

-
肠造口术是结直肠疾病治疗过程中一种常用的手术治疗方式。我国每年新增造口病人约10万例[1],造口术后早期并发症发生率16.3%~53.8%,其中造口周围刺激性皮炎是肠造口术后病人最常见的并发症,发生率可高达43%[2]。造口周围刺激性皮炎的发生将导致病人不同程度的疼痛,造口袋粘贴困难,降低病人造口护理自信心和生活质量[3]。造口周围刺激性皮炎多为造口用具与皮肤粘合不紧密,使粪便或肠液从造口胶盘处渗漏而刺激皮肤,因此裁剪形状和大小适宜的造口袋是防范渗漏关键。目前,临床上常使用描摹技术[4]裁剪造口袋。但描摹技术需使用油性笔和双层塑料薄膜,在病人造口上描画,再按照描画的图形使用剪刀裁剪造口袋,病人操作不方便,且存在较大误差。本研究设计可调节造口袋胶盘裁剪器(专利号:zl202021708055.5),可根据不同造口外形实现造口袋胶盘快速精确裁剪,应用于临床,取得良好效果。现作报道。
-
选取2020年3月至2021年3月入住我院普外科行肠造口手术的84例病人为研究对象。按随机对照法分为对照组和观察组,各42例。纳入标准: (1)年龄≥18岁,无残疾和肢体活动障碍,生活能够自理; (2)首次行肠造口术,具备独立学习并完成造口护理的病人;(3)意识清楚,能正常沟通,知情同意并配合本研究。排除标准: (1)对造口胶盘及附件产品过敏者; (2)造口周围存在严重皮肤疾病。
-
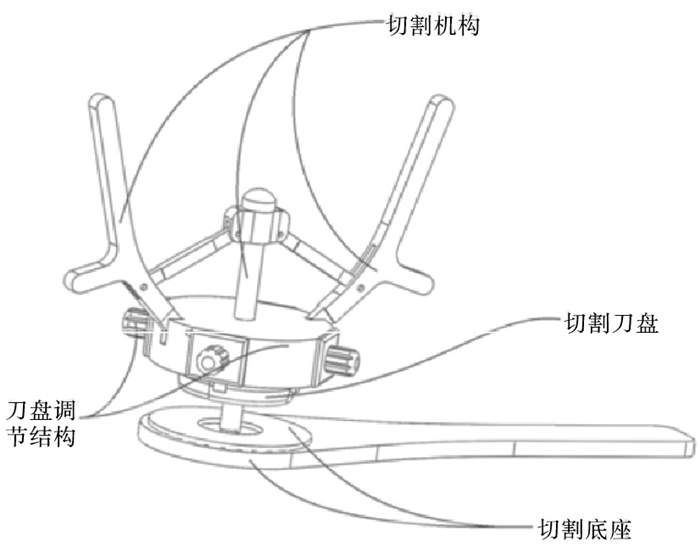
可调节造口袋胶盘裁剪装置分为三大部分:第一部分为一体式可调切割刀盘,第二部分为刀盘调节机构,第三部分为裁剪机构,包括切割机构和切割底座(见图 1)。切割刀盘为具有良好弹性单刃刀片,刀体靠近非刀刃一边有固定孔,固定孔与刀片固定槽内的固定铆钉契合防止刀片脱落,刀片通过变化重叠部分的多少实现刀盘大小调整,通过调节螺丝实现刀盘外形调整。外力通过切割手柄、牵拉中轴、切割底座等实现切割刀盘对造口袋胶盘的一体切割成型,可实现快速、高效、准确切割。

图 1 可调节造口袋胶盘裁剪器三维结构示意图
-
2组病人和家属均于术后第2天由造口治疗师按ARC[5]流程进行造口袋更换示范,在剪裁造口袋时,对照组使用造口尺测量造口直径,按照实际剪裁孔比测量孔大1~2 mm的原则,在造口胶盘标记线处,使用造口专用弯头剪刀裁剪胶盘。如造口形状不规则时,造口治疗师使用描摹法,在胶盘描画造口外形后使用剪刀裁剪造口袋。观察组使用造口尺测量造口上下径和左右径,依据测量数据确定各个调节螺丝位置,而后进行一次性冲压切割成型。如造口形状不规则,则增加测量不规则处最大直径和位置,并调节对应的螺丝位置,使裁剪刀片的形状接近造口形状,进行剪裁。2组病人使用不同的造口胶盘剪裁方法,分别于术后第5天在造口师的协作下按ARC流程自行更换造口袋。术后第8天2组病人使用不同的造口胶盘裁剪方法独立进行剪裁并按ARC流程更换造口袋,更换完毕,由造口治疗师对操作进行评价指导。
-
为了保证本研究质量,本研究由2名高级职称护理人员,1名造口治疗师,2个病区各1名责任组长,2名研究生组成。2名高级职称护理人员,1名造口治疗师全程参与本研究。造口治疗师负责病人造口袋更换指导;2名责任组长负责各病区评价指标收集;2名研究生负责数据汇总双人录入,保证准确性;2名高级职称护理人员负责本研究质量控制。
-
本研究评价指标采用克里夫兰医学中心佛罗里达造口功能指数(CCFOFI)量表[6],有关于生活质量的条目(更换造口袋难度、时间、是否需协助更换以及生活方式改变等)。(1)2组病人完成造口胶盘剪裁使用时间。指从病人测量造口至胶盘剪裁完成所用时间,精确到秒。(2)2组造口胶盘剪裁合适例数。以造口胶盘剪裁直径比造口直径大1~2 mm为标准。(3)2组造口胶盘剪裁不合适例数。以造口胶盘剪裁直径比造口直径大2~5 mm为标准。(4)2组造口胶盘报废例数。造口胶盘剪裁直径比造口直径大5 mm及以上,不规则造口,胶盘不规则处剪裁与造口形状不一致,无法佩戴,均属于报废。(5)2组病人剪裁造口胶盘难度评分。将胶盘剪裁分为易(独立完成,用时2 min以内)、一般(独立完成,用时3 min以上)、较难(需指导完成)、难(需协助完成),设定分值为1~4分。病人操作结束后评估并记录。(6)术后第8天2组病人造口胶盘渗漏情况。揭除造口胶盘后,检查造口胶盘背面的黏胶有腐蚀及排泄物残留,为造口胶盘渗漏[5]。
-
采用t检验、χ2检验和非参数Mann-Whitney秩和检验。
-
本次研究共纳入符合上述标准的病人84例,2组病人在年龄、性别、手术方式、造口类型、造口形状及生活自理能力评分方面比较差异均无统计学意义(P>0.05),具有可比性(见表 1)。
分组 n 男 女 年龄(x±s)/岁 疾病诊断 造口类型 造口形状 生活自理能力(x±s)评分/分 直肠癌 结肠癌 肠梗阻 回肠造口 结肠造口 襻式造口 圆形 不规则 观察组 42 31(73.8) 11(26.2) 65.90±12.83 29(69.1) 11(26.2) 2(4.8) 14(33.3) 27(64.3) 10(23.8) 28(66.7) 14(33.3) 97.14±4.57 对照组 42 28(66.7) 14(33.3) 67.97±10.28 37(88.1) 5(11.9) 0(0.0) 25(59.5) 17(40.5) 11(26.2) 30(71.4) 12(28.6) 98.09±3.97 χ2 — 0.51 0.82* 1.51 5.39 0.22 1.02* P — >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 *示t值 表 1 2组一般资料比较[n; 百分率(%)]
-
观察组病人独立完成造口胶盘剪裁使用(2.85±0.63)min,对照组病人独立完成造口胶盘剪裁使用(3.31±0.69)min,2组比较差异有统计学意义(t=3.20,P < 0.01)。
-
观察组病人造口胶盘剪裁优于对照组(P < 0.05),胶盘剪裁难度低于对照组(P < 0.05),术后第8天造口胶盘渗漏率低于对照组(P < 0.05)(见表 2)。
分组 n 造口胶盘 造口胶盘剪裁难度评分 造口胶盘渗漏 剪裁合适 剪裁不合适 报废 1分 2分 3~4分 是 否 观察组 42 34(81.0) 6(14.3) 2(4.8) 29(69.0) 10(23.8) 3(7.1) 8(19.1) 34(80.9) 对照组 42 27(64.3) 5(11.9) 10(23.8) 18(42.9) 16(38.1) 8(19.0) 17(40.5) 25(59.5) uc — 1.97 2.48 4.61* P — < 0.05 < 0.05 < 0.05 *示χ2值 表 2 2组病人造口胶盘剪裁和使用情况比较[n;百分率(%)]
-
结直肠癌是常见的消化系统恶性肿瘤之一,其发病率和死亡率均位居恶性肿瘤的第4位[7]。其中50%~60%的结直肠癌病人属于低位直肠癌,需接受永久性肠造口术[8]。随着加速康复外科在临床的广泛应用,肠造口病人的围手术期逐渐缩短,肠造口手术后住院时间大约为10 d[9]。在这有限的住院时间里,病人既要面对手术带来的生理和心理创伤,又要学习造口护理技术。有研究[10]显示多数永久性肠造口病人及家属住院期间未能完全掌握造口护理技能,以致病人出院后因护理不当而引起造口相关并发症,增加再入院率。造口病人多为老年人,因视力下降,思维、手指灵活性受限等诸多生理原因,对其术后的自护能力有所影响[11],尤其是造口袋的裁剪。临床中使用剪刀按照造口胶盘标志线剪裁,因病人视力下降,易出现剪裁过大或过小的现象。如造口为椭圆形,由于胶盘标志线均为圆形,无法完全按标志线剪裁,需病人依据经验手工调整剪裁的弧度,胶盘易出现边缘毛刺,不光滑,外形与造口边缘不贴合。本研究使用的可调节造口袋胶盘裁剪器,通过测量造口上下左右径,调节刀盘位置,直接切割成型。本研究显示观察组病人剪裁造口胶盘难度评分1分29例,2分10例,3分3例,对照组病人剪裁造口胶盘难度评分1分18例,2分16例,3分8例;观察组病人独立完成造口胶盘剪裁使用(2.85±0.63)min,对照组病人独立完成造口胶盘剪裁使用(3.31±0.69)min,2组比较差异有统计学意义(P < 0.05),说明可调节造口袋胶盘裁剪器操作简单,病人易于掌握,可以有效提升病人剪裁速度。如造口为非圆形的不规则造口,由于造口胶盘标志线在正面,病人剪裁胶盘不规则处的位置与实际粘贴造口袋时的方向相反,易出现误剪,使胶盘报废。而使用可调节造口袋胶盘裁剪器,通过测量不规则处最大直径,调节刀盘,由造口胶盘内面进行切割,与病人造口袋粘贴方向一致,不易出现误剪裁。本研究结果显示观察组造口胶盘剪裁合适34例,不合适6例,报废2例,对照组造口胶盘剪裁合适27例,不合适5例,报废10例,2组比较差异有统计学意义(P < 0.05),说明可调节造口袋胶盘裁剪器操作直观简单,剪裁准确,报废率低。
肠造口周围皮肤并发症作为最常见的造口问题,其中约77%的皮肤问题是底盘渗漏引起[12]。造口胶盘更换ARC流程,规范更换造口胶盘的手法及操作方式, 要求造口胶盘与造口黏膜之间保持适当空隙(1~2 mm)。空隙过大,粪水集聚,浸润胶盘,易引起胶盘渗漏,刺激皮肤易引起皮炎[5]。本研究显示术后第8天观察组造口胶盘渗漏8例,对照组造口胶盘渗漏17例,2组比较差异有统计学意义(P < 0.05),说明可调节造口袋胶盘裁剪器,可依据造口外形尺寸进行个体化调整,精确裁剪,降低了胶盘渗漏概率。
综上所述,可调节造口袋胶盘裁剪器可依据造口外形尺寸进行个体化调整,使剪裁的造口袋胶盘切缘圆滑,与造口外形完美契合、报废率低。而且操作直观简单,裁剪速度快,方便病人使用。
可调节造口袋胶盘裁剪器的设计和应用
Design and application of an adjustable plastic tray cutter for ostomy bag
-
摘要:
目的设计一种可调节造口袋胶盘裁剪器并探讨其应用效果。 方法选取2020年3月至2021年3月行造口手术病人84例,分为观察组和对照组,每组各42例。对照组使用造口专用剪刀剪裁造口袋胶盘,观察组使用可调节造口袋胶盘裁剪器剪裁造口袋胶盘。比较2组病人独立完成造口袋胶盘剪裁使用时间,造口袋胶盘剪裁难度评分、造口袋胶盘剪裁合适、不合适和报废例数以及术后第8天2组病人造口袋胶盘渗漏情况。 结果观察组病人独立完成造口袋胶盘剪裁使用时间少于对照组(P < 0.01)。观察组病人造口胶盘剪裁优于对照组(P < 0.05),胶盘剪裁难度低于对照组(P < 0.05),术后第8天造口胶盘渗漏率低于对照组(P < 0.05)。 结论造口袋胶盘调节裁剪器,可根据不同造口外形实现造口袋胶盘快速精确裁剪,报废率低,方便病人使用。 Abstract:ObjectiveTo design an adjustable plastic tray cutter for ostomy bag and discuss its application effect. MethodsA total of 84 patients with ostomy surgery from March 2020 to March 2021 were selected and divided into observation group and control group, 42 cases in each group. The control group used special scissors for stoma to cut the plastic disc of the ostomy bag, the observation group used an adjustable ostomy plastic tray cutter to cut the ostomy plastic tray. The time of patients independently completing the tailored ostomy plastic disc, difficulty score of tailoring plastic tray for ostomy bag, number of cases of proper, inappropriate and scrapped plastic tray for ostomy bag, and leakage of the plastic disc in the ostomy bag on the eighth day after surgery were compared. ResultsThe time of patients independently completing the cutting of pocket plastic disc in the observation group was less than that in the control group(P < 0.01). The cutting of colostomy plastic disc in the observation group was better than that in the control group(P < 0.05), the difficulty of plastic disc cutting was lower than that of the control group(P < 0.05), and the leakage rate of plastic disc was lower than that of the control group on the eighth day after operation(P < 0.05). ConclusionsThe adjustable plastic tray cutter for ostomy bag can realize rapid and accurate cutting of pocket plastic disc according to different stoma shapes, with low scrap rate and convenience for patients. -
Key words:
- enterostomy care /
- cutter /
- design
-
表 1 2组一般资料比较[n; 百分率(%)]
分组 n 男 女 年龄(x±s)/岁 疾病诊断 造口类型 造口形状 生活自理能力(x±s)评分/分 直肠癌 结肠癌 肠梗阻 回肠造口 结肠造口 襻式造口 圆形 不规则 观察组 42 31(73.8) 11(26.2) 65.90±12.83 29(69.1) 11(26.2) 2(4.8) 14(33.3) 27(64.3) 10(23.8) 28(66.7) 14(33.3) 97.14±4.57 对照组 42 28(66.7) 14(33.3) 67.97±10.28 37(88.1) 5(11.9) 0(0.0) 25(59.5) 17(40.5) 11(26.2) 30(71.4) 12(28.6) 98.09±3.97 χ2 — 0.51 0.82* 1.51 5.39 0.22 1.02* P — >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 2组病人造口胶盘剪裁和使用情况比较[n;百分率(%)]
分组 n 造口胶盘 造口胶盘剪裁难度评分 造口胶盘渗漏 剪裁合适 剪裁不合适 报废 1分 2分 3~4分 是 否 观察组 42 34(81.0) 6(14.3) 2(4.8) 29(69.0) 10(23.8) 3(7.1) 8(19.1) 34(80.9) 对照组 42 27(64.3) 5(11.9) 10(23.8) 18(42.9) 16(38.1) 8(19.0) 17(40.5) 25(59.5) uc — 1.97 2.48 4.61* P — < 0.05 < 0.05 < 0.05 *示χ2值
下载: 导出CSV
-
[1] 李道娟, 李倩, 何宇彤. 结直肠癌流行病学趋势[J]. 肿瘤防治研究, 2015, 42(3): 305. doi: 10.3971/j.issn.1000-8578.2015.03.020 [2] STEINHAE NE, RNCOLWEL LJ, CANNON LM. Intestinal stomas-postoperative stoma careand peristomal skin complications[J]. Clin Colon Rectal Surg, 2017, 30(3): 184. doi: 10.1055/s-0037-1598159 [3] 羡红涛, 张宇, 杨洋, 等. 结肠造口患者生活质量现状及影响因素研究[J]. 中国护理管理, 2018, 18(6): 829. doi: 10.3969/j.issn.1672-1756.2018.06.024 [4] 冼燕群, 乔建萍, 谭玉玲. 描摹技术在造口袋胶盘裁剪的应用[J]. 数理医药学杂志, 2018, 31(1): 149. [5] 王玉珏. ARC换药流程在结直肠癌术后造口周围皮肤的应用研究[J]. 护士进修杂志, 2017, 32(14): 1302. [6] COLQUHOUN P, KAISER R, WEISS EG, et al. Correlating the Fecal Incontinence Quality-of-Life Score and the SF-36 to a proposed Ostomy Function Index in patients with a stoma[J]. Ostomy Wound Manage, 2006, 52(12): 68. [7] 王锡山. 中美结直肠癌流行病学特征及防诊治策略的对比分析[J/CD]. 中华结直肠疾病电子杂志, 2017, 6(6): 447. [8] KIYO K, TOMOKO I, KAZUHIRO I. Comprehensive fluoro-genic derivatization-liquid chromatography/tandem mass spectrometry proteomic analysis of colorectal cancer cell to identify biomarker candidatel[J]. Biomed Chromatogr, 2013, 27(4): 440. doi: 10.1002/bmc.2811 [9] 陈凛, 陈亚进, 董海龙, 等. 加速康复外科中国专家共识及路径管理指南(2018版)[J]. 中国实用外科杂志, 2018, 38(1): 1. [10] 钟春霞, 魏清风, 熊燕, 等. 基于IMB模型的出院准备计划在结直肠癌永久性肠造口患者中的应用[J]. 护理学杂志, 2020, 35(21): 1. doi: 10.3870/j.issn.1001-4152.2020.21.001 [11] 罗洋, 代艺, 李芬. 特殊肠造口患者造口袋更换方法的改进[J]. 护理学杂志, 2019, 34(17): 39. [12] 张颜, 芦桂芝, 徐娜, 等. 肠造口周围皮肤常见问题护理现状[J]. 中国护理管理, 2014, 15(6): 602. -

 点击查看大图
点击查看大图
图(1)表(2)
计量
- 文章访问数: 2459
- HTML全文浏览量: 1178
- PDF下载量: 7
- 被引次数: 0
