

-
脓毒症为全身性的炎症反应,主要引起有效循环血容量不足、循环障碍等情况[1],严重时可引起多器官功能衰竭,是临床上危重症病人死亡的重要原因之一[2]。流行病学调查显示其死亡率25%~45%[3],治疗十分棘手。因此,早期预测脓毒症病情变化对病人预后有重要意义。目前临床上常用的监测指标有C反应蛋白、降钙素原、血乳酸(blood lactic acid,LAC)等,能一定程度上反映体内炎症反应程度及病情进展情况,但对体内组织缺血缺氧情况反映较差,容易漏筛部分病人。在李周山等[4]的研究中证实了降钙素原和LAC的异常升高可用于评估脓毒血症病人病情的严重程度和治疗效果,但需要动态监测,且受环境及肝功能等的影响,使得应用受限。APACHE Ⅱ评分包括急性生理评分、年龄评分及慢性健康评分,是评价急性疾病严重度的重要指标,广泛应用于危重病病情分类及预后预测,但受评价者主观影响较大,容易导致结果偏差。
动脉-中心静脉血氧含量差[C(a-cv)O2]、中心静脉-动脉血二氧化碳分压差[P(cv-a)CO2]主要通过动静脉血中氧气及二氧化碳的分压差值反映组织供氧和二氧化碳排出的情况[5]。其中,中心静脉-动脉二氧化碳分压差与动脉-中心静脉血氧含量差比值[P(cv-a)CO2/C(a-cv)O2]对于识别无氧代谢有较高的敏感度和特异性[6],能很好地反映出组织灌注情况及机体内缺氧程度[7],且反应速度快、受外界因素影响小,目前在脓毒血症中应用越来越广泛,但因需要专业人员置管,导致操作困难,在评估病情恶化中应用较少。我院观察了169例脓毒症病人的P(cv-a)CO2/C(a-cv)O2及与病人预后的关系,推断了两者的相关性。现作报道。
-
将2015-2019年我院重症医学科收治的脓毒症病人169例进行回顾性分析,所有病人均为住院病例,根据病人治疗后的预后情况分为良好组(n=121)和恶化组(n=48)。纳入标准:(1)符合脓毒症的相关诊断标准[8];(2)年龄≥18岁,住院时间≥3 d;(3)临床资料完整并已完成相关操作。排除标准:(1)孕妇或入组后24 h死亡的病人;(2)不能放置中心静脉导管或有输血禁忌证的病人。
-
所有病人均为入组24 h内放置的中心静脉导管(选择部位包括颈内静脉或者锁骨下静脉)。肝素冲管后用2 mL针管抽取中心静脉血及股动脉血各1 mL(由操作熟练并具有资格的本科室医生进行),采用美国沃芬的血气生化分析仪(GEM Premier 3000) 测中心静脉、动脉血气分析及LAC水平;同时抽取手臂处静脉血,使用日本希森美康血细胞分析仪(Sysmex XT-4000i)查血常规,采用美国强生全自动干式生化分析仪(VITROS4600)监测血生化、肝功能、肾功能、血脂、感染性指标等项目。详细询问了家属现病史、既往史、家族史及感染部位等情况。监测病人体温、心率、血压等基本生命体征,评估APACHEⅡ评分[9]。病人均按照脓毒症治疗指南[2]给予相应治疗及对症治疗,并动态记录治疗中各个阶段的中心静脉和动脉血气分析、LAC、中心静脉压(CVP)、出入量、尿量等项目。
-
(1) 病人一般资料:包括年龄、性别、体温、心率、APACHEⅡ评分等一般资料,其中APACHEⅡ评分[9]主要用来评定疾病严重程度,评分越高代表病情越重,预后越差,死亡率越高。(2)实验室指标:包括肝功能、肾功能、血常规、炎症指标等,如白细胞(white blood cell,WBC)、降钙素原(procalcitonin,PCT)、LAC、血小板计数(blood platelet,PLT)等;(3)治疗和用药情况;(4)动静脉血血气分析情况:测定SaO2、ScvO2、PaO2、PcvO2、PaCO2、PcvCO2,计算出:[P(cv-a)CO2]=PcvCO2-PaCO2、[C(a-cv)O2]=Hb×1.34×(SaO2-ScvO2)+(PaO2-PcvO2)×0.03及(P(cv-a)CO2/C(a-cv)O2)。
-
(1) 好转:病人体温、心率、血压等均控制在正常范围内,无需或小剂量应用升压药等血管活性药物,复查炎症指标较前下降、部分恢复正常,APACHEⅡ评分较前下降30%以上。(2)恶化:病人体温较前升高,心率增快或出现心律失常、心肌缺血等情况,血压控制不稳、持续大剂量应用血管活性药物,复查炎症指标较前升高,APACHEⅡ评分无降低甚至升高。
-
所有病人均采用同一专业团队的医护人员进行中心静脉导管放置,在相同的环境内并应用同一仪器检测相关项目。
-
采用χ2检验、t检验、多因素logistic回归分析和ROC曲线分析。
-
除恶化组APACHEⅡ评分明显高于好转组(P < 0.01)外,2组年龄、性别等其他一般资料差异均无统计学意义(P>0.05)(见表 1)。
项目 恶化组
(n=48)好转组
(n=121)t P 年龄/岁 68.39±14.93 72.02±11.14 1.73 >0.05 性别 男 31 79 0.01* >0.05 女 17 42 体温/℃ 37.64±1.13 37.25±1.20 1.94 >0.05 心率/(次/分) 99.43±20.42 97.13±21.02 0.65 >0.05 收缩压/mmHg 85.35±15.82 88.91±14.27 1.42 >0.05 舒张压/mmHg 60.03±10.55 60.59±9.74 0.33 >0.05 合并肝功损伤 6 18 0.16* >0.05 合并肾功能损伤 5 15 0.13* >0.05 APACHEⅡ评分/分 20.37±3.41 17.69±2.85 5.21 < 0.01 感染部位 肺部感染 25 62 腹盆腔感染 12 31 胆道感染 5 12 0.03* >0.05 泌尿系感染 4 11 其他 2 5 治疗情况 抗感染药 48 120 0.40* >0.05 血管活性药物 48 115 2.47* >0.05 机械辅助通气 43 96 3.17* >0.05 *示χ2值 表 1 一般资料在2组间的比较(x±s,n)
-
恶化组PCT、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2均高于好转组(P < 0.01),而C(a-cv)O2低于好转组(P < 0.01),其他指标在2组之间差异均无统计学意义(P>0.05)(见表 2)。
分组 n WBC/(×109/L) PCT/(ng/mL) CRP/(mg/L) LAC/(mmol/L) PLT/(×109/L) C(a-cv)O2/mL P(cv-a) CO2/mmHg P(cv-a)CO2/C(a-cv)O2(mmHg/mL) 恶化组 48 17.35±5.42 18.57±5.71 30.65±8.73 7.21±1.72 117.41±30.38 2.84±0.83 6.59±1.32 2.42±0.78 好转组 121 15.86±4.98 14.40±5.00 28.76±9.04 6.06±1.68 110.25±31.27 3.43±0.98 5.46±1.14 1.51±0.50 t — 1.71 4.69 1.24 3.99 1.35 3.68 5.55 9.01 P — >0.05 < 0.01 >0.05 < 0.01 >0.05 < 0.01 < 0.01 < 0.01 表 2 2组实验室指标对比(x±s,n)
-
以脓毒症病情恶化为因变量(是=1,否=0),APACHEⅡ评分和表 2中有统计学意义的实验室指标为自变量(自变量赋值为其实际值),进行多因素logistic回归分析显示,APACHEⅡ评分、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2是影响脓毒症病情恶化的独立危险因素(OR=1.310、3.787、2.526、12.650,P < 0.01)(见表 3)。
自变量 B SE Waldχ2 P OR(95%CI) APACHEⅡ评分 0.270 0.088 9.49 < 0.01 1.310(1.103~1.555) PCT 0.601 0.458 1.72 >0.05 1.823(13.743~23.478) LAC 1.332 0.447 8.86 < 0.01 3.787(6.576~8.098) C(a-cv)O2 -0.528 0.333 2.52 >0.05 0.590(0.307~1.132) P(cv-a)CO2 0.927 0.256 13.06 < 0.01 2.526(1.528~4.176) P(cv-a)CO2/C(a-cv)O2 2.538 0.560 20.50 < 0.01 12.650(4.217~37.945) 表 3 各因素影响脓毒症病情恶化的多因素logistic回归分析
-
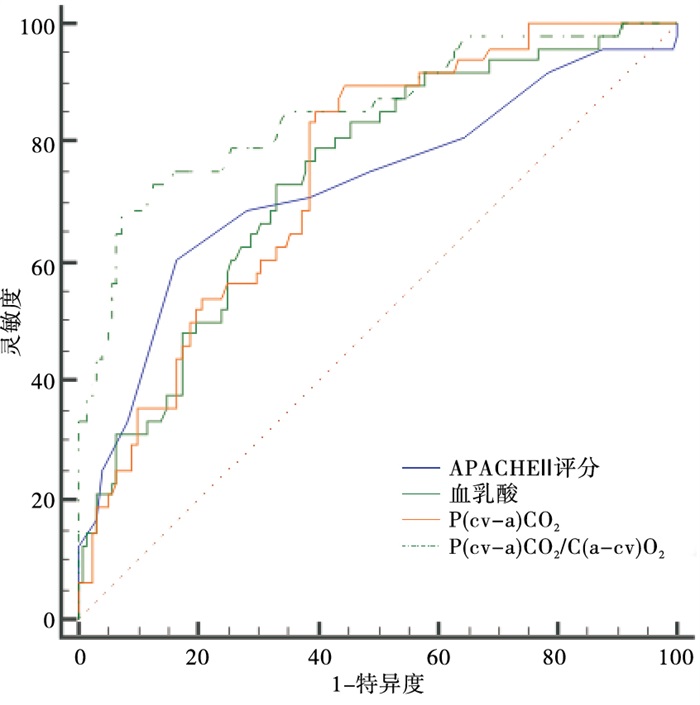
ROC曲线显示P(cv-a)CO2/C(a-cv)O2预测脓毒症病人病情恶化的诊断效能明显高于APACHEⅡ评分、LAC和P(cv-a)CO2的预测价值(P < 0.05),其最佳截点:>2.05 mmHg/mL,此时诊断的敏感性为72.93%、特异性为82.64%(见图 1、表 4)。

图 1 各因素预测脓毒症病人病情恶化的ROC曲线
变量 AUC SE 95%CI APACHE Ⅱ评分 0.728 0.047 2 0.654~0.793 LAC 0.742 0.041 1 0.669~0.806 P(cv-a)CO2 0.748 0.038 9 0.676~0.812 P(cv-a)CO2/C(a-cv)O2 0.851*△# 0.035 3 0.788~0.901 Z检验:与APACHEⅡ评分比较Z=2.01,*P < 0.05;与LAC比较Z=2.04,△P < 0.05;与P(cv-a)CO2/C(a-cv)O2比较Z=1.94,#P < 0.05 表 4 各因素预测脓毒症病人病情恶化的AUC
-
近年来,随着医学的快速发展,脓毒症病人住院的死亡率较前下降,但仍有30%左右的病人治疗效果不佳[11]。因此,早期快速而准确地预测脓毒血症病人预后情况,以便调整治疗方案改善预后,是目前研究的热点问题。
组织缺氧是导致脓毒症病人病情恶化的重要原因[12],目前临床上主要观察CRP、PCT等指标变化来指导治疗,其值的高低能反映出体内炎症反应的严重程度,对评价病情变化和治疗效果有一定的指导意义,但对判断早期组织缺氧作用局限,无法反映体内的氧合状态[13]。陈静波[14]研究表明了动态监测CRP联合PCT有助于早期筛查和评估脓毒症及其严重程度,但容易受心肾等器官功能不全的影响,而重症病人容易伴随各器官功能受损。而C(a-cv)O2主要是通过对比静脉血与动脉血中氧气含量的差值来判断组织中氧气供应是否充足、有无明显缺氧;P(cv-a)CO2比较的则是动脉血与静脉血中的二氧化碳分压差,可有助于判断组织中二氧化碳的生成和排出情况;P(cv-a)CO2/C(a-cv)O2则代表了体内的二氧化碳生成量及耗氧量比值,则可准确地反映出机体内组织的缺氧情况,而且反应迅速、影响因素少[15],对脓毒血症病情转归的判断有重要意义。
本研究中纳入研究的169例脓毒症病人,其中48例病人治疗后病情出现恶化,病情恶化发生率为28.40%。相关流行病学研究临床上有30%左右的脓毒血症病人会出现病情恶化[11],本文研究与之接近。这提示了早期预测病情的转归,及时调整治疗方案以提高预后对脓毒症病人有重要的意义。其中恶化组病人的A-PACHEⅡ评分明显高于好转组。说明入院时病人A-PACHEⅡ评分对病人病情判定有一定的意义,是目前重症医学科应用最广泛、最权威的危重症评价系统,可很好地判断病人目前状态和预测病死率[16],以便于客观制订及修正相关的医疗护理计划,对脓毒血症判断也有很重要的意义,其评分越高,病人状态越差、病情越严重。在温莉玲等[9]的研究指出APACHE Ⅱ评分能早期预测脓毒血症病情严重程度,评分越高病人预后越差,还能评估相应器官损伤情况,支持本研究观点。2组病人WBC、CRP等实验室指标对比无意义,但恶化组的PCT、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2均高于好转组,而恶化组C(a-cv)O2低于好转组。说明了脓毒血症病情恶化的病人其体内炎症反应更重、而控制更不容易,且其体内组织缺氧更严重。WBC和CRP虽然也能反映出体内炎症反应程度,但受外界影响较大、无特异性,不止在感染严重病人中升高,在重症病人在各种应激状态下也可导致上述指标的升高,在脓毒血症检查中无特殊意义,不能有效反映出体内炎症状态,故两组对比无差异。
研究[17]显示,PCT是细菌感染和脓毒血症的一个重要标志物,在诊断和治疗中具有重要价值,其水平越高,体内炎症越严重,病人病情越危重、预后越不良,本研究结果与之一致。而LAC作为体内组织一个无氧代谢的中间产物,主要反映组织缺氧情况,组织内氧气供应越少,进行的无氧代谢越多,LAC堆积越多,而LAC的堆积,又进一步加重了组织缺氧,形成了一个恶性循环,导致脓毒血症病人病情恶化。在石玉娜等[18]的研究中也指出了PCT和LAC对预测脓毒血症病人预后有重要意义,可反映出体内炎症反应的严重程度。而脓毒症由于全身炎症反应,导致组织低灌注和微循环障碍,进而导致各器官严重缺氧,引起多器官衰竭,主要用于判断脓毒血症病情严重程度。而C(a-cv)O2、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2则更直观地表现出组织内氧气、二氧化碳两者之间的关系,可有效地表现出组织供氧和二氧化碳的排出是否平衡,对判断脓毒症病人病情恶化有重要意义。其中P(cv-a)CO2/C(a-cv)O2是反映体内无氧代谢的指标,可预测病人的氧耗变化,侧面反映出局部组织循环供血情况。其比值越高,病人体内组织缺氧越严重,二氧化碳潴留越多,病人病情越重、恶化越快、死亡率越高。在HE等[19]的研究中,也证实了P(cv-a)CO2/C(a-cv)O2可评估LAC清除率,反应机体组织氧供情况,其值越高,体内组织缺氧越严重,病人病情恶化越快,是预测脓毒血症死亡率的一个独立性指标。而王雪婷等[20]的研究中也证实Lac和P(cv-a)CO2/C(a-cv)O2比值能准确地反映出组织缺氧情况,是脓毒性休克病人死亡的危险因素,可评估病人病情变化,本研究与之一致。
多因素logistic回归分析显示,APACHEⅡ评分、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2是影响脓毒症病情恶化的独立危险因素。ROC曲线显示:P(cv-a)CO2/C(a-cv)O2预测脓毒症病人病情恶化的诊断效能明显高于APACHEⅡ评分等项目。这表明了APACHEⅡ评分、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2都与脓毒症病人病情恶化有关,其中P(cv-a)CO2/C(a-cv)O2相关性更大,对脓毒症病情恶化的诊断意义最大。可准确指导临床治疗,有助于提高医疗服务质量、确定有效的治疗方案及确定最佳的出院时机,提供了客观的依据。
综上所述,P(cv-a)CO2/C(a-cv)O2能有效地预测脓毒症病人病情恶化的风险,有较高的临床应用价值。由于本文纳入病例数少,选取的病例质量不一,中心静脉导管置入术操作者和置入时间不能固定,研究的指标不全面,使得结果有偏差,今后需继续积累病例数量并严格控制病例质量和操作流程,进行更深入的探讨。
中心静脉-动脉血二氧化碳分压差/动脉-中心静脉血氧含量差与脓毒症发生病情恶化风险的相关性
Correlation between central vene-arterial partial pressure of carbon dioxide/artery-central venous oxygen content and the risk of sepsis
-
摘要:
目的分析中心静脉-动脉血二氧化碳分压差/动脉-中心静脉血氧含量差[P(cv-a)CO2/C(a-cv)O2]与脓毒症发生病情恶化风险的相关性。 方法将脓毒症病人169例根据治疗后的病情转归分好转组(n=121)和恶化组(n=48)。比较2组的一般资料、实验室指标等。应用多因素logistic回归分析各因素对脓毒症病人病情恶化的影响,应用ROC曲线分析P(cv-a)CO2/C(a-cv)O2等因素预测脓毒症病人病情恶化的价值。 结果2组年龄、性别、WBC、CRP等临床资料对比差异均无统计学意义(P>0.05)。恶化组APACHEⅡ评分、PCT、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2均高于好转组(P < 0.01),C(a-cv)O2低于好转组(P < 0.01)。多因素logistic回归分析显示,APACHEⅡ评分、LAC、P(cv-a)CO2和P(cv-a)CO2/C(a-cv)O2是影响脓毒症病人病情恶化的独立危险因素(P < 0.01)。ROC曲线显示,P(cv-a)CO2/C(a-cv)O2预测脓毒症病人病情恶化的诊断效能高于APACHEⅡ评分、LAC和P(cv-a)CO2的预测价值(P < 0.05),其最佳截点为>2.05 mmHg/mL,此时诊断的敏感性为72.93%、特异性为82.64%。 结论P(cv-a)CO2/C(a-cv)O2能有效预测脓毒症病人发生病情恶化的风险。 -
关键词:
- 脓毒症 /
- 动脉-中心静脉血氧含量差 /
- 中心静脉-动脉血二氧化碳分压差 /
- 血气分析
Abstract:ObjectiveTo analyze the correlation between the central venous-arterial partial pressure of carbon dioxide/artery-central venous blood oxygen content [P(cv-a)CO2/C(a-cv)O2] and the risk of sepsis. MethodsA total of 169 sepsis patients were divided into the improved group(n=121) and deteriorated group(n=48) according to the outcome of treatment.The general data and laboratory indicators of the two groups were compared.Multivariate logistic regression was used to analyze the effect of various factors on the deterioration of sepsis patients, and ROC curve was used to analyze the value of P(cv-a)CO2/C(a-cv)O2 and other factors in predicting the deterioration of sepsis patients. ResultsThere was no significant difference in age, gender, WBC, CRP and other clinical data between the two groups(P>0.05).But the APACHEⅡ score, PCT, LAC, P(cv-a)CO2 and P(cv-a)CO2/C(a-cv)O2 in the deteriorated group were higher than those in improved group(P < 0.01), and C(a-cv)O2 was lower than that in the improved group(P < 0.01).Multiariable logistic regression analysis showed that the APACHEⅡ score, LAC, P(cv-a)CO2 and P(cv-a)CO2/C(a-cv)O2 was the independent risk factors affecting the progression of sepsis patients(P < 0.01).ROC curve showed that the effectiveness of P(cv-a)CO2/C(a-cv)O2 predicting the progression of the disease in the diagnosis of sepsis patients was significantly higher than the APACHEⅡ score, LAC and the predictive value of P(cv-a)CO2(P < 0.05), the best cutoff value was >2.05 mmHg/mL with the combined diagnostic sensitivity of 72.93%, specificity of 82.64%. ConclusionsP(cv-a)CO2/C(a-cv)O2 can effectively predict the risk of disease deterioration in patients with sepsis. -
表 1 一般资料在2组间的比较(x±s,n)
项目 恶化组
(n=48)好转组
(n=121)t P 年龄/岁 68.39±14.93 72.02±11.14 1.73 >0.05 性别 男 31 79 0.01* >0.05 女 17 42 体温/℃ 37.64±1.13 37.25±1.20 1.94 >0.05 心率/(次/分) 99.43±20.42 97.13±21.02 0.65 >0.05 收缩压/mmHg 85.35±15.82 88.91±14.27 1.42 >0.05 舒张压/mmHg 60.03±10.55 60.59±9.74 0.33 >0.05 合并肝功损伤 6 18 0.16* >0.05 合并肾功能损伤 5 15 0.13* >0.05 APACHEⅡ评分/分 20.37±3.41 17.69±2.85 5.21 < 0.01 感染部位 肺部感染 25 62 腹盆腔感染 12 31 胆道感染 5 12 0.03* >0.05 泌尿系感染 4 11 其他 2 5 治疗情况 抗感染药 48 120 0.40* >0.05 血管活性药物 48 115 2.47* >0.05 机械辅助通气 43 96 3.17* >0.05 *示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 2组实验室指标对比(x±s,n)
分组 n WBC/(×109/L) PCT/(ng/mL) CRP/(mg/L) LAC/(mmol/L) PLT/(×109/L) C(a-cv)O2/mL P(cv-a) CO2/mmHg P(cv-a)CO2/C(a-cv)O2(mmHg/mL) 恶化组 48 17.35±5.42 18.57±5.71 30.65±8.73 7.21±1.72 117.41±30.38 2.84±0.83 6.59±1.32 2.42±0.78 好转组 121 15.86±4.98 14.40±5.00 28.76±9.04 6.06±1.68 110.25±31.27 3.43±0.98 5.46±1.14 1.51±0.50 t — 1.71 4.69 1.24 3.99 1.35 3.68 5.55 9.01 P — >0.05 < 0.01 >0.05 < 0.01 >0.05 < 0.01 < 0.01 < 0.01
下载: 导出CSV
表 3 各因素影响脓毒症病情恶化的多因素logistic回归分析
自变量 B SE Waldχ2 P OR(95%CI) APACHEⅡ评分 0.270 0.088 9.49 < 0.01 1.310(1.103~1.555) PCT 0.601 0.458 1.72 >0.05 1.823(13.743~23.478) LAC 1.332 0.447 8.86 < 0.01 3.787(6.576~8.098) C(a-cv)O2 -0.528 0.333 2.52 >0.05 0.590(0.307~1.132) P(cv-a)CO2 0.927 0.256 13.06 < 0.01 2.526(1.528~4.176) P(cv-a)CO2/C(a-cv)O2 2.538 0.560 20.50 < 0.01 12.650(4.217~37.945)
下载: 导出CSV
表 4 各因素预测脓毒症病人病情恶化的AUC
变量 AUC SE 95%CI APACHE Ⅱ评分 0.728 0.047 2 0.654~0.793 LAC 0.742 0.041 1 0.669~0.806 P(cv-a)CO2 0.748 0.038 9 0.676~0.812 P(cv-a)CO2/C(a-cv)O2 0.851*△# 0.035 3 0.788~0.901 Z检验:与APACHEⅡ评分比较Z=2.01,*P < 0.05;与LAC比较Z=2.04,△P < 0.05;与P(cv-a)CO2/C(a-cv)O2比较Z=1.94,#P < 0.05
下载: 导出CSV
-
[1] 宋迎春, 任国庆. 降钙素原、动脉血乳酸水平及中心静脉-动脉血二氧化碳分压差(Pcv-aCO2)在脓毒症患者预后评估中的临床意义[J]. 吉林医学, 2018, 39(9): 1621. doi: 10.3969/j.issn.1004-0412.2018.09.008 [2] WIRZ Y, MEIER MA, BOUADMA L, et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: a patient-level meta-analysis of randomized trials[J]. Crit Care, 2018, 22(1): 191. doi: 10.1186/s13054-018-2125-7 [3] MESQUIDA J, SALUDES P, GRUARTMONER G, et al. Central venous-toarterial carbon dioxide difference combined with arterial-to-venous oxygen content difference is associated with lactate evolution in early septic shock[J]. Crit Care, 2015, 19: 126. doi: 10.1186/s13054-015-0858-0 [4] 李洲山, 程丹. 降钙素原异常升高预警早期脓毒血症的临床诊治分析[J]. 内科急危重症杂志, 2021, 27(1): 86. [5] CHOL JJ, MCARTHY MW. Novel applications for serum procalcitonin testing in clinical practice[J]. Expert Rev Mol Diagn, 2018, 18(1): 27. doi: 10.1080/14737159.2018.1407244 [6] 王中华, 温剑艺, 李汉彪, 等. 中心静脉-动脉血二氧化碳分压差对老年脓毒症患者预后的评估价值[J]. 中华危重病急救医学, 2018, 30(8): 727. doi: 10.3760/cma.j.issn.2095-4352.2018.08.003 [7] YANG S, QI H, KAN K, et al. Neutrophil extracellular traps promote hypercoagulability in patients with sepsis[J]. Shock, 2017, 47(2): 132. doi: 10.1097/SHK.0000000000000741 [8] 中国医师协会急诊医师分会, 中国研究型医院学会休克与脓毒症专业委员会. 中国脓毒症/脓毒性休克急诊治疗指南(2018)[J]. 感染、炎症、修复, 2019, 20(1): 3. doi: 10.3969/j.issn.1672-8521.2019.01.001 [9] 温莉玲, 陈家佳, 梁红丽. 尿NGAL、KIM-1联合APACHEⅡ评分对脓毒症急性肾损伤诊断及预后的价值[J]. 临床急诊杂志, 2019, 20(2): 110. [10] HASAN GM, AL-EYADHY AA, TEMSAH MA, et al. Feasibility and efficacy of sepsis management guidelines in a pediatric intensive care unit in Saudi Arabia: a quality improvement initiative[J]. Int J Qual Health Care, 2018, 30(8): 587. doi: 10.1093/intqhc/mzy077 [11] ONG DSY, FRENCKEN JF, KLEIN KLOUWENBERG PMC, et al. Short-course adjunctive gentamicin as empirical therapy in patients with severe sepsis and septic shock: A prospective observational cohort study[J]. Clin Infect Dis, 2017, 64(12): 1731. doi: 10.1093/cid/cix186 [12] LUKAS P, DURILA M, JONAS J, et al. Evaluation of thromboelastometry in sepsis in correlation with bleeding during invasive procedures[J]. Clin Appl Thromb Hemost, 2018, 24(6): 993. doi: 10.1177/1076029617731624 [13] OFOMA UR, DAHDAH J, KETHIREDDY S, et al. Case volume-outcomes associations among patients with severe sepsis who underwent interhospital transfer[J]. Crit Care Med, 2017, 45(4): 615. doi: 10.1097/CCM.0000000000002254 [14] 陈静波. C-反应蛋白、降钙素原对脓毒症患者早期诊断及病情评估的应用价值[J]. 国际检验医学杂志, 2020, 41(2): 242. doi: 10.3969/j.issn.1673-4130.2020.02.029 [15] MOUSTAFA AA, ANTONIOS MA, ABDELLATIF EM, et al. Association of lactate/albumin ratio level to organ failure and mortality in severe sepsis in a pediatric intensive care unit in Egypt[J]. Turk J Pediatr, 2018, 60(6): 691. doi: 10.24953/turkjped.2018.06.010 [16] 孟祥海, 章宏伟, 张淑兰. 重症肺炎患者预后和APACHEⅡ评分及降钙素原PCT水平变化的关系[J/CD]. 现代医学与健康研究电子杂志, 2018, 2(1): 30. [17] 张运君, 卓小岸, 周小曼, 等. 血清降钙素原、C-反应蛋白及乳酸对老年脓毒症患者的预后评估[J]. 中华老年多器官疾病杂志, 2018, 17(1): 47. [18] 石玉娜, 周晓燕, 王庆海, 等. 脓毒症患者血清降钙素原表达及其对预后的影响分析[J]. 国际检验医学杂志, 2018, 39(9): 1059. doi: 10.3969/j.issn.1673-4130.2018.09.010 [19] HE H, LONG Y, LIU D, et al. The prognostic value of central venousto-arterial CO2 difference/arterial-central venous O2 difference ratio in septic shock patients with central venous O2 saturation ≥ 80[J]. Shock, 2017, 48(5): 551. doi: 10.1097/SHK.0000000000000893 [20] 王雪婷, 高雪花, 曹雯, 等. 血乳酸联合中心静脉-动脉血二氧化碳分压差与动脉-中心静脉血氧含量差比值预测脓毒性休克患者预后的应用价值[J]. 中华危重病急救医学, 2020(1): 39. -

 点击查看大图
点击查看大图
图(1)表(4)
计量
- 文章访问数: 2408
- HTML全文浏览量: 1426
- PDF下载量: 10
- 被引次数: 0
