

-
胸腰椎骨质疏松性压缩性骨折(osteoporotic vertebral compression fracture, OVCF)是老年人经常发生的骨折,严重者可导致驼背畸形甚至死亡。临床上椎体成形术(percutaneous vertebroplasty, PVP)被广泛应用治疗该疾病,但笔者发现,对于椎体前壁有破裂的病椎,骨水泥的弥散和渗漏仿佛是一对矛盾体,弥散效果好容易出现渗漏,而没有渗漏往往弥散效果欠佳。鉴于此,我科设计了一种“补丁技术”,2019年1月至2021年10月,我们将此项新技术应用于前壁破裂的OVCF病人治疗,与传统PVP相比,术中术后均获得了满意的效果。现作报道。
-
选择2019年1月至2021年10月蚌埠医学院第一附属医院骨科收治的前壁破裂的OVCF病人72例。纳入标准:(1)年龄≥50岁且无肿瘤、感染、精神疾病疾病;(2)核磁共振显示为椎体前壁有破裂的新鲜性压缩性骨折,且椎管内没有骨块压迫脊髓或神经根;(3)单纯压缩性骨折且没有下肢神经症状的病人;(4)无外伤史或仅有轻微外伤史。其中男15例,女57例;年龄53~88岁;胸椎34例,腰椎38例。随机分为骨水泥在湿沙期注入病椎组(A组)、骨水泥在拉丝期注入病椎组(B组)、少量骨水泥在面团早期封闭椎体前壁破口然后湿沙期骨水泥推注组(C组),各24例。
-
A、B组手术方法区别仅为骨水泥推注时机不同(A组为湿沙期骨水泥,B组为拉丝期骨水泥),C臂机透视确定病椎穿刺进针点后,按顺序穿入导管器械一次性连续推注骨水泥。
C组术前仔细阅片,观察病椎前壁破裂的位置,在C臂机的透视下根据脊柱正位片上双侧椎弓根的影像解剖标志,局部麻醉后以双侧椎弓根影的外上缘作为穿刺进针点穿入,超过椎体后缘2 mm后拔出针芯,置入导针,再拔出外套管,将扩张器经导针穿入椎弓根,拔出导针,此时可根据椎体前壁破裂位置调整扩张器的方向再继续穿入,直至接近前壁破裂位置。取骨水泥粉剂一半及溶剂的一半进行混合,搅拌均匀后注入工作套管内,待骨水泥至面团早期,在C臂机监视下将工作套管插入扩张器至接近前壁破裂位置,开始缓慢推注面团早期的骨水泥1 mL,C臂机监视下此时骨水泥如“补丁”一般将前壁破裂处补上。接着将工作套管拔除丢弃,扩张器回退至椎体中部,然后将剩余一半的骨水泥粉剂和溶剂混合,搅拌均匀后注入新的工作套管,待骨水泥至湿沙期,将新的工作套管插入扩张器至椎体中部,在C臂机监视下推注,双侧各推注1.5~2 mL,待骨水泥硬化后拔出扩张器和工作套管,包扎切口。
3组病人均采用双侧穿入,推注速度基本相同,推注骨水泥量均为4~5 mL。
-
术后第1天,病人根据具体情况下床活动,并拍摄腰椎正侧位片复查,口服抗骨质疏松药物继续治疗。术后第2天,配合Oswestry脊柱功能障碍评分(ODI评分)调查术后疼痛缓解情况。
-
比较3组病人术后骨水泥渗漏率;3组病人分别在术前、术后2 d进行ODI评分,评估并比较术后疼痛缓解情况。
-
采用t检验、方差分析、q检验和χ2检验。
-
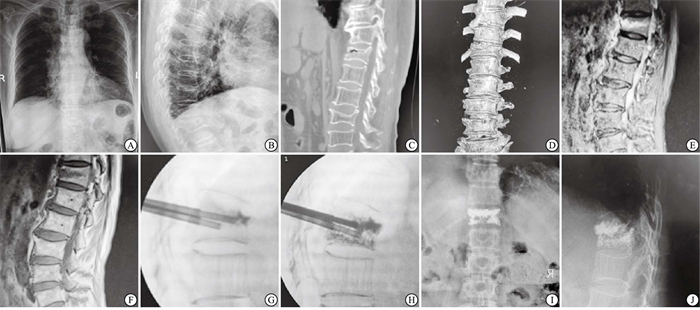
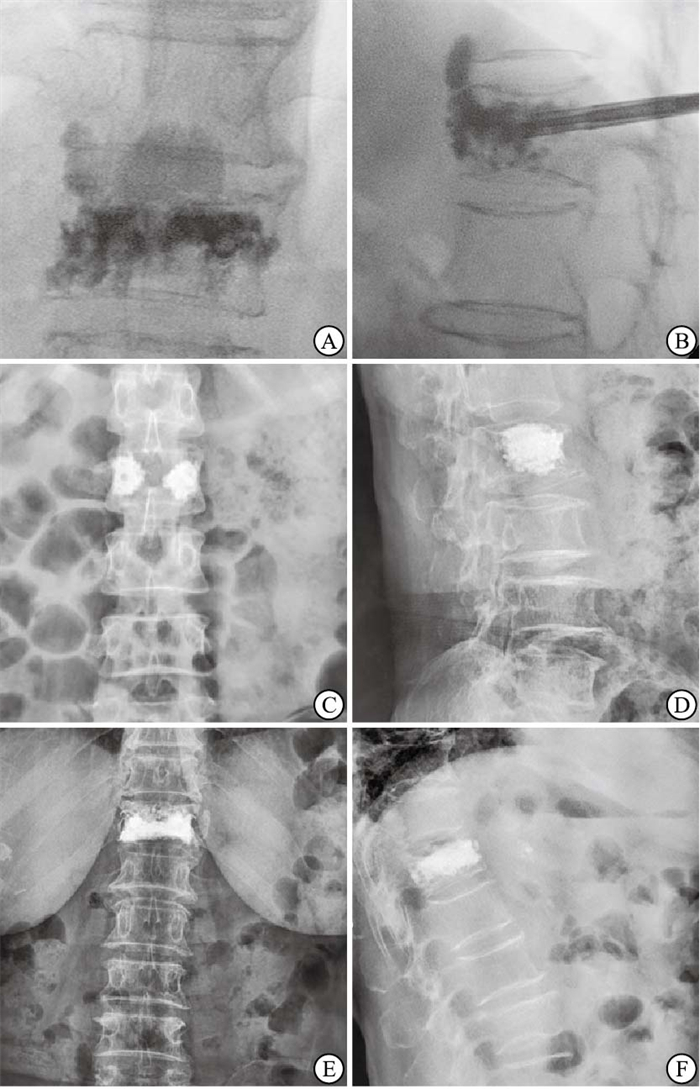
3组病人均顺利完成手术,其中骨水泥C型渗漏率为A组>B组>C组(P < 0.01)(见图 1、表 1),A、C组弥散状况均好于B组(见图 1)。3组病人术前ODI评分间差异无统计学意义(P>0.05);术后2 d,3组病人ODI评分均较术前明显降低(P < 0.01),且A组和C组均明显低于B组(P < 0.01),而A组与C组差异无统计学意义(P>0.05)(见表 2)。C组典型病例见图 2。

图 1 3组病人术中/术后胸腰段正侧位片
分组 n 骨水泥C型渗漏数 χ2 P A组 24 13(54.17) 16.02 < 0.01 B组 24 5 (20.83)** C组 24 1 (4.17)**## 与A组比较**P < 0.01;与B组比较##P < 0.01 表 1 3组病人术后骨水泥渗漏率比较[n;百分率(%)]
分组 术前 术后2 d t P A组 43.58±3.15 5.21±0.66 58.41 < 0.01 B组 44.00±2.40 8.46±0.93** 67.64 < 0.01 C组 43.88±3.75 4.88±0.80## 49.83 < 0.01 F 0.11 145.25 — — P >0.05 < 0.01 — — MS组内 9.915 0.647 — — q检验:与A组比较**P < 0.01;与B组比较##P < 0.01 表 2 3组病人手术前后ODI评分比较(n=24;x±s;分)

图 2 C组病人,女,69岁,T12椎体OVCF
-
骨水泥渗漏是PVP术最常见的并发症,根据国内外报道[1-3],其发生率可达24.4%~38.6%,而对于椎体前壁有破裂的压缩性骨折,渗漏率可能更高。骨水泥聚合过程分为湿沙期、拉丝期、面团期、硬化期。骨水泥渗漏可分为沿椎基底静脉渗漏至椎体后缘型(B型)、沿椎体骨壁裂口渗漏型(C型)、沿椎间静脉渗漏型(S型)[4]。B、S型渗漏可导致脊髓、神经受压或血管栓塞引起严重症状,椎体后壁破裂导致的C渗漏由于骨水泥会向椎管内渗漏引起脊髓神经压迫症状,往往被认为是PVP手术的相对禁忌症[4-5]。而本研究中探讨的椎体前壁破裂所导致的骨水泥向椎体前方渗漏,由于大多没有临床症状而往往被忽视,但如果骨水泥向前方渗漏过多,可能会对椎前大血管,包括腹主动脉、胸主动脉及下腔静脉,造成压迫或烧灼,引起严重后果[6]。
骨水泥渗漏的因素很多,主要包括[7-9]:(1)椎体骨折程度。椎体塌陷程度越重,渗漏概率越大,椎体骨皮质破裂会明显增加渗漏风险。(2)椎体骨质疏松程度。椎体骨质疏松越严重,发生渗漏的概率越大。(3)推注骨水泥的量。注射大量的骨水泥不会更好地减轻疼痛,反而会增加渗漏的风险,这与大量骨水泥使得病椎内压力异常增大有关,但注入骨水泥量过少会导致病椎内弥散不足,上下软骨终板得不到足够的强化支撑,可能会造成椎体高度丢失,笔者认为适量的骨水泥并且病椎内广泛弥散这种状态最好,一般认为胸腰段骨水泥推注4~5 mL,下腰椎推注6 mL左右为宜;(4)推注骨水泥的黏度和速度。推注骨水泥的黏度越低,流动性越大,弥散程度越好,但同时渗漏的可能越大,尤其是在椎体周围骨皮质破裂的情况下,同时,推注骨水泥的速度过快也会增加渗漏的风险,应缓慢推注,每推注0.2 mL透视一次,推注骨水泥时有落空感或压力突然减轻,应停止推注及时透视以防止更严重的渗漏。本研究中A组病人采用湿沙期骨水泥推注,由于湿沙期骨水泥黏度低,虽然术中骨水泥弥散效果很好,但渗漏率很高(52%),安全性较差。
学者们提出“明胶海绵填塞法”防止骨水泥渗漏的手术技巧[10],但有一定的局限性。具体操作是将明胶海绵剪成合适大小,通过漏斗装置和探针将其推送到椎体骨皮质破裂处,再推注骨水泥。实际操作有一定难度:首先,明胶海绵推送的手术过程较复杂;其次,明胶海绵不显影,C壁机透视无法确定其是否在骨折的位置;最后,明胶海绵缺少晚期骨水泥那种粘连性和稳定性,所以明胶海绵填塞法仍有一定的渗漏率。本研究中,C组病人采用“补丁技术”,将骨水泥两次制备,分次注射,首次推注的面团早期骨水泥类似“补丁”,封闭椎体前壁的破口防止渗漏,安全稳定且手术方式简单,第二次推注湿沙期骨水泥又保证了骨水泥在病椎内的弥散性。
-
前文已述及推注病椎内的骨水泥黏度越低,骨水泥在病椎内的弥散程度越好,这直接降低了术后发生椎体再骨折的概率。因为当骨水泥分布不均,局限于椎体内某处,此处的椎体强度明显提高,就会增加周围未弥散骨水泥的松质骨的Von Mises应力,最终导致周围椎体再骨折塌陷[11],而骨水泥充分弥散,能够充分均匀地强化病椎,重建椎体的生物力学性能,特别是当骨水泥能充分弥散至上下终板,能使病椎的强度提高8倍,最大程度地恢复病椎高度,预防后凸畸形[12]。也有研究[13]指出,充分骨水泥的填充会导致病椎的刚度异常增加,进而增加了临近椎体骨折的风险。我们认为,骨水泥充分弥散并不代表需要大量推注,适量的骨水泥如果弥散充分,一样能够接触上下终板,达到“顶天立地”的效果。本研究中B组病人推注拉丝期骨水泥,术后拍片病椎左右两侧的骨水泥没有相连,也没有接触到上下终板,并没有达到理想的弥散效果(见图 1C、D)。所以,骨水泥在病椎内的弥散程度与推注骨水泥的黏度息息相关。
PVP术后病人疼痛的缓解程度与注射骨水泥量没有直接关系,但与骨水泥弥散程度有关[14],这个结论在本研究中也得以体现:3组病人病椎内注射的骨水泥量基本相同,但是A、C组由于弥散充分,故术后疼痛感相较B组病人降低。这是因为当骨水泥充分填充骨小梁之间的孔隙,能够起到“锚固”的作用,最大程度地稳定断裂的骨小梁,疼痛即可得到有效缓解。同时骨水泥对病椎内的感觉神经末梢具有“消融作用”,也降低了疼痛感[15]。
-
(1) 扩张器要穿到椎体前壁接近骨折处,但不能穿破皮质,以免扩大椎体前壁的破口,同时也为了保护椎体前方的血管;(2)要等到面团早期再进行第一次推注,笔者的经验是拉丝期第一次推注很大概率会人为造成渗漏,而面团晚期推注阻力很大,很难达到满意效果,所以第一次推注的时机很重要;(3)第一次推注完毕后要立即将工作套管拔除,扩张器回退至椎体中间部位再二次制备骨水泥,以免面团期骨水泥硬化后扩张器难以回退或拔出。
综上,对于前壁有破裂的OVCF,传统PVP术无论湿沙期还是拉丝期推注,都有一定的局限性,而“补丁技术”能够在明显降低骨水泥渗漏率的基础上保证病椎内的骨水泥弥散效果,与传统PVP术对比优势明显。但由于“补丁技术”在我科临床上应用的例数仍不够多,其手术效果仍需要各级医院进一步推广验证。
PVP术中“补丁技术”对椎体前壁破裂的OVCF治疗效果
Effect of "patch technique" in PVP treatment on OVCF with anterior vertebral wall rupture
-
摘要:
目的探索椎体成形术(PVP)中“补丁技术”对于椎体前壁破裂的骨质疏松性压缩性骨折(OVCF)的应用方法和治疗效果。 方法选取拟行PVP手术治疗的椎体前壁破裂的OVCF病人72例,随机分为湿沙期骨水泥推注组(A组)、拉丝期骨水泥推注组(B组)、应用“补丁技术”组(面团早期骨水泥封闭椎体前壁破口,然后湿沙期骨水泥推注)(C组),各24例。术中均双侧穿入,推注速度基本相同,推注的骨水泥量均为4~5 mL。术后拍摄X线片,观察骨水泥的弥散情况和渗漏情况;3组病人术前、术后2 d进行ODI评分,评估疼痛缓解情况。 结果A组病人术后病椎骨水泥弥散状况佳,但发生C型渗漏高达13例(渗漏率54.17%);B组病人术后病椎骨水泥弥散状况欠佳,发生C型渗漏5例(渗漏率20.83%);C组病人术后病椎骨水泥弥散状况佳,且发生C型渗漏仅1例(渗漏率4.17%),3组渗漏率间差异有统计学意义(P < 0.01)。3组病人术前ODI评分间差异无统计学意义(P>0.05);术后2 d,3组病人ODI评分均较术前明显降低(P < 0.01),且A组和C组均明显低于B组,而A组与C组差异无统计学意义(P>0.05)。 结论PVP术中的“补丁技术”不仅有利于骨水泥在病椎内均匀分布,减少再骨折的发生,术后减轻疼痛效果好,且因其极低的渗漏率,手术安全性高。 -
关键词:
- 椎体成形术 /
- 骨质疏松性压缩性骨折 /
- 椎体前壁破裂 /
- 补丁技术 /
- 骨水泥C型渗漏
Abstract:ObjectiveTo explore the application and therapeutic effect of "patch technique" in percutaneous vertebroplasty (PVP) for osteoporotic vertebral compression fracture (OVCF) with rupture of the anterior vertebral body. MethodsA total of 72 OVCF patients with rupture of the anterior vertebral body who underwent PVP were selected.All patients were randomly divided into three groups, 24 cases in each group.Group A: bone cement injection during wet-sand phase, group B: bone cement injection during wire-drawing phase, group C: the "patch technique" was used to seal the fracture of the anterior vertebral body with bone cement in the early dough stage of paste, and then bone cement was injected in wet-sand phase.Both sides were penetrated during the operation, with basically same injection speed and 4-5 mL of bone cement volume for each side.Postoperative X-ray films were taken to observe the diffusion and leakage of bone cement.The pain relief of patients in the three groups was evaluated using the Oswestry disability index (ODI) before and 2 days post operation. ResultsIn group A, the cement in diseased vertebral body was relatively evenly distributed, while type-C leakage occurred in 13 cases (54.17%).In group B, the cement distribution in postoperative diseased vertebral body was relatively scattered, with 5 cases having type-C leakage(20.83%).In the group C, the cement in diseased vertebral body was relatively evenly distributed, there was only 1 case of type-C leakage(4.17%).There was significant difference in leakage rate among the three groups (P < 0.01).There was no significant difference in preoperative ODI scores among the three groups(P>0.05).On the second day after operation, the ODI scores of the three groups were significantly lower than those before operation (P < 0.01), and the ODI scores of group A and group C were significantly lower than those of group B, but there was no significant difference between group A and group C(P>0.05). ConclusionsThe "patch technique" in PVP is beneficial for the even distribution of bone cement in the diseased vertebral body, reducing the occurrence of re-fracture, and alleviating postoperative pain.In addition, due to the lower leakage rate, this technique shows higher safety. -
表 1 3组病人术后骨水泥渗漏率比较[n;百分率(%)]
分组 n 骨水泥C型渗漏数 χ2 P A组 24 13(54.17) 16.02 < 0.01 B组 24 5 (20.83)** C组 24 1 (4.17)**## 与A组比较**P < 0.01;与B组比较##P < 0.01  下载: 导出CSV
下载: 导出CSV
表 2 3组病人手术前后ODI评分比较(n=24;x±s;分)
分组 术前 术后2 d t P A组 43.58±3.15 5.21±0.66 58.41 < 0.01 B组 44.00±2.40 8.46±0.93** 67.64 < 0.01 C组 43.88±3.75 4.88±0.80## 49.83 < 0.01 F 0.11 145.25 — — P >0.05 < 0.01 — — MS组内 9.915 0.647 — — q检验:与A组比较**P < 0.01;与B组比较##P < 0.01
下载: 导出CSV
-
[1] ALHASHASH M, SHOUSHA M, BARAKAT AS, et al. Effects of polymethylmethacrylate cement viscosity and bone porosity on cement leakage and new vertebral fractures after percutaneous vertebroplasty: a prospective study[J]. Global Spine J, 2019, 9(7): 754. doi: 10.1177/2192568219830327 [2] ZHANG TY, ZHANG PX, XUE F, et al. Risk factors for cement leakage and nomogram for predicting the intradiscal cement leakage after the vertebra augmented surgery[J]. BMC Musculoskelet Disord, 2020, 21(1): 792. doi: 10.1186/s12891-020-03810-4 [3] 王龙, 李续. 骨质疏松性腰椎压缩性骨折行椎体成形术后骨水泥渗漏的危险因素分析[J]. 颈腰痛杂志, 2021, 42(5): 744. [4] CHEN WC, HUANG S, TSAI L, et al. Comparison between vertebroplasty with high or low viscosity cement augmentation or kyphoplasty in cement leakage rate for patients with vertebral compression fracture: a systematic review and network meta-analysis[J]. Eur Spine J, 2021, 30(9): 2680. doi: 10.1007/s00586-020-06636-9 [5] CAO PJ, HAO WM, ZHANG L, et al. Safety and efficacy studies of vertebroplasty with dual injections for the treatment of osteoporotic vertebral compression fractures: preliminary report[J]. Acad Radiol, 2020, 27(8): e224. doi: 10.1016/j.acra.2019.09.023 [6] 林宇洋, 张建新. 预防椎体成形术骨水泥渗漏研究进展[J]. 辽宁中医药大学学报, 2010, 12(4): 249. [7] 杨惠林, 干旻峰. 需要进一步强调的椎体强化术焦点问题[J]. 骨科临床与研究杂志, 2021, 6(5): 257. [8] 杨柳, 杜建伟. 椎体增强术中降低骨水泥渗漏率的措施[J]. 中国组织工程研究, 2021, 26(22): 3598. [9] HSIEH MK, KAO FC, CHIU PY, et al. Risk factors of neurological deficit and pulmonary cement embolism after percutaneous vertebroplasty[J]. J Orthop Surg Res, 2019, 14(1): 406. doi: 10.1186/s13018-019-1459-4 [10] 赵敏, 何承建. 经皮椎体成形术中应用明胶海绵预防骨水泥渗漏25例[J]. 中国骨科临床与基础研究杂志, 2019, 11(4): 216. [11] LIANG H, JI T, ZHANG Y, et al. Reconstruction with 3D-printed pelvic endoprostheses after resection of a pelvic tumour[J]. Bone J, 2017, 99B(2): 267. [12] 姚龚, 沈忆新, 李敏, 等. 骨水泥不同弥散方式对椎体成形术后生物力学影响的有限元分析[J]. 中国骨伤, 2021, 34(8): 732. [13] ZHANG H, XU C, ZHANG T, et al. Does percutaneous vertebroplasty or balloon kyphoplasty for osteoporotic vertebral compression fractures increase the incidence of new vertebral fractures?A meta-analysis[J]. Pain Physician, 2017, 20(1): E13. [14] LI C, ZHOU Y. Creation of a planned or central-clefted puncture combined with a second puncture during vertebroplasty to treat osteoporotic vertebral compression fractures with large clefts[J]. J Orthop Surg Res, 2020, 15(1): 535. [15] 刘志强, 周云龙, 雷飞, 等. 不同时相骨水泥推注对经皮椎体后凸成形术治疗骨质疏松性椎体压缩性骨折疗效的影响[J]. 中国修复重建外科杂志, 2020, 34(4): 435. -

 点击查看大图
点击查看大图
图(2)表(2)
计量
- 文章访问数: 2175
- HTML全文浏览量: 1022
- PDF下载量: 24
- 被引次数: 0
