



-
急性冠状动脉综合征(ACS)是一组严重的心脏急性缺血综合征[1-2],其病情变化迅速,且对心肌产生不可逆转的缺血损伤。虽然随着现代医学水平的进步,ACS的发病机制已逐渐明确[3-4],治疗方案也日趋完善,但仍有部分病人在接受了系统的药物及介入治疗后会出现不良心血管事件[1-2, 5-6]。因此,积极探索心肌细胞死亡调控通路,保护心脏免受缺血相关损伤,将对临床靶向防治ACS并改善其远期预后有重要的指导价值。
有研究[7]表明,抑制谷胱甘肽过氧化物酶4(GPX4)的功能将导致细胞膜发生脂质过氧化,并可诱导铁死亡。FENG等[8]研究发现,铁死亡抑制剂利普罗斯他汀-1通过增加GPX4活性,减少线粒体脂质活性氧的生成,保护小鼠心肌细胞免受缺血再灌注损伤。我们推测ACS病人可能会因为高水平的GPX4抑制心肌细胞铁死亡而获益。但目前GPX4与ACS之间的相关性仍不明确,血浆GPX4水平与心肌缺血损伤之间的研究大多处于基础研究阶段。本研究采用酶联免疫吸附法(ELISA)对404例病人的血浆GPX4水平进行检测,观测血浆GPX4水平变化与ACS病人临床特征、危险分层及其预后之间的相关性,从而为更精确有效地防治ACS并改善其预后提供新的治疗思路。
-
纳入2018年11月至2019年6月因胸痛于我科住院治疗并拟行冠状动脉造影检查的病人404例。ACS组纳入标准:依据中华医学会相关指南[9-12],根据病史、生化指标、影像学检查及冠脉造影结果分为不稳定型心绞痛组(UAP组)261例和急性心肌梗死组(AMI组)55例。同时选取同期行冠状动脉造影并排除冠心病诊断的病人为对照组。排除标准:肝肾功能不全,急性脑血管疾病,感染性疾病,肿瘤等消耗性疾病,血液系统疾病,碘及造影剂过敏和病史资料收集不全的病人。
-
所有病人均于入院后次日清晨在空腹状态下接受肘静脉血的采集,分别抽取5 mL置于肝素钠抗凝试管中,送往我院检验科进行各项常规生化指标检测;5 mL置于EDTA抗凝试管中,送往我院心肺实验室,经过离心留存血清,置于-80 ℃环境下保存,待样本集齐后,采用ELASA检测每个样本中血浆GPX4的水平[13]。
-
采用Judkins[14-15]法行冠状动脉造影,判断造影结果的标准为美国ACC/AHA心血管疾病诊治报告[16],由经验丰富的专业心内科医师操作完成。应用Gensini评分[17]评估病人冠状动脉病变严重程度。
-
采用心肌梗死溶栓治疗临床试验危险评分(TIMI危险评分)[18-19]对ACS组病人进行危险分层,UAP/NSTEMI和STEMI病人按不同评分标准计算。
-
采用门诊及电话随访等形式,追踪随访ACS组病人院外主要心血管不良事件(MACEs)[20]的发生情况,平均为期21个月。本研究包含的MACEs为:再发胸痛、心力衰竭、脑卒中、再发心梗、出血、再次血运重建、支架内血栓、支架内再狭窄、死亡。
-
采用t检验、χ2检验、非参数秩和检验、Kaplan-Meier法、ROC分析和Cox风险比例回归分析。
-
ACS组在年龄、男性病人比例、合并高血压、合并糖尿病、血肌酐、TG、低密度脂蛋白水平上高于对照组,而高密度脂蛋白水平低于对照组(P < 0.05~P < 0.01)(见表 1)。
分组 n 年龄/岁 男 高血压 糖尿病 血糖/(mmol/L) 尿酸/(μmol/L) 肌酐/(μmol/L) ACS组 316 63.33±10.89 201 202 76 5.85(5.51, 6.20) 315.31(304.25, 326.37) 70.55(68.31, 72.79) 对照组 88 57.77±10.34 44 43 6 5.42(5.07, 5.77) 302.96(286.11, 319.81) 63.42(60.94, 65.90) Zc — 4.27* 5.02# 6.54# 12.48# 0.77 1.56 4.05 P — < 0.01 < 0.05 < 0.05 < 0.01 >0.05 >0.05 < 0.01 分组 n 总胆固醇/(mmol/L) 三酰甘油/(mmol/L) 低密度脂蛋白胆固醇/(mmol/L) 高密度脂蛋白胆固醇/(mmol/L) C反应蛋白/(mg/L) D-二聚体/(mg/L) 脂蛋白a/(mg/L) ACS组 316 4.02(3.86, 4.17) 1.74(1.60, 1.88) 2.26(2.16, 2.35) 0.96(0.92, 1.00) 5.46(3.55, 7.37) 0.57(0.39, 0.74) 363.68(327.29, 400.08) 对照组 88 3.96(3.73, 4.18) 1.47(1.25, 1.69) 2.04(2.01, 2.16) 1.01(0.94, 1.07) 4.54(1.92, 7.16) 0.76(0.12, 1.41) 287.57(237.61, 337.53) Zc — 1.98 2.31 3.05 1.88 1.60 0.37 0.37 P — >0.05 < 0.05 < 0.05 < 0.05 >0.05 >0.05 >0.05 *示t值;#示χ2值 表 1 AC组与对照组病人基线资料比较[M(P25, P75)]
-
ACS组血浆GPX4水平低于对照组(P < 0.05)。UAP组与AMI组血浆GPX4水平差异无统计学意义(P>0.05)(见表 2)。
分组 n GPX4/(ng/mL) ACS组 316 103.80(101.50,106.11) 对照组 88 131.38(126.31,136.45) Zc — 9.48 P — < 0.05 UAP组 261 105.09(102.67,107.51) AMI组 55 104.23(98.47,109.99) Zc — 0.49 P — >0.05 表 2 不同病人血浆GPX4水平比较
-
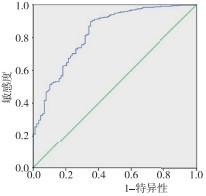
ROC曲线显示血浆CTPX4水平可以辅助ACS的诊断。ROC曲线下面积(AUC)为0.828(0.778~0.878),其最佳截断点为128.78 ng/mL,特异性为64.8%,敏感性为90.0%(P < 0.05)(见图 1)。
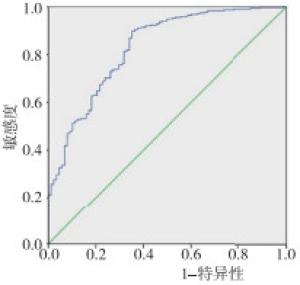
图 1 血浆GPX4水平对ACS诊断的ROC曲线
-
根据病人TIMI危险评分将ACS组病人分为低危组、中危组和高危组,结果发现,低危组在年龄、合并高血压、C反应蛋白、D-二聚体水平均低于中危组及高危组,在合并糖尿病、Gensini评分水平低于高危组,在男性病人占比上高于高危组(P < 0.05~P < 0.01)。低危组血浆GPX4水平高于中危组和高危组(P < 0.05),高危组病人血浆GPX4水平与中危组差异无统计学意义(P>0.05)(见表 3)。
分组 n 年龄/岁 男 高血压 糖尿病 血糖/(mmol/L) 尿酸/(μmol/L) 肌酐/(μmol/L) 总胆固醇/(mmol/L) 三酰甘油/(mmol/L) 低危组 53 54.58±7.85 41 24 8 5.18(4.57, 5.79) 342.78(314.89, 370.66) 66.95(63.58, 70.32) 4.04(3.66, 4.42) 1.72(1.33, 2.12) 中危组 227 64.46±10.61* 142 146* 46 5.81(5.43, 6.19) 309.49(296.17, 322.80) 71.10(68.29, 73.91) 4.00(3.80, 4.19) 1.74(1.57, 1.92) 高危组 36 69.03±9.56* 18* 32* 22* 6.77(5.11, 8.42) 302.44(268.93, 335.95) 72.56(63.50, 81.62) 4.20(3.70, 4.71) 1.79(1.50, 2.09) Zc — 27.00 7.41 17.61# 31.50# 5.97 4.60 0.53 1.58 4.11 P — < 0.01 < 0.05 < 0.01 < 0.01 >0.05 >0.05 >0.05 >0.05 >0.05 分组 n 低密度脂蛋白胆固醇/(mmol/L) 高密度脂蛋白胆固醇/(mmol/L) C反应蛋白/(mg/L) D-二聚体/(mg/L) 脂蛋白a/(mg/L) Gensini评分 GPX4 /(ng/mL) 低危组 53 2.30(2.03, 2.57) 0.96(0.90, 1.03) 1.59(1.01, 2.18) 0.26(0.16, 0.37) 363.68(327.29, 400.08) 23.75(16.70, 30.80) 114.63(107.46, 121.79) 中危组 227 2.14(2.02, 2.27) 0.95(0.92, 0.98) 5.91(3.42, 8.41)* 0.57(0.34, 0.79)* 332.72(291.79, 373.65) 33.18(28.54, 37.81) 101.61(99.01, 104.20)* 高危组 36 2.41(2.07, 2.74) 1.06(0.69, 1.43) 8.38(1.23, 15.54)* 0.79(0.35, 1.24)* 378.36(248.47, 508.25) 52.44(37.23, 67.65)* 102.75(96.85, 108.66)* Zc — 3.68 3.53 9.99 16.49 3.67 13.78 14.50 P — >0.05 >0.05 < 0.01 < 0.01 >0.05 < 0.01 < 0.05 与低危组比较*P < 0.05;#示χ2值 表 3 TIMI危险分层低危组、中危组和高危组病人基线资料比较[M(P25, P75)]
-
ROC曲线显示血浆GPX4水平可以辅助TIMI危险分层中低危病人的诊断。AUC为0.665(0.577~0.754),敏感度为37.7%,特异性为95.0%,最佳截断值为127.06 ng/mL(P < 0.05)(见图 2)。
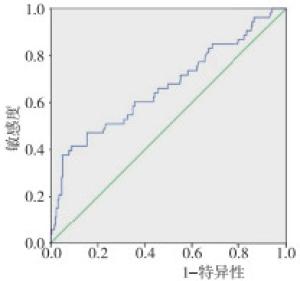
图 2 血浆GPX4水平对TIMI危险分层低危病人的ROC曲线
-
本研究对ACS组病人进行了平均21个月的门诊或电话随访,其中4例(1.3%)失访,共30例(9.5%)发生MACEs事件。根据随访结果中病人是否发生MACEs事件,将ACS组病人分为MACEs组30例和非MACEs组282例,结果发现,MACEs组病人GPX4水平为95.16(90.05,100.26)ng/mL, 低于非MACEs组104.53(102.01,107.06)ng/mL(Zc=2.86, P < 0.05)。
-
依据所有ACS病人测得GPX4数值的中位数将研究对象分为GPX4≥101.90 ng/mL组和GPX4 < 101.90 ng/mL组,绘制Kaplan-Meier曲线。在所有ACS病人中,4例失访。GPX4≥101.90 ng/mL 158例,失访2例,共10例发生MACEs事件,平均生存时间为620.06 d;GPX4 < 101.90 ng/mL的病人人数为158例,失访2例,共20例发生MACEs事件,平均生存时间为607.23 d。K-M曲线显示,血浆GPX4 < 101.90 ng/mL的ACS病人预期生存时间与GPX4≥101.90 ng/mL组差异无统计学意义(χ2=3.70,P>0.05)(见图 3)。

图 3 K-M曲线分析对GPX4对ACS病人发生MACEs的预测价值
-
将血浆GPX4水平纳入Cox风险比例回归分析,结果显示,B′为-0.03,SE为0.01,Waldχ2为6.99,OR(95%CI)为0.97(0.95~0.99)。随着ACS病人血浆GPX4水平的升高,ACS病人发生MACEs事件的风险降低,表明血浆GPX4水平升高是MACEs事件发生的保护因素(P < 0.05)。
-
ACS在我国发病率持续升高,给社会带来严重的医疗负担[21]。并且由于心肌细胞是终末分化细胞,当心脏受到缺血损伤时,心肌细胞受到的打击将不可逆转,导致心肌细胞数量上永久减少,从而引起ACS严重的临床症状及不良的预后。因此,探索心肌细胞死亡的调控通路,抑制心肌细胞死亡,保护心脏免受缺血相关损伤,将对临床靶向防治ACS并改善其远期预后起到重要的指导价值。
铁死亡是来自哥伦比亚大学的研究人员DIXON等[22]于2012年正式提出的一种由小分子Erastin诱导的铁依赖性的新型细胞死亡形式。这一过程的特点是大量的、依赖于铁元素的脂质活性氧(ROS)的积累[23-24]。形态学上,铁死亡的主要变化在于线粒体的损伤,表现为线粒体外膜的破裂、线粒体膜的固缩以及线粒体嵴的减少或消失[25]。当细胞内铁代谢的稳定被打破时,细胞产生过量的铁离子(Fe2+),Fe2+在微酸环境下发生芬顿反应(Fenton)生成大量ROS,随着ROS在细胞内的不断堆积,逐步诱发细胞的铁死亡[26-27],这是目前已知的铁死亡基础启动机制。
GPX4是一种特殊的硒蛋白[28],它可以将脂质ROS还原为无毒的脂质醇,限制了脂质过氧化物在膜质中的传播,有效预防了细胞的氧化应激,从而抑制细胞的铁死亡进程[29]。因为其在铁死亡发生发展中的关键作用机制,GPX4这一铁死亡调控因子已成为研究热门。来自武汉大学的李文远等[30]的研究证明,靶向抑制铁死亡在保护心肌细胞对抗过量铁及缺血再灌注损伤时发挥了重要的作用。因此,铁死亡中的关键因子GPX4可能与心肌缺血性疾病ACS之间具有相关性。本研究发现,ACS病人的血浆GPX4水平比正常对照组病人明显降低(P < 0.05),并且GPX4的ROC AUC为0.83(0.78~0.88),其最佳截断点为128.78 ng/mL,特异性为64.8%,敏感性为90.0%,提示GPX4对于ACS的诊断具有一定的参考价值。但在比较UAP组与AMI组病人血浆GPX4水平时,两者的差异无统计学意义,可能说明GPX4对反映ACS的诊断比较敏感,但对ACS中各种亚型的鉴别价值不大。TIMI危险评分是临床上针对于ACS病人预后的危险评分[31],用于ACS病人的危险分层与预后预测时,操作方便,实用,有效。本研究发现,TIMI危险分层低危组病人的血浆GPX4水平高于中危组和高危组(P < 0.05),并且ROC曲线显示,血浆GPX4对TIMI危险分层中病人是否处于低危状态具有判别价值,其中AUC为0.665(0.578,0.754),敏感度为37.7%,特异性为95.0%,最佳截断值为127.06 ng/mL(P < 0.05),这表明GPX4对于临床对ACS病人进行TIMIT危险分层具有辅助参考价值。然而,高危组和中危组病人血浆GPX4水平差异无统计学意义,可能与本研究纳入高危组病人数量较少有关,有待进一步研究探讨与完善。
本研究对总计316例ACS病人进行了平均21个月的电话或门诊随访,其中4例(1.3%)失访,30例(9.6%)发生MACEs事件。我们发现MACEs组病人的血浆GPX4水平低于非MACEs组病人(P < 0.05);Cox回归分析显示,GPX4是避免ACS病人发生MACEs事件的保护因素,提示高水平的血浆GPX4水平降低了ACS病人发生MACEs事件的风险。通过检测ACS病人的GPX4水平,可以有效地帮助临床医生判断病人的远期预后,对改善病人院外生存率可能起到积极作用[32]。Kaplan-Meier曲线分析显示血浆GPX4 < 101.90 ng/mL的病人发生MACEs事件的平均时间有比GPX4≥101.90 ng/mL的病人更早的趋势,但Logrank检验P>0.05,差异无统计学意义,可能与本研究纳入病人人数较少、随访时间较短导致发生终点事件的人数过少有关,有待进一步研究。
综上所述,血浆GPX4水平对于ACS的诊断、TIMI危险分层、远期预后的判断均有参考价值。为在阐明GPX4在冠心病中的作用机制,并通过靶向干预铁死亡在临床上进行ACS的防治,提供新的思路与参考依据。本研究为单中心回顾性研究,纳入的样本量较少,排除了严重的肝肾功能及心肺功能不全的病人,且随访时间较短,MACEs的发生率偏低,只是初步的经验总结,有待后续研究深入探讨。
GPX4水平与急性冠状动脉综合征病人临床特征、危险分层及其预后相关性研究
Study on the correlation between the plasma level of glutathione peroxidase 4 and clinical characteristics, risk stratification and prognosis of patients with acute coronary syndrome
-
摘要:
目的探讨血浆谷胱甘肽过氧化物酶4(GPX4)水平与急性冠状动脉综合征(ACS)病人临床特征、危险分层及预后之间的相关性。 方法拟行冠状动脉造影病人404例,依据病史、生化检验指标、影像学检查结果及冠状动脉造影检查结果分为ACS组(n=316)和对照组(CON组,n=88)。并将ACS组病人分为不稳定型心绞痛组(UAP组,n=261)和急性心肌梗死组(AMI组,n=55)。依据TIMI危险分层将ACS组病人分为高危组(n=36)、中危组(n=227)和低危组(n=53)。采用酶联免疫吸附法检测病人血浆GPX4水平。出院后对ACS组病人进行平均21个月的随访,追踪有无主要心血管不良事件(MACEs)的发生,其中4例失访,将病人分为MACEs组(n=30)和非MACEs组(n=282), 依据ACS组病人GPX4水平中位数将病人分为GPX4≥101.90 ng/mL组(n=158)和GPX4 < 101.90 ng/mL组(n=158)。 结果ACS组病人血浆GPX4水平低于对照组(P < 0.05)。ROC曲线显示血浆GPX4水平可以辅助ACS的诊断,曲线下面积(AUC)为0.828(0.778~0.878),其最佳截断点为128.78 ng/mL,特异性为64.8%,敏感性为90.0%。在TIMI危险分层中,与高危组和中危组相比,低危组血浆GPX4水平升高(P < 0.05),ROC曲线显示血浆GPX4水平可以辅助判断ACS病人是否处于TIMI危险分层中的低危状态AUC为0.665(0.577~0.754),最佳截断值为127.06 ng/mL,敏感度为37.7%,特异性为95.0%(P < 0.05)。MACEs组病人血清GPX4水平低于非MACEs组(P < 0.05)。Kaplan-Meier曲线中GPX4 < 101.90 ng/mL组和GPX4≥101.90 ng/mL组中生存时间的差异无统计学意义(P < 0.05)。血浆GPX4水平升高是MACEs发生的保护因素(P < 0.05)。 结论血浆GPX4水平对ACS病人临床诊断、TIMI危险分层及远期预后的判断均有参考价值。 -
关键词:
- 急性冠状动脉综合征 /
- 谷胱甘肽过氧化物酶4 /
- TIMI危险分层 /
- 临床预后
Abstract:ObjectiveTo explore the correlation between the plasma level of glutathione peroxidase 4(GPX4) and clinical characteristics, risk stratification and prognosis of patients with acute coronary syndrome(ACS). MethodsA total of 404 patients scheduled by coronary angiography were divided into the ACS group(n=316) and control group(n=88) according to the medical history, biochemical examination, results of imaging examination and coronary angiography.The ACS group was subdivided into the unstable angina pectoris group(UAP group, n=261) and acute myocardial infarction group(AMI group, n=55).According to TIMI risk stratification, the ACS patients were divided into the high-risk group(n=36), medium-risk group(n=227) and low-risk group(n=53).The plasma levels of GPX4 in all cases were determined by enzyme linked immunosorbent assay.The ACS group was followed up for an average of 21 months after discharge for major adverse cardiovascular events(MACEs), 4 cases were lost to follow-up, and the other patients were divided into the MACEs group(n=30) and non-MACEs group(n=282).The ACS group were divided into the GPX4≥101.90 ng/mL group(n=158) and GPX4 < 101.90 ng/mL group(n=158) according to the median GPX4 level of pateints. ResultsThe serum levels of GPX4 in ACS group were lower than that in control group(P < 0.05).The results of ROC curve showed that serum level of GPX4 could assist the diagnosis of ACS.The area under curve(AUC) was 0.828(0.778-0.878), the optimal cut-off value was 128.78 ng/mL, the specificity was 64.8%, and the sensitivity was 90.0%.In TIMI risk stratification, the serum level of GPX4 in low-risk group was higher than that in high-risk and medium-risk groups(P < 0.05).The results of ROC curve showed that the serum level of GPX4 could assist in determining whether ACS patients were in low-risk state in TIMI risk stratification, and the AUC was 0.665(0.577-0.754).The optimal cut-off value was 127.06 ng/mL, the sensitivity was 37.7%, and the specificity was 95.0%(P < 0.05).The level of GPX4 in MACEs group was lower than that in non-MACEs group(P < 0.05).There was no statistical significance in the survival time between GPX4 < 101.90 ng/mL group and GPX4≥101.90 ng/mL group in Kaplan-Meier curve.The serum level of GPX4 increasing was a protective factor for MACEs(P < 0.05). ConclusionsThe serum level of GPX4 has reference value in the clinical diagnosis, TIMI risk stratification and long-term prognosis of ACS patients. -
表 1 AC组与对照组病人基线资料比较[M(P25, P75)]
分组 n 年龄/岁 男 高血压 糖尿病 血糖/(mmol/L) 尿酸/(μmol/L) 肌酐/(μmol/L) ACS组 316 63.33±10.89 201 202 76 5.85(5.51, 6.20) 315.31(304.25, 326.37) 70.55(68.31, 72.79) 对照组 88 57.77±10.34 44 43 6 5.42(5.07, 5.77) 302.96(286.11, 319.81) 63.42(60.94, 65.90) Zc — 4.27* 5.02# 6.54# 12.48# 0.77 1.56 4.05 P — < 0.01 < 0.05 < 0.05 < 0.01 >0.05 >0.05 < 0.01 分组 n 总胆固醇/(mmol/L) 三酰甘油/(mmol/L) 低密度脂蛋白胆固醇/(mmol/L) 高密度脂蛋白胆固醇/(mmol/L) C反应蛋白/(mg/L) D-二聚体/(mg/L) 脂蛋白a/(mg/L) ACS组 316 4.02(3.86, 4.17) 1.74(1.60, 1.88) 2.26(2.16, 2.35) 0.96(0.92, 1.00) 5.46(3.55, 7.37) 0.57(0.39, 0.74) 363.68(327.29, 400.08) 对照组 88 3.96(3.73, 4.18) 1.47(1.25, 1.69) 2.04(2.01, 2.16) 1.01(0.94, 1.07) 4.54(1.92, 7.16) 0.76(0.12, 1.41) 287.57(237.61, 337.53) Zc — 1.98 2.31 3.05 1.88 1.60 0.37 0.37 P — >0.05 < 0.05 < 0.05 < 0.05 >0.05 >0.05 >0.05 *示t值;#示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 不同病人血浆GPX4水平比较
分组 n GPX4/(ng/mL) ACS组 316 103.80(101.50,106.11) 对照组 88 131.38(126.31,136.45) Zc — 9.48 P — < 0.05 UAP组 261 105.09(102.67,107.51) AMI组 55 104.23(98.47,109.99) Zc — 0.49 P — >0.05
下载: 导出CSV
表 3 TIMI危险分层低危组、中危组和高危组病人基线资料比较[M(P25, P75)]
分组 n 年龄/岁 男 高血压 糖尿病 血糖/(mmol/L) 尿酸/(μmol/L) 肌酐/(μmol/L) 总胆固醇/(mmol/L) 三酰甘油/(mmol/L) 低危组 53 54.58±7.85 41 24 8 5.18(4.57, 5.79) 342.78(314.89, 370.66) 66.95(63.58, 70.32) 4.04(3.66, 4.42) 1.72(1.33, 2.12) 中危组 227 64.46±10.61* 142 146* 46 5.81(5.43, 6.19) 309.49(296.17, 322.80) 71.10(68.29, 73.91) 4.00(3.80, 4.19) 1.74(1.57, 1.92) 高危组 36 69.03±9.56* 18* 32* 22* 6.77(5.11, 8.42) 302.44(268.93, 335.95) 72.56(63.50, 81.62) 4.20(3.70, 4.71) 1.79(1.50, 2.09) Zc — 27.00 7.41 17.61# 31.50# 5.97 4.60 0.53 1.58 4.11 P — < 0.01 < 0.05 < 0.01 < 0.01 >0.05 >0.05 >0.05 >0.05 >0.05 分组 n 低密度脂蛋白胆固醇/(mmol/L) 高密度脂蛋白胆固醇/(mmol/L) C反应蛋白/(mg/L) D-二聚体/(mg/L) 脂蛋白a/(mg/L) Gensini评分 GPX4 /(ng/mL) 低危组 53 2.30(2.03, 2.57) 0.96(0.90, 1.03) 1.59(1.01, 2.18) 0.26(0.16, 0.37) 363.68(327.29, 400.08) 23.75(16.70, 30.80) 114.63(107.46, 121.79) 中危组 227 2.14(2.02, 2.27) 0.95(0.92, 0.98) 5.91(3.42, 8.41)* 0.57(0.34, 0.79)* 332.72(291.79, 373.65) 33.18(28.54, 37.81) 101.61(99.01, 104.20)* 高危组 36 2.41(2.07, 2.74) 1.06(0.69, 1.43) 8.38(1.23, 15.54)* 0.79(0.35, 1.24)* 378.36(248.47, 508.25) 52.44(37.23, 67.65)* 102.75(96.85, 108.66)* Zc — 3.68 3.53 9.99 16.49 3.67 13.78 14.50 P — >0.05 >0.05 < 0.01 < 0.01 >0.05 < 0.01 < 0.05 与低危组比较*P < 0.05;#示χ2值
下载: 导出CSV
-
[1] OYLUMLU M, OYLUMLU M, ARIK B, et al. Monocyte to high-density lipoprotein cholesterol and lymphocyte to monocyte ratios are predictors of in-hospital and long-term mortality in patients with acute coronary syndrome[J]. Int J Clin Pract, 2021, 75(5): e13973. [2] 张宁, 刘文娴, 康云鹏. 超效C-反应蛋白与白蛋白比值对急性冠综合征患者死亡的预测价值[J]. 中华危重病急救医学, 2021, 33(5): 573. doi: 10.3760/cma.j.cn121430-20201127-00736 [3] SOEHNLEIN O, BAZIOTI V, WESTERTERP M. A pad 4 plaque erosion[J]. Circ Res, 2018, 123(1): 6. doi: 10.1161/CIRCRESAHA.118.313110 [4] BENTZON JF, OTSUKA F, VIRMANI R, et al. Mechanisms of plaque formation and rupture[J]. Circ Res, 2014, 114(12): 1852. doi: 10.1161/CIRCRESAHA.114.302721 [5] ZHANG S, WANG W, SAWHNEY JPS, et al. Antithrombotic management and long-term outcomes following percutaneous coronary intervention for acute coronary syndrome in Asia[J]. Int J Cardiol, 2020, 310(1): 16. [6] KONG S, CHEN C, ZHENG G, et al. A prognostic nomogram for long-term major adverse cardiovascular events in patients with acute coronary syndrome after percutaneous coronary intervention[J]. BMC Cardiovasc Disord, 2021, 21(1): 253. doi: 10.1186/s12872-021-02051-0 [7] NI J, CHEN K, ZHANG J, et al. Inhibition of GPX4 or mTOR overcomes resistance to Lapatinib via promoting ferroptosis in NSCLC cells[J]. Biochem Biophys Res Commun, 2021, 567(19): 154. [8] FENG YC, ALIAGAN ACI, TOMBO NC, et al. Inhioition of ferroptosis by liproxstatin-1 compound protects the myocardium against ischemia/reperfusion injury by decreasing VDAC1 levels and increasing in GPX4 activity[J]. Faseb J, 2019, 520(3): 606. [9] 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 非ST段抬高型急性冠状动脉综合征诊断和治疗指南(2016)[J]. 中华心血管病杂志, 2017, 45(5): 359. doi: 10.3760/cma.j.issn.0253-3758.2017.05.003 [10] 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019, 10(47): 766. [11] LIU C, JIANG SQ, LI J, et al. Prognostic potential of layer-specific global longitudinal strain in patients with non-ST-segment elevated acute coronary syndrome and preserved left ventricular ejection fraction[J]. Int J Cardiovasc Imaging, 2021, 37(4): 1301. doi: 10.1007/s10554-020-02119-6 [12] 王斌, 李毅, 韩雅玲. 稳定性冠心病诊断与治疗指南[J]. 中华心血管病杂志, 2018, 46(9): 680. doi: 10.3760/cma.j.issn.0253-3758.2018.09.004 [13] SUGIYAMA T, ICHIKAWA-SEKI M, SATO H, et al. Enzyme-linked immunosorbent assay(ELISA) using recombinant Fasciola cathepsin L1 for the diagnosis of human fasciolosis caused by Fasciola hepatica/gigantica hybrid type[J]. Parasitol Intern, 2021, 82(1): 102311. [14] HARRY L, PAGE JR. The Judkins technique[J]. Catheterization and Cardiovasc Diagn, 1979, 5(2): 187. doi: 10.1002/ccd.1810050214 [15] CADER FA, KHAN SR. Feasibility of transradial multi-vessel percutaneous coronary intervention to both left and right coronary arteries by using Judkins left as a multipurpose guiding catheter[J]. Clin Med(London, England), 2020, 20(2): s102. [16] SMITH SC, DOVE JT, JACOBS AK. ACC/AHA guidelines for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(Committee to Revise the 1993 Guidelines for Percutaneous Transluminal Coronary Angioplasty)[J]. Circulation, 2001, 103(24): 3019. doi: 10.1161/01.CIR.103.24.3019 [17] MATOS LCV, CARVALHO LS, MODOLO R, et al. Gensini score and thrombus burden add predictive value to the SYNTAX score in detecting no-reflow after myocardial infarction[J]. Arq Bras Cardio, 2021, 116(3): 466. [18] ANTMAN EM, COHEN M, BERNINK P, et al. The TIMI risk score for unstable angina/non-ST-elevation MI: a method for prognostication and therapeutic decision making[J]. JAMA, 2000, 284(7): 835. doi: 10.1001/jama.284.7.835 [19] VERMA S, SHARMA A, ZINMAN B, et al. Empagliflozin reduces the risk of mortality and hospitalization for heart failure across Thrombolysis In Myocardial Infarction Risk Score for Heart Failure in Diabetes categories: Post hoc analysis of the EMPA-REG OUTCOME trial[J]. Diabetes Obes Metab, 2020, 22(7): 1141. doi: 10.1111/dom.14015 [20] ZHAO Y, ZHANG J. Clinical implication of homocysteine in premature acute coronary syndrome female patients: Its distribution and association with clinical characteristics and major adverse cardiovascular events risk[J]. Medicine(Baltimore), 2021, 100(18): e25677. [21] WANG C, WANG C, LIU M, et al. Temporal and spatial trends of ischemic heart disease burden in Chinese and subgroup populations from 1990 to 2016: socio-economical data from the 2016 global burden of disease study[J]. BMC Cardiovasc Disord, 2020, 20(1): 243. doi: 10.1186/s12872-020-01530-0 [22] DIXON SJ, LEMBERG KM, LAMPRECHT MR, et al. Ferroptosis: an iron-dependent form of nonapoptotic cell death[J]. Cell Cambridge Ma, 2012, 149(5): 1060. [23] DOLL S, FREITAS FP, SHAH R, et al. FSP1 is a glutathione-independent ferroptosis suppressor[J]. Nature, 2019, 575(7784): 14. [24] YAN Y, LEI G, GAN B. A mTORC1-mediated cyst(e)ine sensing mechanism governing GPX4 synthesis and ferroptosis[J]. Mol Cell Oncol, 2021, 8(3): 1919006. doi: 10.1080/23723556.2021.1919006 [25] FRIEDMANN JP, SCHNEIDER M, PRONETH B, et al. Inactivation of the ferroptosis regulator Gpx4 triggers acute renal failure in mice[J]. Nat Cell Biol, 2014, 16(12): 1180. doi: 10.1038/ncb3064 [26] BOGDAN AR, MIYAZAWA M, HASHIMOTO K, et al. Regulators of iron homeostasis: new players in metabolism, cell death, and disease[J]. Trends Biochem Sci, 2016, 41(3): 274. doi: 10.1016/j.tibs.2015.11.012 [27] FENG Z, MIN L, CHEN H, et al. Iron overload in the motor cortex induces neuronal ferroptosis following spinal cord injury[J]. Redox Biol, 2021, 43(1): 101984. [28] LU D, XIA Q, YANG Z, et al. ENO3 promoted the progression of NASH by negatively regulating ferroptosis via elevation of GPX4 expression and lipid accumulation[J]. Ann Transl Med, 2021, 9(8): 661. doi: 10.21037/atm-21-471 [29] XU C, SUN S, JOHNSON T, et al. The glutathione peroxidase Gpx4 prevents lipid peroxidation and ferroptosis to sustain Treg cell activation and suppression of antitumor immunity[J]. Cell Rep, 2021, 35(11): 109235. doi: 10.1016/j.celrep.2021.109235 [30] LI WY, LENG Y, XIONG Y, et al. Ferroptosis is involved in diabetes myocardial ischemia/reperfusion injury through endoplasmic reticulum stress[J]. DNA Cell Biol, 2020, 39(2): 210. doi: 10.1089/dna.2019.5097 [31] 沈兰, 陆言巧, 汪莉, 等. TIMI评分和GRACE评分系统对中国非ST段抬高型心肌梗死患者院内事件的评估价值[J]. 第二军医大学学报, 2020, 41(9): 1005. [32] 邵艳艳, 邵名亮, 彭徳清, 等. 基于质量管理工具的护理模式对冠心病介入治疗病人生活质量及心血管不良事件的影响[J]. 蚌埠医学院学报, 2021, 46(8): 1122. -

 点击查看大图
点击查看大图
图(3)表(3)
计量
- 文章访问数: 4308
- HTML全文浏览量: 1832
- PDF下载量: 116
- 被引次数: 0
