

-
危险性急性上消化道出血(acute upper gastrointestinal bleeding,AUGIB)是指在24 h内大量上消化道出血导致血流动力学异常、器官功能衰竭,起病急、进展快、严重者可危及生命,是消化内科常见的危急重症。此类疾病占消化道出血比例约为15%~20%,病死率高[1]。临床上有多种评估AUGIB预后的评分,但在危险性AUGIB应用方面研究较少,如何更好地运用不同危险评分系统评估高危AUGIB病人预后显得尤为重要[2]。本研究回顾性分析299例危险性AUGIB病人的临床资料,探讨不同内镜前评分系统对其预后评估价值。现作报道。
-
选择2017年12月至2021年1月安徽医科大学第二附属医院收治的危险性AUGIB病人作为研究对象。纳入标准:急性失血,呕血和/或黑便,并伴有以下之一项:(1)心率>100次/分;(2)收缩压 < 90 mmHg;(3)血红蛋白(Hb) < 80 g/L;(4)存在因失血导致重要器官灌注不足的症状[3-4]。排除标准:临床资料不全,无法进行评分。
-
确诊为危险性AUGIB,将院内或30 d内死亡、再出血作为临床研究终点,记录病人预后转归情况。再出血判断:(1)新发呕血、黑便、血便;(2)充分补液、输血后周围循环衰竭改善不明显,或好转后又加重;(3)Hb或红细胞计数呈进行性下降;(4)补液和尿量充足情况下,血尿素氮持续升高;(5)复查内镜提示再出血[5]。输血指征:(1)显著血流动力学不稳定的病人; (2)Hb < 60 g/L,若病人≥65岁,合并心肌缺血或慢性阻塞性肺病等基础疾病,可考虑放宽指标[6]。
-
收集病人的基线资料,包括基本信息(如性别、年龄等)、临床症状、临床干预措施(如内镜检查、内镜下治疗、输血、介入治疗、外科治疗等)、治疗结局(如再出血、死亡等)。分析内镜检查时间对院内或30 d内死亡的影响。
-
根据入院24 h内的指标完成AIMS65[7]、Glasgow-Blatchford(GBS)[8]以及Pre-Rockall[9]评分系统。其中AIMS65包括5个变量:血浆白蛋白 < 30 g/L、收缩压 < 90 mmHg、意识改变、国际标准化比值(INR)>1.5以及年龄>65岁。GBS包括收缩压、Hb、血尿素氮、脉搏、晕厥、黑便、肝病、心力衰竭等指标。Pre-Rockall包括三项临床指标(年龄、休克状况、伴发疾病)。评价三种内镜前评分系统对危险性AUGIB病人预后(输血率、院内或30 d内再出血率和死亡率)的评估价值。
-
采用t检验、χ2检验和χ2分割检验,采用受试者工作特征(ROC) 曲线分析评估三种评分系统预测预后的能力,并用曲线下面积(AUC)来评估ROC曲线的准确性。
-
本研究最终共纳入危险性AUGIB病人299例,其中男223例(74.58%),女76例(25.42%); 年龄20~97岁。院内或30 d内死亡43例(14.38%),存活256例(85.62%)。主要症状为呕血(66.22%)、黑便(85.95%)和晕厥(8.03%)。既往史:肝硬化病史(26.76%),消化性溃疡病史(7.69%),高血压病史(26.76%),恶性肿瘤病史(10.37%),糖尿病病史(10.37%),口服阿司匹林(10.03%)、非甾体消炎药(5.69%)。
-
住院期间行胃镜检查236例(78.93%)。行胃镜检查病人病因方面排名前5位的是,十二指肠球部溃疡68例(28.81%),肝硬化并食管胃底静脉曲张破裂出血60例(25.42%),胃溃疡47例(19.92%),复合性溃疡13例(5.51%),胃恶性肿瘤12例(5.08%)。未行胃镜检查病人63例,根据既往病史推测肝硬化并食管胃底静脉曲张破裂出血23例(36.51%)。236例行胃镜检查病人中,行紧急胃镜0~12 h 48例(20.34%),13~24 h行胃镜检查45例(19.07%),24 h以后行胃镜检查143例(60.59%)。行紧急胃镜0~12 h的病人病死率高于行13~24 h和>24 h胃镜检查病人,差异有统计学意义(P < 0.05)(见表 1)。
检查时间 n 死亡 存活 病死率/% χ2 P 0~12 h 48 10 38 20.83 13~24 h
> 24 h45
1432
143
1424.44*
0.70*28.11 < 0.01 合计 236 13 223 5.51 χ2分割检验:与0~12 h组比较* P < 0.05 表 1 胃镜检查时间对危险性AUGIB病人死亡的影响(n)
首次胃镜即行内镜下治疗111例(47.03%),再出血行内镜下治疗12例(5.08%),内镜下治疗方式包括局部喷洒去甲肾上腺素23例(9.75%), 金属夹止血49例(20.76%), 黏膜下注射止血16例(6.78%), 套扎及硬化剂注射52例(22.03%),再出血数字减影血管造影术治疗3例(1.27%),再出血行手术治疗11例(4.66%)。
-
死亡组43例,存活组256例,院内或30 d内死亡组病人AMIS65、Pre-Rocall的评分值均高于存活组,差异均有统计学意义(P < 0.01),2组GBS评分差异无统计学意义(P>0.05)(见表 2)。
分组 n GBS AMIS65 Pre-Rocall 院内或30 d内死亡组 43 11.67±2.86 2.49±1.03 3.67±1.63 院内或30 d内存活组 256 11.64±2.66 1.18±0.91 1.70±1.58 t — 0.07 8.57 7.53 P — > 0.05 < 0.01 < 0.01 院内或30 d内再出血组 58 11.53±2.61 2.03±0.96 2.91±1.91 院内或30 d内未再出血组 241 11.67±2.70 1.21±0.96 1.76±1.60 t — 0.37 5.84 4.73 P — > 0.05 < 0.01 < 0.01 表 2 院内或30 d内不同临床结局与GBS、AMIS65、Pre-Rocall评分的关系(x ± s; 分)
-
再出血组58例,未再出血组241例,院内或30 d内再出血病人AMIS65、Pre-Rocall的评分值均高于未再出血组,差异均有统计学意义(P < 0.01),2组GBS评分差异无统计学意义(P>0.05)(见表 2)。
-
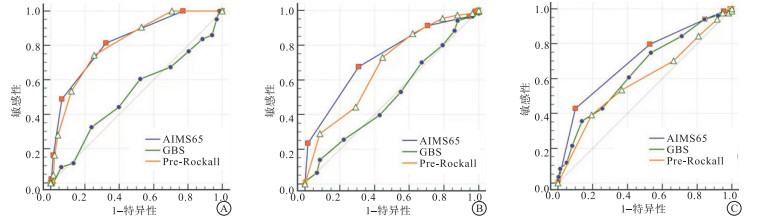
在预测院内或30 d内死亡率方面,AMIS65、Pre-Rocall、GBS评分系统的AUC分别为0.820、0.812、0.516,最优的是AMIS65,其次为Pre-Rocall,但二者之间差异无统计学意义(Z=0.17,P>0.05)。在预测院内或30 d内再出血方面,AMIS65、Pre-Rocall、GBS评分系统的AUC分别为0.729、0.676、0.511,最优的是AMIS65,其次为Pre-Rocall,但二者之间差异无统计学意义(Z=1.28,P>0.05)。在预测输血方面,AMIS65、Pre-Rocall、GBS评分系统的AUC分别为0.709、0.591、0.646,最优的是AMIS65,其次为GBS,但二者之间差异无统计学意义(Z=1.61,P>0.05)(见表 3、图 1)。
评分项目 AUC 95% CI 院内或30 d内死亡 AMIS65 0.820 0.771~0.861 Pre-Rocall 0.812 0.763~0.854 GBS 0.516 0.458~0.574 院内/30 d内再出血 AMIS65 0.729 0.675~0.778 Pre-Rocall 0.676 0.620~0.729 GBS 0.511 0.453~0.569 输血 AMIS65 0.709 0.654~0.759 Pre-Rocall 0.591 0.533~0.647 GBS 0.646 0.589~0.700 表 3 AIMS65评分、GBS评分、Pre-Rockall评分的AUC
图 1 AIMS65、GBS、Pre-Rockall预测院内30d内死亡、院内30d内再出血及输血的ROC曲线
-
危险性AUGIB临床表现主要为大量呕血、黑便及晕厥等,可因大量迅速出血导致循环衰竭、继发脏器功能损害[2]。近期我国一项大样本单中心回顾性病例分析[10]显示,上消化道出血发病呈上升趋势,男性多于女性,前3位的出血病因为消化性溃疡特别是十二指肠球部溃疡、食管胃底静脉曲张破裂出血及上消化道恶性肿瘤出血。本研究发现危险性AUGIB多见于老年男性病人,经胃镜检查,出血病因首位为十二指肠球部溃疡,其次为肝硬化并食管胃底静脉曲张破裂出血,与文献报道一致。
胃镜检查在上消化道出血的诊断、危险分层及治疗中有重要作用[11]。急诊胃镜对于出血的定位及定性有着重要价值。早期胃镜检查是否影响病人的预后,尤其是高危病人,内镜检查时机是一个有争议的问题。我国急性上消化道出血诊治指南[1]推荐大多数上消化道出血病人应在出血24 h内血流动力学稳定后尽快行急诊内镜检查。有研究[12]报道紧急内镜检查对降低急性非静脉曲张性出血病人的死亡率没有益处。在一项361例病人的回顾性队列研究[13]中发现,接受紧急内镜检查的病人不良结果(包括死亡、再出血、手术或放射干预或反复内镜治疗)的风险增加了5倍以上。本研究发现在危险性AUGIB病人中,行紧急胃镜(0~12 h)的病人病死率高于行13~24 h和>24 h胃镜检查的病人,可能与本研究纳入的病人均为高危病人,部分为恶性肿瘤晚期复发病人有关。
危险性AUGIB病人需要早期进行精准化治疗,否则可能危及生命,因此准确、及时评估预测病人的预后十分重要。目前常用早期内镜检查前风险评分系统主要有AIMS65、Pre-Rockall、GBS评分系统,但对其临床价值研究结论并不一致。其中Pre-Rockall评分不包括内镜,为Rockall评分去除内镜检查指标,简单易行,主要用于内镜前评估,在预测病死率与再出血方面,与Rockall评分具有同样的预测价值[9]。LU等[7]提出AIMS65评分是最方便的UGIB预后评分用于预测住院死亡率。CHANG等[14]亦提出无论是静脉曲张出血还是非静脉曲张出血,AIMS65在预测住院死亡率方面价值最好。涂家红等[3]指出在预测高危出血病人院内死亡或30 d内病死率方面,Pre-Rockall和AIMS65评分具有很好的价值。本研究发现对于危险性AUGIB病人,在预测院内/30 d内死亡率及再出血率方面,AMIS65、Pre-Rocall评分均具有较好的预测价值,两项评分之间并不存在显著差异。GBS评分于2000年提出[8], 其特点是灵敏度高,不涉及内镜检查结果,适用于门诊病人,对于风险极低的出血病人价值较高,对高风险出血病人作用有限,但一项大型多中心前瞻性研究[15]指出,GBS评分是预测病死率的最佳评分系统。本研究发现GBS评分在预测院内或30 d内死亡率及再出血率方面预测价值比较差,这可能与本研究纳入的病人在就诊时即有休克和/或Hb < 80 g/L,为高危病人有关。与李嘉嫦等[4]对危险性AUGIB病人研究结果一致。在预测输血方面,三种评分的AUC均不高,预测能力较差。赵宁宁等[16]也提出Pre-Rockall、GBS、AIMS65评分系统对于临床干预治疗预测不理想,仍需创建使用新的评分系统进行评估。
综上所述,行紧急胃镜的病人病死率高于非紧急胃镜检查的病人,但本研究为单中心、回顾性研究,入组病例不多,仍需进一步扩大样本量分析。AMIS65及Pre-Rocall评分在预测院内死亡或30 d内死亡率及再出血率方面价值较高,适用于危险性AUGIB的内镜检查前风险评估,便于临床推广。
三种内镜前评分系统对危险性急性上消化道出血预后评估的比较
Comparison of three pre-endoscopic scoring systems for prognosis evaluation of high risk acute upper gastrointestinal bleeding
-
摘要:
目的探讨三种内镜前评分系统AIMS65、Glasgow-Blachford(GBS)及Pre-Rockall在危险性急性上消化道出血(AUGIB)病人预后中的评估价值。 方法回顾性分析299例危险性AUGIB病人的临床资料,回顾诊断及治疗结局。以院内死亡或30 d内死亡、再出血为终点指标,绘制ROC曲线,比较曲线下面积(AUC),评估三种评分系统对预后的评估价值。 结果299例危险性AUGIB病人,行紧急胃镜(0~12 h)的病人病死率高于行13~24 h和>24 h胃镜检查病人,差异存在统计学意义(P < 0.05)。在预测院内死亡/30 d内死亡率方面,AMIS65、Pre-Rocall、GBS评分系统的AUC分别为0.820、0.812、0.516,其中AMIS65最优,其次为Pre-Rocall,二种评分系统能力相当(P>0.05)。在预测院内/30 d内再出血方面,AMIS65、Pre-Rocall、GBS评分系统的AUC分别为0.729、0.676、0.511,其中AMIS65最优,其次为Pre-Rocall,二种评分系统能力相当(P>0.05)。在预测输血方面,AMIS65、Pre-Rocall、GBS评分系统的AUC分别为0.709、0.591、0.646,其中AMIS65最优,其次为GBS,二种评分系统能力相当(P>0.05)。 结论AIMS65、Pre-Rockall能准确预测病人死亡率及再出血率,适用于危险性AUGIB的内镜前风险评估。 -
关键词:
- 急性上消化道出血 /
- AIMS65评分 /
- Pre-Rockall评分 /
- Glasgow-Blachford评分
Abstract:ObjectiveTo explore the prognostic value of three pre-endoscopic scoring systems AIMS65, Glasgow-Blachford(GBS) and Pre-Rockall in patients with high risk acute upper gastrointestinal bleeding(AUGIB). MethodsClinical data of 299 patients with high risk AUGIB were retrospectively analyzed, and the diagnosis and treatment outcome were reviewed.The death in hospital or death and rebleeding within 30 days were taken as the study endpoints.The ROC curve was draw, and area under the curve(AUC) was compared.Clinical values among the three scores were evaluated by ROC and AUC. ResultsThe mortality of patients undergoing emergency gastroscopy in 0-12 h was higher than patients undergoing emergency gastroscopy in 13-24 h and >24 h(P < 0.05).In predicting in-hospital death or 30-day mortality, the AUC of AMIS65, Pre-Rocall and GBS were 0.820, 0.812 and 0.516, respectively, the AMIS65 was best, followed by Pre-Rocall, there were no significant differences between the two scored(P>0.05).In predicting in-hospital or 30-day rebleeding, the AUC of AMIS65, Pre-Rocall and GBS were 0.729, 0.676 and 0.511, respectively, the AMIS65 was best, followed by Pre-Rocall, there were no significant differences between the two scored(P>0.05).In predicting blood transfusion, the AUC of AMIS65, Pre-Rocall and GBS were 0.709, 0.591 and 0.646, respectively, the AMIS65 was best, followed by GBS, there were no significant differences between the two scored(P>0.05). ConclusionsAIMS65 and Pre-Rockall can accurately predict the mortality rate and rebleeding rate of patients, which are suitable for pre-endoscopic assessment of high risk AUGIB. -
Key words:
- acute upper gastrointestinal bleeding /
- AIMS65 /
- Pre-Rockall /
- Glasgow-Blachford
-
表 1 胃镜检查时间对危险性AUGIB病人死亡的影响(n)
检查时间 n 死亡 存活 病死率/% χ2 P 0~12 h 48 10 38 20.83 13~24 h
> 24 h45
1432
143
1424.44*
0.70*28.11 < 0.01 合计 236 13 223 5.51 χ2分割检验:与0~12 h组比较* P < 0.05  下载: 导出CSV
下载: 导出CSV
表 2 院内或30 d内不同临床结局与GBS、AMIS65、Pre-Rocall评分的关系(x ± s; 分)
分组 n GBS AMIS65 Pre-Rocall 院内或30 d内死亡组 43 11.67±2.86 2.49±1.03 3.67±1.63 院内或30 d内存活组 256 11.64±2.66 1.18±0.91 1.70±1.58 t — 0.07 8.57 7.53 P — > 0.05 < 0.01 < 0.01 院内或30 d内再出血组 58 11.53±2.61 2.03±0.96 2.91±1.91 院内或30 d内未再出血组 241 11.67±2.70 1.21±0.96 1.76±1.60 t — 0.37 5.84 4.73 P — > 0.05 < 0.01 < 0.01
下载: 导出CSV
表 3 AIMS65评分、GBS评分、Pre-Rockall评分的AUC
评分项目 AUC 95% CI 院内或30 d内死亡 AMIS65 0.820 0.771~0.861 Pre-Rocall 0.812 0.763~0.854 GBS 0.516 0.458~0.574 院内/30 d内再出血 AMIS65 0.729 0.675~0.778 Pre-Rocall 0.676 0.620~0.729 GBS 0.511 0.453~0.569 输血 AMIS65 0.709 0.654~0.759 Pre-Rocall 0.591 0.533~0.647 GBS 0.646 0.589~0.700
下载: 导出CSV
-
[1] 中国医师协会急诊医师分会. 急性上消化道出血急诊诊治流程专家共识[J]. 中国急救医学, 2015, 35(10): 865. doi: 10.3969/j.issn.1002-1949.2015.10.001 [2] 胡佳辰. 危险性消化道出血的急诊临床诊治与临床思维[J]. 中国急救医学, 2017, 37(5): 467. doi: 10.3969/j.issn.1002-1949.2017.05.019 [3] 涂家红, 张明清, 赵斌. 危险性急性上消化道出血141例临床诊治分析[J]. 中华急诊医学杂志, 2018, 27(5): 518. doi: 10.3760/cma.j.issn.1671-0282.2018.05.012 [4] 李嘉嫦, 吕菁君, 姜洁, 等. 不同内镜前评分方法对危险性急性上消化道出血的预后评估价值[J]. 中国急救医学, 2019, 39(2): 124. doi: 10.3969/j.issn.1002-1949.2019.02.006 [5] 急性非静脉曲张性上消化道出血诊治指南(2015年, 南昌)[J]. 中华消化内镜杂志, 2015, 32(12): 787. [6] QUACH DT, DAO NH, DINH MC, et al. The performance of a modified Glasgow Blatchford Score in predicting clinical interventions in patients with acute nonvariceal upper gastrointestinal bleeding: a vietnamese propective multicenter cohort study[J]. Gut Liver, 2016, 10(3): 375. [7] LU X, ZHANG X, CHEN H. Comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems for the prediction of the risk of in-hospital death among patients with upper gastrointestinal bleeding[J]. Rev Esp Enferm Dig, 2020, 112(6): 467. [8] BLATCHFORD O, MURRAY WR, BLATCHFORD M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage[J]. Lancet, 2000, 356(9238): 1318. doi: 10.1016/S0140-6736(00)02816-6 [9] PARK SM, YEUM SC, KIM BW, et al. Comparison of AIMS65 Score and other scoring systems for predicting clinical outcomes in koreans with nonvariceal upper gastrointestinal bleeding[J]. Gut Liver, 2016, 10(4): 526. doi: 10.5009/gnl15153 [10] 王锦萍, 崔毅, 王锦辉, 等. 上消化道出血15年临床流行病学变化趋势[J]. 中华胃肠外科杂志, 2017, 20(4): 425. doi: 10.3760/cma.j.issn.1671-0274.2017.04.012 [11] HEARNSHAW SA, LOGAN RF, LOWE D, et al. Use of endoscopy for management of acute upper gastrointestinal bleeding in the UK: results of a nationwide audit[J]. Gut, 2010, 59(8): 1022. doi: 10.1136/gut.2008.174599 [12] KIM SS, KIM KU, KIM SJ, et al. Predictors for the need for endoscopic therapy in patients with presumed acute upper gastrointestinal bleeding[J]. Korean J Intern Med, 2019, 34(2): 288. doi: 10.3904/kjim.2016.406 [13] SUNG JJ, CHIU PW, CHAN FKL, et al. Asia-Pacific working group consensus on non-variceal upper gastrointestinal bleeding: an update 2018[J]. Gut, 2018, 67(10): 1757. doi: 10.1136/gutjnl-2018-316276 [14] CHANG A, OUEJIARAPHANT C, AKARAPATIMA K, et al. Prospective comparison of the AIMS65 Score, Glasgow-Blatchford Score, and Rockall Score for predicting clinical outcomes in patients with variceal and nonvariceal upper gastrointestinal bleeding[J]. Clin Endosc, 2021, 54(2): 211. doi: 10.5946/ce.2020.068 [15] ABOUGERGI MS, CHARPENTIER JP, BETHEA E, et al. A prospective, multicenter study of the AIMS65 score compared with the glasgow-blatchford score in predicting upper gastrointestinal hemorrhage outcomes[J]. J Clin Gastroenterol, 2016, 50(6): 464. doi: 10.1097/MCG.0000000000000395 [16] 赵宁宁, 苏争艳, 孙超, 等. 四种评分系统对急性非静脉曲张性上消化道出血预后评估的应用研究[J]. 中华消化内镜杂志, 2018, 35(4): 248. doi: 10.3760/cma.j.issn.1007-5232.2018.04.005 -

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 2377
- HTML全文浏览量: 1171
- PDF下载量: 11
- 被引次数: 0
