32 16 4 15 52 χ2 — 0.11 0.70* 0.53 0.13 P — >0.05 >0.05 >0.05 >0.05 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 2组围手术期指标的比较(x ±s)
分组 n 手术时间/min 平均失血量/mL 住院时间/d 观察组 20 75.39±6.76 57.88±9.91 6.81±0.67 对照组 20 73.11±6.03 163.23±13.91 7.98±1.02 t — 1.13 27.59 4.29 P — >0.05 < 0.01 < 0.01
下载: 导出CSV
表 3 2组功能指标比较(x ±s; 分)
分组 n VAS评分 UCLA评分 Constant-Murley评分 术前 观察组 20 6.39±0.88 22.87±4.01 43.52±4.55 对照组 20 6.42±0.90 22.87±4.12 43.98±4.31 t — 0.11 0.00 0.33 P — >0.05 >0.05 >0.05 术后1个月 观察组 20 2.32±0.20** 30.61±2.11** 70.54±9.14** 对照组 20 2.38±0.21** 28.01±2.01** 62.22±7.10** t — 0.93 3.99 3.21 P — >0.05 < 0.01 < 0.01 术后24个月 观察组 20 1.41±0.16**△△ 33.13±1.57**△ 86.18±4.57**△△ 对照组 20 1.48±0.17**△△ 31.32±1.50**△ 84.87±5.33**△△ t — 1.34 3.73 0.83 P — >0.05 < 0.01 >0.05 q检验:与术前比较*P < 0.05, **P < 0.01;与术后1个月比较△P < 0.05, △△P < 0.01
下载: 导出CSV
-
[1] 黄强. 肩锁关节脱位的分型与治疗方法的选择[J]. 中国骨伤, 2015, 28(6): 487. doi: 10.3969/j.issn.1003-0034.2015.06.001 [2] ZHANG L, ZHOU X, QI J, et al. Modified closed-loop double-endobutton technique for repair of rockwood type Ⅲ acromioclavicular dislocation[J]. Exp Ther Med, 2018, 15(1): 940. [3] ARIRACHAKARAN A, BOONARD M, PIYAPITTAYANUN P, et al. Post-operative outcomes and complications of suspensory loop fixation device versus hook plate in acute unstable acromioclavicular joint dislocation: a systematic review and meta-analysis[J]. J Orthop Traumatol, 2017, 18(4): 293. doi: 10.1007/s10195-017-0451-1 [4] ARRIGONI P, BRADY PC, ZOTTARELLI L, et al. Associated lesions requiring additional surgical treatment in grade 3 acromioclavicular joint dislocations[J]. Arthroscopy, 2014, 30(1): 6. doi: 10.1016/j.arthro.2013.10.006 [5] 王进, 黄彰, 江华, 等. 纽扣钢板内固定治疗肩锁关节脱位31例[J]. 蚌埠医学院学报, 2014, 39(8): 1037. [6] BARTH J, DUPARC F, BAVEREL L, et al. Prognostic factors to succeed in surgical treatment of chronic acromioclavicular dislocations[J]. Orthop Traumatol Surg Res, 2015, 101(8S): S305. [7] Moura DL, Reis A RE, Ferreira J, et al. A combined technique for acromioclavicular reconstruction after acute dislocation - technical description and functional outcomes[J]. Tex State J Med, 2018, 53(1): 67. [8] BARAN S, BELISLE JG, GRANGER EK, et al. Functional and radiographic outcomes after allograft anatomic coracoclavicular ligament reconstruction[J]. J Orthop Trauma, 2018, 32(4): 204. doi: 10.1097/BOT.0000000000001079 [9] 张黎明, 汪志芳, 施海伟. 关节镜辅助锁扣带袢双钛板TightRope置入修复肩锁关节脱位: 早期即可坚强固定[J]. 中国组织工程研究, 2015, 19(9): 1441. [10] 陆友权, 方宣城, 李浩. 两种手术方式治疗肩锁关节脱位的疗效比较[J]. 蚌埠医学院学报, 2017, 42(7): 929. [11] GERHARDT C, KRAUS N, PAULY S, et al. Arthroscopically assisted stabilization of acute injury to the acromioclavicular joint with the double TightRope technique: one-year results[J]. Unfallchirurg, 2013, 116(2): 125. doi: 10.1007/s00113-011-2065-z -

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 2912
- HTML全文浏览量: 1320
- PDF下载量: 9
- 被引次数: 0
