

-
胆源性急性胰腺炎(biliogenic acute pancreatitis, BAP)的发生涉及消化酶的作用、微循环的改变、胰管屏障的破坏等病理生理学过程,临床结局差异较大,多数病人可能仅有腹胀、腹痛等不适,但部分症状严重者往往会发展至多器官衰竭甚至死亡[1]。因此,临床上寻找能够预测BAP预后的标志物,从而早期对预后较差的病人实施必要的干预,显得十分重要。血小板淋巴细胞比值(platelet to lymphocyte ratio, PLR)和中性粒淋巴细胞比值(neutrophil to lymphocyte ratio, NLR)是临床上通过血常规即可获取的免疫炎症标志物,现有的研究[2-5]证据表明,二者与胃癌、肝癌、膀胱癌等肿瘤预后密切相关。然而二者与BAP相关研究较少,本研究探讨PLR、NLR与BAP病人预后之间的关系,以期为临床中BAP的诊治提供帮助。
-
选取2015年1月至2020年1月在我院首诊的338例BAP病人。其中急性胰腺炎诊断至少满足以下3条中的2条: (1)急性胰腺炎的特征性腹痛特征;(2)血清淀粉酶和/或脂肪酶大于正常值3倍以上;(3)符合急性胰腺炎的影像学特征性表现。乙醇、高脂血症、自身免疫等其他原因引起胰腺炎除外;复发性胰腺炎、慢性胰腺炎、合并创伤、肿瘤或肝功能衰竭除外;近期抗生素治疗、输血等影响血常规检查结果病例除外。其中男142例, 女196例;年龄22~90岁;>60岁140例,≤60岁198例。所有研究通过电话、书信、邮件等方式随访100 d或至死亡日期。随访期间,存活317例,死亡21例。研究所有回顾性资料均获取于我院病案系统。所有研究对象发病24 h内接受血常规、生化、血清淀粉酶等常规检查并且档案资料保存完整。
-
根据病人入院后的血常规结果计算PLR和NLR,同时分析年龄、性别、血清淀粉酶等临床病理参数与二者的关系。体质量指数(BMI)定义为体质量千克数(kg)除以身高米数平方(m2)。WHO将BMI≤18.5 kg/m2认定为体质量过轻,本研究统计过程中将BMI按>18.5 kg/m2和≤18.5 kg/m2转化为二分类变量。血细胞计数资料均来自于病人发病24 h内我院血常规检查。PLR=血小板计数/淋巴细胞计数,NLR=中性粒细胞计数/淋巴细胞计数。以病人随访生存状态为结局指标绘制PLR和NLR的受试者工作特征(receiver operating curve,ROC)曲线,选取约登指数最大时的值为截断值。根据截断值将病人分为高PLR/NLR组(PLR/NLR值>截断值)和低PLR/NLR组(PLR/NLR值≤截断值)。
-
采用χ2检验和Fisher′s确切概率法。ROC曲线取PLR和NLR的截断值,曲线下面积(AUC)的比较采用Z检验。应用Kaplan-Meier法和Cox多因素回归模型进行生存分析。
-
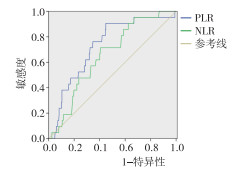
以病人的随访期间病人生存状态为判定依据,PLR的最佳临界值为344.7,AUC为0.787;NLR的最佳临界值为17.8,AUC为0.655(见图 1)。PLR和NLR的AUC比较,PLR的诊断价值高于NLR,差异有统计学意义(Z=2.03,P < 0.05)。
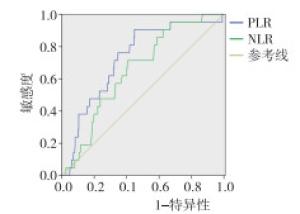
图 1 PLR和NLR对胆源性急性胰腺炎病人的ROC曲线
-
以PLR和NLR最佳临界值将病人分为PLR高组(PLR>344.7)165例和PLR低组(PLR≤344.7)173例,NLR高组(NLR>17.8)149例和NLR低组(NLR≤17.8)189例。PLR和NLR均与病人性别、年龄、体质量指数、高血压、糖尿病等临床参数无关(P>0.05)。但在高NLR组血清淀粉酶升高的病人比例高于低NLR组,差异有统计学意义(P < 0.01)(见表 1)。
临床病理参数 NLR χ2 P PLR χ2 P NLR≤17.8 NLR>17.8 PLR≤344.7 PLR>344.7 年龄/岁 ≤60
>6086
63112
770.08 >0.05 100
7398
670.09 >0.05 性别 男
女80
6995
940.39 >0.05 87
8688
870.31 >0.05 BMI 低
高115
34146
430.002 >0.05 128
45133
325.22 >0.05 血清淀粉酶/(U/L) >405
≤40576
73132
5711.65 < 0.01 99
74109
562.44 >0.05 糖尿病 无
有123
26162
270.63 >0.05 149
24139
290.88 >0.05 高血压 无
有126
23151
381.22 >0.05 137
36140
251.83 >0.05 表 1 PLR和NLR与BAP病人临床特征之间的关系(n)
-
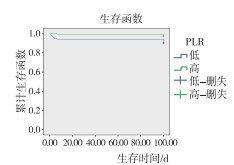
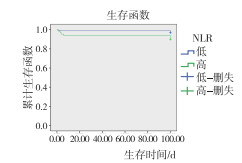
高PLR组平均生存时间为93.43 d(95%CI: 90.89~97.86),低于低PLR组平均生存时间99.43 d(95%CI: 98.15~100.72),差异有统计学意义(χ2=8.062, P < 0.01)(见图 2)。高NLR组平均生存时间为94.16 d(95%CI: 90.33~97.99.00),低于低NLR组平均生存时间98.96 d(95%CI: 97.38~100.53),差异有统计学意义(χ2=6.876, P < 0.01)(见图 3)。Kaplan-Meier法分析结果提示PLR和NLR影响BAP病人预后。以100 d随访生存时间和生存状态(死亡=0,生存=1)作为因变量,以年龄(>60=0, ≤60=1)、性别(男= 0,女=1)、BMI(>18.5kg/m2=0,≤18.5 kg/m2=1)和血清淀粉酶(>405=1,≤405=2)、NLR(低=0,高=1)和PLR(高=0,低=1)等临床特征为自变量进行Cox等比例风险模型分析,结果表明PLR、NLR与病人预后有关系,其中低PLR病人死亡风险是高PLR病人死亡风险的3.551倍(95%CI: 1.161~10.868);高NLR病人死亡风险是低NLR病人死亡风险的2.769倍(95%CI: 1.039~7.397)(见表 2)。
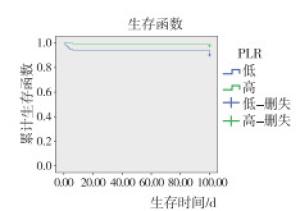
图 2 PLR与急性胰腺炎病人总生存率关系
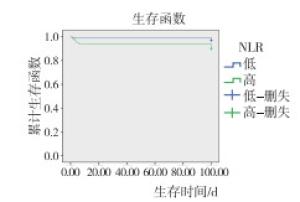
图 3 NLR与BAP病人总生存率关系
临床病理参数 B SE Waldχ2 HR 95%CI P NLR 1.025 0.501 4.179 2.769 1.039~7.397 < 0.05 PLR 1.266 0.571 4.908 3.551 1.161~10.868 < 0.05 表 2 BAP病人多因素生存分析
-
BAP是临床上最常见的急性胰腺炎类型,临床上寻找预测BAP病人预后的标志物,提前干预高风险病人的病程发展有着重要意义。中性粒细胞和淋巴细胞是白细胞的重要组成部分,在急性胰腺炎的病程进展中发挥着重要作用。急性胰腺炎发病过程中,血小板能够通过血小板活化因子、血小板微粒、趋化因子等因素参与和放大炎症反应,引起组织及器官损伤。本研究发现PLR和NLR与BAP病人生存相关,并且PLR预测BAP病人生存较NLR更为准确。
AZAB等[6]最早将NLR应用于急性胰腺炎方面研究,研究结果表明当NLR < 4.7时急性胰腺炎病人具有更低的ICU住院率和更短的住院时间。随后,国外学者[7]研究了NLR与急性胰腺炎死亡率的关系,但统计结果并没有明显差异。然而我国学者ZHANG等[8]研究表明,NLR ≥ 11是急性胰腺炎预后的独立危险因素,并且提示更高的持续性器官衰竭发生率和更高的死亡率。NLR与BAP病人预后之间的关系报道较少,本文研究了NLR与BAP病人生存预后之间的关系,结果表明NLR是BAP预后的独立影响因素;当NLR>17.8时,死亡风险较高。目前,高NLR提示BAP病人死亡风险增加的具体原因尚不明确。有研究[9-10]表明,较低的中性粒细胞数值往往提示急性胰腺炎病人预后较好。最早有研究[11]表明淋巴细胞的数值对急性胰腺炎疾病严重程度有一定的评估价值。随后,TAKEYAMA等[12]发现重症急性胰腺炎病程中的免疫损伤能够引起淋巴细胞的坏死、减少,并且与急性胰腺炎并发症相关。因此,中性粒细胞计数增加或者淋巴细胞计数相对或者绝对减少(NLR升高)可能提示急性胰腺炎病人预后较差。本研究观察到其中高NLR组血淀粉酶升高3倍以上的比例明显高于低NLR组,可能是BAP病人早期就诊病例较多,淀粉酶早期升高明显,具有一定特异性,但当胰腺组织出现坏死后,部分病人淀粉酶水平与正常值无明显差异。
PLR作为临床常用的免疫炎症标志物,其与良恶性肿瘤、急性胰腺炎等疾病预后关系研究一直是热点问题[13-15]。WANG等[15]回顾性分析了110例高脂血症性急性胰腺炎病人的临床资料,研究了PLR、NLR和RDW与高脂血症性急性胰腺炎预后之间的关系,结果表明PLR不是高脂血症性急性胰腺炎预后的独立影响因素。CHO等[16]回顾性分析了134例结石性急性胰腺炎和109例酒精性急性胰腺炎资料,结果表明NLR和PLR与结石性急性胰腺炎的严重程度相关。ZHOU等[17]研究表明PLR能够预测急性胰腺炎程度和死亡率,但预测价值较红细胞分布宽度低。然而PLR与BAP病人生存预后的关系尚未见报道,本文研究了PLR与BAP病人存预后之间的关系,结果表明PLR是BAP生存预后的独立影响因素;当PLR>344.7时,死亡风险较高。同时,PLR预测价值较NLR高。本研究中高PLR组病人预后较差原因尚未可知,可能与血小板在急性胰腺炎发展过程中作用及淋巴细胞的减少有关。血小板作为外周血的有形成分,最初的研究多集中在维持血管壁完整性、止血、伤口愈合等方面,随着研究的深入,血小板与胰腺炎的作用机制被逐渐揭示。血小板能够通过产生血小板活化因子、血小板微粒等成分驱化炎症细胞聚集、浸润,放大炎症反应,引起肿瘤坏死因子、白细胞介素、黏附分子等炎症因子的大量释放,引起内皮细胞损伤,进一步造成组织和器官损害[18-19]。
本研究仍存在一定的局限性。首先此次研究为单中心、小样本的研究,可能因样本量问题造成统计学偏倚。其次,急性胰腺炎病程进展极为复杂,不同时间点外周血指标改变显著,单次抽血结果预测最终结局存在一定的偶然性,本研究为回顾性研究,未能做重复抽血结果的统计。未来仍需大样本、多中心、前瞻性、重复性的临床资料验证其可靠性。
综上所述,PLR和NLR是预测急性胰腺炎死亡率的潜在标志物,能够从血常规中获取,不增加病人经济负担,进一步验证后有在临床上有广泛推广使用的潜力。
血小板淋巴细胞比值、中性粒淋巴细胞比值与胆源性急性胰腺炎病人预后的关系
Relationship between platelet to lymphocyte ratio, neutrophil to lymphocyte ratio and prognosis of patients with biliogenic acute pancreatitis
-
摘要:
目的研究血小板淋巴细胞比值(PLR)、中性粒淋巴细胞比值(NLR)与胆源性急性胰腺炎病人预后关系, 并比较二者在预测胆源性急性胰腺炎预后中的价值。 方法回顾性分析2015年1月至2020年1月338例首诊的胆源性急性胰腺炎病人临床资料, 利用受试者工作特征曲线(ROC)得出PLR与NLR最佳界值; 比较不同水平PLR和NLR病人的临床特征, 分析胆源性急性胰腺炎预后的危险因素。 结果以生存状态为依据PLR最佳界值为344.7, NLR的最佳界值为17.8。PLR的ROC曲线下面积(AUC)大于NLR (Z=2.03, P < 0.05)。多因素Cox回归模型表明, 低PLR病人死亡风险是高PLR病人死亡风险的3.551倍(95%CI: 1.161~10.868);高NLR病人死亡风险是低NLR病人死亡风险的2.769倍(95%CI: 1.039~7.397)。 结论PLR和NLR可能与胆源性急性胰腺炎预后相关。与NLR相比, PLR预测急性胰腺炎预后更加准确。 Abstract:ObjectiveTo study the relationship between platelet to lymphocyte ratio(PLR), neutrophil to lymphocyte ratio(NLR) and the prognosis of patients with biliogenic acute pancreatitis, and to compare their value in predicting the prognosis of biliogenic acute pancreatitis. MethodsThe clinical data of 338 patients with biliogenic acute pancreatitis diagnosed first time from January 2015 to January 2020 were retrospectively reviewed.Receiver operating curve(ROC) was used to determine the best critical value of PLR and NLR.The clinical features of patients with different levels of PLR and NLR were compared and the prognostic risk factors of biliogenic acute pancreatitis were explored. ResultsThe best critical values of PLR and NLR were 344.7 and 17.8, respectively according to the survival status of patients.The area under ROC curve(AUC) of PLR was bigger than NLR(Z=2.03, P < 0.05).Multivariate Cox regression model showed that the death risk of patients with low PLR was 3.551 times higher than that in patients with high PLR(95%CI: 1.161-10.868), and the risk of death in patients with high NLR was 2.769 times higher than that in patients with low NLR(95%CI: 1.039-7.397). ConclusionsPLR and NLR may be related to the prognosis of biliogenic acute pancreatitis.Compared with NLR, PLR is more accurate in predicting the prognosis of biliogenic acute pancreatitis. -
表 1 PLR和NLR与BAP病人临床特征之间的关系(n)
临床病理参数 NLR χ2 P PLR χ2 P NLR≤17.8 NLR>17.8 PLR≤344.7 PLR>344.7 年龄/岁 ≤60
>6086
63112
770.08 >0.05 100
7398
670.09 >0.05 性别 男
女80
6995
940.39 >0.05 87
8688
870.31 >0.05 BMI 低
高115
34146
430.002 >0.05 128
45133
325.22 >0.05 血清淀粉酶/(U/L) >405
≤40576
73132
5711.65 < 0.01 99
74109
562.44 >0.05 糖尿病 无
有123
26162
270.63 >0.05 149
24139
290.88 >0.05 高血压 无
有126
23151
381.22 >0.05 137
36140
251.83 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 BAP病人多因素生存分析
临床病理参数 B SE Waldχ2 HR 95%CI P NLR 1.025 0.501 4.179 2.769 1.039~7.397 < 0.05 PLR 1.266 0.571 4.908 3.551 1.161~10.868 < 0.05
下载: 导出CSV
-
[1] BANKS PA, BOLLEN TL, DERVENIS C, et al. Classification of acute pancreatitis-2012: revision. The diagnosis of acute pancreatitis requires two of the following three features: and definitions by international consensus[J]. Gut, 2013, 62(1): 102. doi: 10.1136/gutjnl-2012-302779 [2] ZHANG LX, WANG ZJ, XU AM, et al. Can the neutrophil-lymphocyte ratio and platelet-lymphocyte ratio be beneficial in predicting lymph node metastasis and promising prognostic markers of gastric cancer patients?Tumor maker retrospective study[J]. Internat J Surg, 2018, 56(8): 320. [3] ZHANG W, WANG R, MA W, et al. Systemic immune-inflammation index predicts prognosis of bladder cancer patients after radical cystectomy[J]. Ann Transl Med, 2019, 7(18): 431. doi: 10.21037/atm.2019.09.02 [4] WANG D, BAI N, HU X, et al. Preoperative inflammatory markers of NLR and PLR as indicators of poor prognosis in resectable HCC[J]. Peer J, 2019, 14(7): e7132. [5] LIN JX, HUANG YQ, XIE JW, et al. Association of the age-adjusted Charlson Comorbidity Index and systemic inflammation with survival in gastric cancer patients after radical gastrectomy[J]. Eur J Surg Oncol, 2019, 45(12): 2465. doi: 10.1016/j.ejso.2019.07.010 [6] AZAB B, JAGLALL N, ATALLAH JP, et al. Neutrophil-lymphocyte ratio as a predictor of adverse outcomes of acute pancreatitis[J]. Pancreatology, 2011, 11(4): 445. doi: 10.1159/000331494 [7] GULEN B, SONMEZ E, YAYLACI S, et al. Effect of harmless acute pancreatitis score, red cell distribution width and neutrophil/lymphocyte ratio on the mortality of patients with nontraumatic acute pancreatitis at the emergency department[J]. World J Emerg Med, 2015, 6(1): 29. doi: 10.5847/wjem.j.1920-8642.2015.01.005 [8] ZHANG Y, WU W, DONG L, et al. Neutrophil to lymphocyteratio predicts persistent organ failure and in-hospital mortality in an AsianChinese population of acute pancreatitis[J]. Medicine, 2016, 95(37): e4746. doi: 10.1097/MD.0000000000004746 [9] XUE J, SHARMA V, HABTEZION A. Immune cells and immune-based therapy in pancreatitis[J]. Immunol Res, 2014, 58(2/3): 378. [10] ZHU L, CHEN G, XIA Q, et al. Use of band cell percentage as an early predictor of death and ICU admission in severe acute pancreatitis[J]. Hepatogastroenterology, 2010, 57(104): 1543. [11] PEZZILLI R, BILLI P, BELTRANDI E, et al. Circulating lymphocyte subsets in human acute pancreatitis[J]. Pancreas, 1995, 11(1): 95. doi: 10.1097/00006676-199507000-00010 [12] TAKEYAMA Y, TAKAS K, UEDA T, et al. Peripheral lymphocyte reduction in severe acute pancreatitis is caused by apoptotic cell death[J]. J Gastrointest Surg, 2000, 4(4): 379. doi: 10.1016/S1091-255X(00)80016-5 [13] 李剑昂, 韩序, 方圆, 等. 术前CA19-9联合血小板和淋巴细胞比值预测胰腺导管内乳头状黏液性肿瘤癌变风险的价值分析[J]. 中华外科杂志, 2019, 57(3): 170. [14] 王琦, 李建军, 孙坚萍, 等. 纤维蛋白原联合血小板-淋巴细胞比率对肝癌早期复发的预测价值[J]. 中华医学杂志, 2019, 99(35): 2781. doi: 10.3760/cma.j.issn.0376-2491.2019.35.013 [15] WANG Y, FUENTES HE, ATTAR BM, et al. Evaluation of the prognostic value of neutrophil to lymphocyte ratio in patients with hypertriglyceridemia-induced acute pancreatitis[J]. Pancreatology, 2017, 17(6): 893. doi: 10.1016/j.pan.2017.10.001 [16] CHO SK, JUNG S, LEE KJ, et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio can predict the severity of gallstone pancreatitis[J]. BMC Gastroenterol, 2018, 18(1): 18. doi: 10.1186/s12876-018-0748-4 [17] ZHOU H, MEI X, HE X, et al. Severity stratification and prognostic prediction of patients with acute pancreatitis at early phase: a retrospective study[J]. Medicine (Baltimore), 2019, 98(16): e15275. doi: 10.1097/MD.0000000000015275 [18] STOKES KY, GRANGER DN. Platelets: a critical link between inflammation and microvascular dysfunction[J]. J Physiol, 2012, 590(5): 1023. doi: 10.1113/jphysiol.2011.225417 [19] 陈珵, 徐侃. 血小板在炎症反应中作用的研究进展[J]. 海南医学, 2017, 28(4): 623. doi: 10.3969/j.issn.1003-6350.2017.04.035 -

 点击查看大图
点击查看大图
图(3)表(2)
计量
- 文章访问数: 4090
- HTML全文浏览量: 1855
- PDF下载量: 11
- 被引次数: 0
