

-
门静脉血栓(PVT)指在血栓形成于门静脉主干,肝内分支伴或不伴(脾静脉、肠系膜上静脉等)受累,是肝硬化的常见并发症之一,发病率为0.6%~26.0%[1-2]。研究[3-4]发现,PVT可导致门静脉闭塞或海绵样变性,加重门静脉高压,不仅导致顽固性腹水,增加食管静脉曲张破裂出血风险,还严重影响肝硬化食管静脉曲张病人的预后。因此,早期评估肝硬化食管胃静脉曲张破裂出血后门静脉系统血栓栓塞的发生风险,能够及早干预和调整治疗方案以改善肝硬化病人的预后。对于食管胃静脉曲张临床上需进行定期的镜下治疗,然而频繁的影像学检查不仅浪费医疗资源,还会加重病人的经济负担。因而,寻找一种能够预测肝硬化病人食管静脉曲张PVT发生风险的方法,对早期选择干预方案及判断病人预后具有重要意义。目前临床上针对肝硬化病人食管胃静脉曲张破裂出血后PVT形成相关因素的研究大多是从发病原因、影响因素等研究,且以单个因素评估高危病人,忽略了PVT的发生受多种因素的影响。因此,联合多个维度指标建立更客观的预测系统具有重要作用。本研究拟基于多因素分析筛选的风险因素以构建肝硬化病人食管胃静脉曲张破裂出血后PVT发生风险的列线图预测模型。
-
采用回顾性分析的方法,收集2014年1月至2021年1月我院收治的肝硬化伴食管胃底静脉曲张破裂病人448例。纳入标准:(1)根据肝硬化诊治指南[5]病史、影像学检查(腹部B超/肝硬度测定/CT/MRI)或组织病理证实为肝硬化;(2)内镜检查证实食管胃底曲张静脉活动性出血、渗血、喷射等活动性出血状态或食管胃底曲张静脉表面有近期出血征象,如有白色血栓、红色血栓、血凝块等[6];(3)首次住院,且住院前1个月内所有病人均行腹部CT/MRI或门静脉彩超检查证实无PVT形成;(4)有完整的随访资料。排除标准:(1)伴有其他系统的血栓形成;(2)合并严重的多器官功能障碍者;(3)既往在外院接受内镜止血治疗者;(4)合并恶性肿瘤、自身免疫系统及血液系统等疾病;(5)未住院复查或死亡者;(6)随访中,经影像学检查证实为门静脉系统癌栓。
-
将所纳入病人按照3:1的比例分为研究队列336例和112例,2队列再根据是否发生PVT分为血栓组和无血栓组,采用单因素分析和多因素回归分析筛选研究队列肝硬化病人食管胃静脉曲张破裂出血后发生PVT主要风险因素,采用RStudio软件中的rms程序包构建列线图并进行验证。入选病人的临床资料包括: (1)一般资料。性别、年龄、体质量指数(BMI);(2)既往病史。有无吸烟史,有无合并高血压、糖尿病及冠心病等基础疾病,有无NSBB治疗史、外科手术治疗史;(3)入院后检查。肝硬化类型、肝功能Child-Pugh分级、食管静脉曲张分级、有无腹水、消化道溃疡、内镜止血、门静脉内径、脾静脉内径、脾脏厚度;(4)实验室指标:白细胞计数(WBC)、血小板计数(PLT)、红细胞(RBC)、血红蛋白(Hb)、白蛋白(Alb)、纤维蛋白原(FIB)、总胆红素(TBIL)、凝血酶原时间(PT)、活化部分凝血活酶时间(APTT)、凝血酶时间(TT)、D-二聚体(D-D)、尿素氮(UN)、肌酐(Cr)、P-选择素、天门冬氨酸氨基转移酶(AST)、丙氨酸氨基转移酶(ALT)、总胆固醇(TC)、三酰甘油(TG)、国际标准化比值(INR)。通过查阅、检索、收集住院病历记录观察纳入病人从首次住院后的PVT情况,观察时间为3个月至3年,检查方法包括腹部CT/MRI或门静脉彩超等。
-
采用腹部增强CT或MRI以及门静脉彩超检查,依据检查结果(门静脉系统存在无血流信号或无强化的充盈缺损)确诊PVT。
-
采用t检验、χ2检验、logistic回归分析和ROC曲线分析。
-
研究队列与检验队列病人性别、年龄、BMI、肝硬化类型、肝功能Child-Pugh分级、食管静脉曲张分级等临床资料差异均无统计学意义(P>0.05)(见表 1)。
因素 研究队列
(n=336)检验队列
(n=112)t P 男性 189(56.25) 65(58.04) 0.11△ >0.05 年龄/岁 45.88±10.05 46.94±9.52 0.99 >0.05 BMI/(kg/m2) 23.67±2.96 23.81±3.11 0.43 >0.05 吸烟史 66(19.64) 20(17.86) 0.48△ >0.05 高血压 98(29.17) 36(32.14) 0.36△ >0.05 糖尿病 51(15.17) 19(16.96) 0.20△ >0.05 冠心病 8(2.38) 6(5.36) 2.46△ >0.05 NSBB治疗史 108(32.14) 30(26.79) 1.13△ >0.05 外科手术 103(30.65) 28(25.00) 1.30△ >0.05 肝硬化类型 病毒性 198(58.93) 74(66.07) 酒精性 103(30.65) 28(25.00) 1.81△ >0.05 其他 35(10.42) 10(8.93) 肝功能Child-Pugh分级 A级
B+C级121(36.01)
215(63.99)30(26.78)
82(73.21)3.20△ >0.05 食管静脉曲张分级 轻度 36(10.71) 15(13.39) 中度 40(11.91) 18(16.07) 2.18△ >0.05 重度 260(77.38) 79(70.53) 腹水 169(50.30) 70(62.50) 0.86△ >0.05 消化道溃疡 103(30.65) 31(27.69) 0.36△ >0.05 内镜止血 161(47.92) 58(51.79) 0.50△ >0.05 门静脉内径/mm 15.52±3.73 15.23±3.36 0.72 >0.05 脾静脉内径/mm 9.06±2.85 9.15±2.92 0.29 >0.05 脾脏厚度/mm 44.56±7.58 43.96±7.62 0.73 >0.05 WBC/(×109/L) 7.23±2.38 7.35±2.46 0.46 >0.05 PLT/(×109/L) 95.72±20.13 96.46±18.94 0.34 >0.05 RBC/(×1012/L) 2.90±0.77 3.01±0.82 1.29 >0.05 Hb/(g/L) 92.16±11.60 92.87±11.92 0.56 >0.05 Alb/(g/L) 26.91±6.02 27.25±5.90 0.52 >0.05 FIB/(g/L) 2.79±0.81 2.68±0.76 1.26 >0.05 TBIL/(mol/L) 72.56±18.42 71.89±19.01 0.33 >0.05 PT/s 16.97±3.95 16.70±3.79 0.88 >0.05 APTT/s 38.46±8.46 39.02±8.20 0.61 >0.05 TT/s 12.82±3.95 13.52±4.03 1.62 >0.05 D-D/(μg/L) 2.87±0.43 2.78±0.40 1.59 >0.05 UN/(mmol/L) 7.11±2.29 7.01±2.23 0.40 >0.05 Cr/(μmol/L) 72.16±5.80 72.43±6.21 0.42 >0.05 P-选择素/(ng/mL) 70.17±8.09 69.89±7.92 0.27 >0.05 ALT/(U/L) 86.97±22.70 85.83±23.34 0.46 >0.05 AST/(U/L) 56.79±17.42 55.99±17.50 0.68 >0.05 TG/(mmol/L) 1.46±0.31 1.41±0.37 1.08 >0.05 TC/(mmol/L) 4.98±1.22 5.01±1.34 0.18 >0.05 INR 2.78±0.80 3.03±0.78 2.88 < 0.01 △示χ2值 表 1 研究队列与检验队列的临床资料比较(x±s)
-
研究队列中77例(22.92%)发生PVT,其中出血后最快形成PVT者用时2周,49.35%(38/77)在1年内发生PVT,79.22%(61/77)在2年内合并PVT。检验队列中26例(23.21%)发生PVT,出血后最快形成PVT者用时12 d,50.00%(13/26)在1年内发生PVT,80.77%(21/26)在2年内合并PVT。单因素分析结果显示,研究队列PVT组与无PVT组肝功能Child-Pugh分级、门静脉内径、PLT、D-D、P-选择素、TG差异均有统计学意义(P < 0.05~P < 0.01)(见表 2)。
因素 PVT组
(n=77)无PVT组
(n=259)t P 男性 46(59.74) 143(55.21) 0.11△ >0.05 年龄/岁 46.47±10.13 47.22±9.86 0.58 >0.05 BMI/(kg/m2) 23.20±3.01 22.85±3.10 0.88 >0.05 吸烟史 18(23.38) 48(18.53) 2.29△ >0.05 高血压 29(37.66) 69(26.64) 3.49△ >0.05 糖尿病 17(22.08) 34(13.13) 3.69△ >0.05 冠心病 3(3.90) 4(1.54) 1.61△ >0.05 NSBB治疗史 30(38.96) 78(30.12) 2.13△ >0.05 外科手术 29(37.66) 74(28.57) 2.31△ >0.05 肝硬化类型 病毒性 49(63.63) 149(66.07) 酒精性 21(27.27) 82(31.66) 0.92△ >0.05 其他 7(9.09) 28(10.81) Child-Pugh分级 A级
B+C级19(24.68)
58(75.32)102(39.38)
157(60.62)5.57△ < 0.05 食管静脉曲张分级 轻度 8(10.39) 28(10.81) 中度 15(19.48) 25(9.65) 5.50△ >0.05 重度 54(70.13) 206(79.54) 腹水 40(50.30) 129(62.50) 0.11△ >0.05 消化道溃疡 27(30.65) 76(27.69) 0.91△ >0.05 内镜止血 42(47.92) 119(51.79) 1.76△ >0.05 门静脉内径/mm 18.16±4.50 13.04±3.22 11.11 < 0.01 脾静脉内径/mm 9.52±3.07 8.97±2.91 1.44 >0.05 脾脏厚度/mm 44.56±9.18 43.99±8.74 0.50 >0.05 WBC/(×109/L) 7.19±2.27 7.41±2.40 0.72 >0.05 PLT/(×109/L) 124.64±28.44 95.87±20.20 9.92 < 0.01 RBC/(×1012/L) 2.97±0.81 2.82±0.75 1.51 >0.05 Hb/(g/L) 92.71±13.52 92.08±12.89 0.37 >0.05 Alb/(g/L) 27.36±6.63 26.85±6.27 0.62 >0.05 FIB/(g/L) 2.80±0.83 2.72±0.79 0.77 >0.05 TBIL/(mol/L) 72.56±18.42 71.89±19.01 0.27 >0.05 PT/s 16.53±3.74 16.47±3.64 0.13 >0.05 APTT/s 38.96±8.33 40.11±8.51 1.05 >0.05 TT/s 12.82±3.95 13.52±4.03 1.34 >0.05 D-D/(μg/L) 2.93±0.43 2.26±0.39 12.92 < 0.01 UN/(mmol/L) 7.45±2.26 6.98±2.30 1.58 >0.05 Cr/(μmol/L) 72.55±5.78 73.46±6.33 1.13 >0.05 P-选择素/(ng/mL) 75.77±10.09 68.77±7.87 6.40 < 0.01 ALT/(U/L) 87.64±22.66 85.50±26.34 0.65 >0.05 AST/(U/L) 57.11±17.97 56.23±17.76 0.38 >0.05 TG/(mmol/L) 1.11±0.29 1.50±0.41 7.78 < 0.01 TC/(mmol/L) 5.14±1.33 5.05±1.13 0.59 >0.05 INR 2.89±0.81 3.08±0.76 1.90 >0.05 △示χ2值 表 2 研究队列肝硬化病人食管胃静脉曲张破裂出血后发生PVT的单因素分析(x±s)
-
将研究队列单因素分析中PVT组与无PVT组差异有统计学意义的因素作为自变量,将病人发生PVT作为因变量,纳入多因素logistic回归分析,分类变量肝功能Child-Pugh分级赋值:A级=0,B+C级=1,其余定量资料以实际值录入。多因素分析结果显示,肝功能Child-Pugh分级、门静脉内径、PLT、D-D、P-选择素、TG均为肝硬化病人食管胃静脉曲张破裂出血后PVT的风险因素(P < 0.01)(见表 3)。
变量 B SE Waldχ2 P OR 95%CI Child-Pugh分级 1.872 0.548 11.666 < 0.01 6.505 2.221~19.049 门静脉内径 0.394 0.707 32.099 < 0.01 1.484 1.294~1.700 PLT 0.038 0.010 14.791 < 0.01 1.039 1.019~1.059 D-D 0.999 0.258 14.937 < 0.01 2.716 1.636~4.507 P-选择素 0.078 0.025 9.342 < 0.01 1.081 1.028~1.136 TG -2.212 0.670 22.962 < 0.01 0.040 0.011~0.150 表 3 研究队列肝硬化病人食管胃静脉曲张破裂出血后发生PVT的多因素logistic回归分析
-
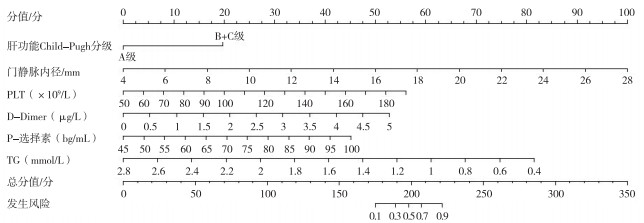
将多因素分析结果进行可视化处理,构建了列线图模型,该列线图由肝功能Child-Pugh分级、门静脉内径、PLT、D-D、P-选择素及TG 6个指标及其对应的线段组成(见图 1)。

图 1 肝硬化病人食管胃静脉曲张破裂出血后PVT的风险预测模型
-
在RStudio软件中对所构建模型进行研究队列与检验队列双重验证,ROC曲线分析结果显示,模型在研究队列的曲线下面积(AUC)为0.953(95%CI:0.931~0.976),灵敏度为81.8%,特异度为94.2%;检验队列的AUC为0.944(95%CI:0.904~0.984),灵敏度为98.9%,特异度为81.4%。
-
研究[7]显示,肝硬化并发食管胃静脉曲张破裂出血占肝硬化合并上消化道出血的50%~80%,起病急,极易出现失血性休克。PVT是肝硬化失代偿期严重并发症之一,研究[8-9]数据显示,肝硬化病人PVT发生率5%~36%,其中在失代偿期病人其发病率高达8%~25%,是肝硬化病人的负面预后因素。另有研究[10]显示,受到部分未规律复诊的非急性症状性PVT漏诊的影响,PVT真实患病率可能更高。因此,早期预测肝硬化病人食管胃静脉曲张破裂出血后PVT的风险,可为制定个体化治疗方案提供参考,对改善病人预后重大意义。
本研究收集448例肝硬化伴食管胃底静脉曲张破裂出血病人的临床资料进行分析,发现PVT发生率为22.99%(103/448),其中出血后最快形成PVT者用时12 d,49.51%(51/103)在1年内发生PVT,79.61%(82/103)在2年内合并PVT,这与既往研究[11]结果相似。在对研究队列进行多因素logistic回归分析中发现,肝功能Child-Pugh分级、门静脉内径、PLT、D-D、P-选择素、TG是肝硬化病人食管胃静脉曲张破裂出血PVT的风险因素。凝血因子主要在肝脏,是参与血液凝固过程的各种蛋白质组分。依赖维生素K的凝血因子(如Ⅰ、Ⅱ、Ⅶ、Ⅸ、Ⅹ、Ⅺ)、抗凝血酶Ⅲ和蛋白C等重要的纤维蛋白溶解因子等主要在肝脏合成,当Child-Pugh肝功能分级增高,此类因子及纤维蛋白原合成功能减退,组织纤溶酶原激活物清除能力减弱导致凝血-抗凝功能紊乱,造成血液流动减缓,血液呈高凝状态,从而引发PVT的形成[12-13]。正常的门静脉主干的内径范围为0.6~1.0 cm,随着门静脉压力的增加,门静脉将代偿性变宽,门静脉血流速度减缓,易致PVT形成[14]。因此,门静脉内径的宽度是临床上常用的反映门静脉高压的程度。DONG等[15]根据ROC曲线推测出预测PVT形成的最佳宽度为12.5 mm,若大于此宽度,则PVT形成的风险将呈显著性增加。PLT是血细胞中最小的细胞,参与凝血机制,主要来源于骨髓巨核细胞脱落的颗粒,具有黏附、聚集和释放各种促凝血因子等功能,在炎性反应、血栓形成、伤口愈合及器官移植排斥等生理病理过程中发挥着重要作用[16]。本研究结果中PLT是肝硬化病人食管胃静脉曲张破裂出血后PVT的风险因素,其机制可能是:血管受损时,胶原纤维暴露,PLT可黏附在血小管血管壁的内皮细胞在血管破裂口处形成血栓;血管破裂受损时,内源与外源性凝血系统被激活,受到刺激后的PLT通过释放其储存的物质来发生酶促反应,将可溶性FIB转化为不溶性纤维蛋白,形成的纤维蛋白互相交织,最终形成血凝块帮助止血;PLT活化后,细胞质内Ca2+浓度增加,在损伤的血管处,PLT通过释放各种促凝因子、血管收缩物质等,使血管闭合,血流量减少,促进血凝块收缩[17-18]。因此,临床上对于对肝硬化并发食管胃静脉曲张破裂出血尤其是肝功能Child-Pugh肝功能分级为B与C级病人,应定期测量门静脉内径或压力,密切检测PLT动态变化,早期预防,降低发生PVT的风险。D-D是经纤溶酶水解产生的一种特异性降解产物,由活化凝血酶从FIB转化而来,可反映纤维蛋白的血管内周转情况。D-D水平随着纤维蛋白溶解而升高,因而作为内源性纤溶指标的D-D可以预测PVT病人疾病进展和预后[19]。P-选择素是选择素家族的重要成员,是内皮细胞与PLT的黏附因子,通常以可溶性形式释放入血。相关研究[20-21]显示,P-选择素可通过增强纤维蛋白沉积和产生促凝血微粒,参与血管壁炎症反应、内皮细胞黏附以及PLT中,进而导致PVT形成。本研究中D-D、P-选择素是肝硬化病人食管胃静脉曲张破裂出血后PVT的风险因素,且其水平随着PVT的发生而升高,由于血液样本容易获取,血液学指标容易检测且检测成本较低,因此,临床上对肝硬化食管胃静脉曲张破裂出血病人密切监测D-D、P-选择素水平,对其病情评估与PVT的诊断、预防及预后均有一定参考价值。研究[22]显示,与正常人和肝炎病人相比,肝癌和肝硬化病人中TG水平显著降低。在一项急性缺血性脑卒中病人无症状深静脉血栓形成(DVT)危险因素的研究[23]中发现DVT病人往往TG水平偏低。OKANO等[24]报道,TG水平与PLT活化能力呈负相关关系。然而以往的研究很少在PVT的形成中纳入脂类变量,而本研究TG水平是PVT形成的风险因素未能找到更多相关的证据。该因素与肝硬化病人PVT形成是否关联仍需要多中心大样本研究来进一步的证实。
基于多维度指标logistic回归分析结果构建预测模型用于预测疾病进展、并发症发生风险、预后是目前众多疾病研究的热点,但logistic回归分析的结果大多以公式化形式呈现,增加了使用医护人员的工作量。列线图是预测临床某一事件发生概率的可视化图形,通过logistic回归分析获得各项风险因素,以相应线段组成的图形呈现,根据各线段的赋值求分来预测事件发生风险。与复杂的公式相比,列线图模型更便于使用医护工作者的理解。为了保证模型的预测价值及其在临床上的通用性,本研究分别在研究队列与检验队列对模型的预测价值进行检验。结果提示,该模型具有较好的预测效能,能够准确地预测肝硬化病人食管胃静脉曲张破裂出血PVT的风险。因此,在临床诊治过程中应给予重点关注并加强巡视,监测相关指标的动态变化及其病情发展变化,及时调整治疗策略,以降低PVT发生风险。本研究创新点有以下几个方面:(1)基于多维度指标构建的风险列线图预测模型诊断效能较可靠。(2)肝硬化病人在中重度食管静脉曲张出血的治疗上,病人需要短期内多次住院行周期性的镜下治疗,而急性或严重的PVT形成可能会直接或间接的影响经内镜静脉曲张治疗的疗效。考虑门静脉进行定期的检测和频繁的影象学检查不仅浪费了医疗资源还加重了病人的经济负担。如果可以通过模型来预测高危人群才进行门静脉定期的检测与影像学检查,低危病人可以不做,可以降低临床诊疗成本,提高病人的依从性。(3)目前对于寻找肝硬化病人食管胃静脉曲张破裂出血后PVT形成的风险因素并建立一项基于多维度指标的列线图的研究报道较少,因此本研究的报道可能具有较大的学术参考价值。但本研究为单中心回顾性研究,结果的论证强度可能不及大样本、多中心、前瞻性等研究,今后可开展前瞻性、大样本、多中心的研究,以进一步验证。
综上所述,肝功能Child-Pugh分级、门静脉内径、PLT、D-D、P-选择素、TG是肝硬化病人食管胃静脉曲张破裂出血PVT的风险因素。基于上述指标建立的列线图预测模型具有良好的诊断效能,可为临床制定针对性治疗方案提供参考。
基于多维度指标构建肝硬化病人食管胃静脉曲张破裂出血后门静脉血栓风险列线图模型及验证
Construction and validation of a nomogram model for portal vein thrombosis risk after esophagogastric variceal rupture and bleeding in patients with cirrhosis based on multi-dimensional indicators
-
摘要:
目的基于多维度指标构建肝硬化病人食管胃静脉曲张破裂出血后门静脉血栓(PVT)风险的列线图模型,并进行验证。 方法选取肝硬化伴食管胃底静脉曲张破裂出血病人448例,按照3∶1的比例分为研究队列336例和检验队列112例,2队列再根据是否发生PVT分为血栓组和无血栓组,采用单因素分析和多因素回归分析筛选研究队列肝硬化病人食管胃静脉曲张破裂出血后发生PVT主要风险因素,采用RStudio软件中的rms程序包构建列线图并进行验证。 结果研究队列中77例(22.92%)发生PVT,其中出血后最快形成PVT者用时2周,49.35%(38/77)在1年内发生PVT,79.22%(61/77)在2年内合并PVT。检验队列中26例(23.21%)发生PVT,出血后最快形成PVT者用时12 d,50%(13/26)在1年内发生PVT,80.77%(21/26)在2年内合并PVT。单因素分析结果显示,研究队列PVT组与无PVT组肝功能Child-Pugh分级、门静脉内径、血小板计数、D-二聚体、P-选择素、三酰甘油差异均有统计学意义(P < 0.05~P < 0.01)。多因素logistic回归分析结果显示,肝功能Child-Pugh分级、门静脉内径、血小板计数、D-二聚体、P-选择素、三酰甘油均为肝硬化病人食管胃静脉曲张破裂出血后PVT的风险因素(P < 0.01)。ROC曲线分析结果显示,风险列线图预测模型在研究队列的曲线下面积(AUC)为0.953(95%CI:0.931~0.976),灵敏度为81.8%,特异度为94.2%;风险列线图预测模型在检验队列的AUC为0.944(95%CI:0.904~0.984),灵敏度为98.9%,特异度为81.4%。 结论肝功能Child-Pugh分级、门静脉内径、血小板计数、D-二聚体、P-选择素、三酰甘油均为肝硬化病人食管胃静脉曲张破裂出血PVT的风险因素。基于上述指标建立的列线图预测模型具有良好的诊断效能,可为临床制定针对性治疗方案提供参考。 Abstract:ObjectiveTo construct and validate a nomograph model for portal vein thrombosis(PVT) risk after esophagogastric variceal rupture and bleeding in patients with cirrhosis based on multi-dimensional indicators. MethodsA total of 448 patients with liver cirrhosis complicated with esophagogastric variceal rupture and bleeding were selected and divided into the study cohort(n=336) and test cohort(n=112) at the ratio of 3:1.The two cohorts were subdivided into the thrombus group and non-thrombus group according to whether PVT occurrence.The main risk factors of PVT in the study cohort after esophagogastric variceal rupture and bleeding in patients with cirrhosis were screened by univariate analysis and multivariate regression analysis, and a nomograph model was constructed using rms package in RStudio software and verified. ResultsIn the study cohort, 77 cases(22.92%) developed PVT, in which the fastest PVT formation after bleeding took two weeks, 49.35%(38/77) developed PVT within one year, and 79.22%(61/77) combined with PVT within two years.In the test cohort, 26 cases(23.21%) developed PVT, in which the fastest PVT formation after bleeding took 12 days, 50%(13/26) developed PVT within 1 year, and 80.77%(21/26)combined PVT within 2 years.Univariate analysis showed that there were significant differences in Child-Pugh liver function grade, portal vein diameter, platelet count, D-dimer, P-selectin and triacylglycerol between PVT group and non-PVT group(P < 0.05 to P < 0.01).Multivariate logistic regression analysis showed that Child-Pugh liver function grade, portal vein diameter, platelet count, D-dimer, P-selectin and triacylglycerol were the risk factors for PVT after esophagogastric variceal rupture and bleeding in patients with cirrhosis(P < 0.01).ROC curve analysis showed that the area under the curve(AUC) of the risk nomogram prediction model in the study cohort was 0.953(95%CI: 0.931-0.976), the sensitivity was 81.8%, and the specificity was 94.2%.ROC curve analysis showed that the AUC of the risk nomogram prediction model in the test cohort was 0.944(95%CI: 0.904-0.984), the sensitivity was 98.9%, and the specificity was 81.4%. ConclusionsChild-Pugh liver function grade, portal vein diameter, platelet count, D-dimer, P-selectin and triacylglycerol are the risk factors of PVT in patients with liver cirrhosis complicated with esophagogastric variceal rupture and bleeding.The nomogram prediction model based on the above indicators has good diagnostic performance, and can provide a reference for development of targeted treatment plans in clinic. -
表 1 研究队列与检验队列的临床资料比较(x±s)
因素 研究队列
(n=336)检验队列
(n=112)t P 男性 189(56.25) 65(58.04) 0.11△ >0.05 年龄/岁 45.88±10.05 46.94±9.52 0.99 >0.05 BMI/(kg/m2) 23.67±2.96 23.81±3.11 0.43 >0.05 吸烟史 66(19.64) 20(17.86) 0.48△ >0.05 高血压 98(29.17) 36(32.14) 0.36△ >0.05 糖尿病 51(15.17) 19(16.96) 0.20△ >0.05 冠心病 8(2.38) 6(5.36) 2.46△ >0.05 NSBB治疗史 108(32.14) 30(26.79) 1.13△ >0.05 外科手术 103(30.65) 28(25.00) 1.30△ >0.05 肝硬化类型 病毒性 198(58.93) 74(66.07) 酒精性 103(30.65) 28(25.00) 1.81△ >0.05 其他 35(10.42) 10(8.93) 肝功能Child-Pugh分级 A级
B+C级121(36.01)
215(63.99)30(26.78)
82(73.21)3.20△ >0.05 食管静脉曲张分级 轻度 36(10.71) 15(13.39) 中度 40(11.91) 18(16.07) 2.18△ >0.05 重度 260(77.38) 79(70.53) 腹水 169(50.30) 70(62.50) 0.86△ >0.05 消化道溃疡 103(30.65) 31(27.69) 0.36△ >0.05 内镜止血 161(47.92) 58(51.79) 0.50△ >0.05 门静脉内径/mm 15.52±3.73 15.23±3.36 0.72 >0.05 脾静脉内径/mm 9.06±2.85 9.15±2.92 0.29 >0.05 脾脏厚度/mm 44.56±7.58 43.96±7.62 0.73 >0.05 WBC/(×109/L) 7.23±2.38 7.35±2.46 0.46 >0.05 PLT/(×109/L) 95.72±20.13 96.46±18.94 0.34 >0.05 RBC/(×1012/L) 2.90±0.77 3.01±0.82 1.29 >0.05 Hb/(g/L) 92.16±11.60 92.87±11.92 0.56 >0.05 Alb/(g/L) 26.91±6.02 27.25±5.90 0.52 >0.05 FIB/(g/L) 2.79±0.81 2.68±0.76 1.26 >0.05 TBIL/(mol/L) 72.56±18.42 71.89±19.01 0.33 >0.05 PT/s 16.97±3.95 16.70±3.79 0.88 >0.05 APTT/s 38.46±8.46 39.02±8.20 0.61 >0.05 TT/s 12.82±3.95 13.52±4.03 1.62 >0.05 D-D/(μg/L) 2.87±0.43 2.78±0.40 1.59 >0.05 UN/(mmol/L) 7.11±2.29 7.01±2.23 0.40 >0.05 Cr/(μmol/L) 72.16±5.80 72.43±6.21 0.42 >0.05 P-选择素/(ng/mL) 70.17±8.09 69.89±7.92 0.27 >0.05 ALT/(U/L) 86.97±22.70 85.83±23.34 0.46 >0.05 AST/(U/L) 56.79±17.42 55.99±17.50 0.68 >0.05 TG/(mmol/L) 1.46±0.31 1.41±0.37 1.08 >0.05 TC/(mmol/L) 4.98±1.22 5.01±1.34 0.18 >0.05 INR 2.78±0.80 3.03±0.78 2.88 < 0.01 △示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 研究队列肝硬化病人食管胃静脉曲张破裂出血后发生PVT的单因素分析(x±s)
因素 PVT组
(n=77)无PVT组
(n=259)t P 男性 46(59.74) 143(55.21) 0.11△ >0.05 年龄/岁 46.47±10.13 47.22±9.86 0.58 >0.05 BMI/(kg/m2) 23.20±3.01 22.85±3.10 0.88 >0.05 吸烟史 18(23.38) 48(18.53) 2.29△ >0.05 高血压 29(37.66) 69(26.64) 3.49△ >0.05 糖尿病 17(22.08) 34(13.13) 3.69△ >0.05 冠心病 3(3.90) 4(1.54) 1.61△ >0.05 NSBB治疗史 30(38.96) 78(30.12) 2.13△ >0.05 外科手术 29(37.66) 74(28.57) 2.31△ >0.05 肝硬化类型 病毒性 49(63.63) 149(66.07) 酒精性 21(27.27) 82(31.66) 0.92△ >0.05 其他 7(9.09) 28(10.81) Child-Pugh分级 A级
B+C级19(24.68)
58(75.32)102(39.38)
157(60.62)5.57△ < 0.05 食管静脉曲张分级 轻度 8(10.39) 28(10.81) 中度 15(19.48) 25(9.65) 5.50△ >0.05 重度 54(70.13) 206(79.54) 腹水 40(50.30) 129(62.50) 0.11△ >0.05 消化道溃疡 27(30.65) 76(27.69) 0.91△ >0.05 内镜止血 42(47.92) 119(51.79) 1.76△ >0.05 门静脉内径/mm 18.16±4.50 13.04±3.22 11.11 < 0.01 脾静脉内径/mm 9.52±3.07 8.97±2.91 1.44 >0.05 脾脏厚度/mm 44.56±9.18 43.99±8.74 0.50 >0.05 WBC/(×109/L) 7.19±2.27 7.41±2.40 0.72 >0.05 PLT/(×109/L) 124.64±28.44 95.87±20.20 9.92 < 0.01 RBC/(×1012/L) 2.97±0.81 2.82±0.75 1.51 >0.05 Hb/(g/L) 92.71±13.52 92.08±12.89 0.37 >0.05 Alb/(g/L) 27.36±6.63 26.85±6.27 0.62 >0.05 FIB/(g/L) 2.80±0.83 2.72±0.79 0.77 >0.05 TBIL/(mol/L) 72.56±18.42 71.89±19.01 0.27 >0.05 PT/s 16.53±3.74 16.47±3.64 0.13 >0.05 APTT/s 38.96±8.33 40.11±8.51 1.05 >0.05 TT/s 12.82±3.95 13.52±4.03 1.34 >0.05 D-D/(μg/L) 2.93±0.43 2.26±0.39 12.92 < 0.01 UN/(mmol/L) 7.45±2.26 6.98±2.30 1.58 >0.05 Cr/(μmol/L) 72.55±5.78 73.46±6.33 1.13 >0.05 P-选择素/(ng/mL) 75.77±10.09 68.77±7.87 6.40 < 0.01 ALT/(U/L) 87.64±22.66 85.50±26.34 0.65 >0.05 AST/(U/L) 57.11±17.97 56.23±17.76 0.38 >0.05 TG/(mmol/L) 1.11±0.29 1.50±0.41 7.78 < 0.01 TC/(mmol/L) 5.14±1.33 5.05±1.13 0.59 >0.05 INR 2.89±0.81 3.08±0.76 1.90 >0.05 △示χ2值
下载: 导出CSV
表 3 研究队列肝硬化病人食管胃静脉曲张破裂出血后发生PVT的多因素logistic回归分析
变量 B SE Waldχ2 P OR 95%CI Child-Pugh分级 1.872 0.548 11.666 < 0.01 6.505 2.221~19.049 门静脉内径 0.394 0.707 32.099 < 0.01 1.484 1.294~1.700 PLT 0.038 0.010 14.791 < 0.01 1.039 1.019~1.059 D-D 0.999 0.258 14.937 < 0.01 2.716 1.636~4.507 P-选择素 0.078 0.025 9.342 < 0.01 1.081 1.028~1.136 TG -2.212 0.670 22.962 < 0.01 0.040 0.011~0.150
下载: 导出CSV
-
[1] 马沙沙, 高春明. PC、SD、PC/SD、FIB-4对肝硬化食管静脉曲张的诊断价值[J]. 蚌埠医学院学报, 2020, 45(10): 1344. doi: 10.13898/j.cnki.issn.1000-2200.2020.10.008 [2] 左怀文, 沙启梅, 孙姣, 等. 肝硬化食管静脉曲张患者门静脉血栓形成的危险因素分析[J]. 临床肝胆病杂志, 2021, 37(1): 63. doi: 10.3969/j.issn.1001-5256.2021.01.013 [3] LIM J, KIM H I, KIM E, et al. Variceal bleeding is aggravated by portal venous invasion of hepatocellular carcinoma: a matched nested case-control study[J]. BMC Cancer, 2021, 21(1): 11. doi: 10.1186/s12885-020-07708-1 [4] ZANETTO A, GARCIA-TSAO G. Some Answers and more questions about portal vein thrombosis in patients with decompensated cirrhosis[J]. Clin Gastroenterol Hepatol, 2020, 18(11): 2432. doi: 10.1016/j.cgh.2020.04.004 [5] 中华医学会肝病学分会. 肝硬化诊治指南[J]. 中华肝脏病杂志, 2019, 27(11): 846. doi: 10.3760/cma.j.issn.1007-3418.2019.11.008 [6] 中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会消化内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 中华内科杂志, 2016, 55(1): 57. doi: 10.3760/cma.j.issn.0578-1426.2016.01.015 [7] 黄鹤, 伦伟健, 梁晓燕, 等. 肝硬化食管胃静脉曲张破裂出血相关危险因素分析[J]. 四川医学, 2016, 37(3): 320. doi: 10.16252/j.cnki.issn1004-0501-2016.03.027 [8] 黄晓铨, 倪礼爰, 姜思雨, 等. 门静脉血栓影响内镜治疗预防乙型肝炎肝硬化食管胃静脉曲张破裂再出血的疗效[J]. 中华肝脏病杂志, 2020, 28(9): 747. doi: 10.3760/cma.j.cn501113-20200616-00326 [9] 肖春桃, 李贤秋, 周贤. 肝硬化门静脉血栓形成的危险因素分析[J]. 中国临床研究, 2021, 34(3): 341. doi: 10.13429/j.cnki.cjcr.2021.03.012 [10] NORTHUP PG, GARCIA-PAGAN JC, GARCIA-TSAO G, et al. Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients With Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases[J]. Hepatology, 2021, 73(1): 366. doi: 10.1002/hep.31646 [11] 杨静. 肝硬化患者食管胃静脉曲张破裂出血后门静脉血栓形成的危险因素分析[D]. 太原: 山西医科大学, 2021. [12] YUAN J, XU GM. Early and late stent thrombosis in patients with versus without diabetes mellitus following percutaneous coronary intervention with drug-eluting stents: a systematic review and Meta-analysis[J]. Am J Cardiovasc Drugs, 2018, 18(6): 483. doi: 10.1007/s40256-018-0295-y [13] BORJAS-ALMAGUER OD, CORTEZ-HERNANDEZ CA, GONZALEZ-MORENO EI, et al. Portal vein thrombosis in patients with cirrhosis: just a common finding or a predictor of poor outcome?[J]. Ann Hepatol, 2016, 15(6): 902. [14] AMITRANO L, GUARDASCIONE MA, BRANCACCIO V, et al. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis[J]. J Hepatol, 2004, 40(5): 736. doi: 10.1016/j.jhep.2004.01.001 [15] DONG G, HUANG XQ, ZHU YL, et al. Increased portal vein diameter is predictive of portal vein thrombosis development in patients with liver cirrhosis[J]. Ann Transl Medicine, 2021, 9(4): 289 doi: 10.21037/atm-20-4912 [16] ABD-ELSALAM S, HABBA E, ELKHALAWANY W, et al. Correlation of platelets count with endoscopic findings in a cohort of Egyptian patients with liver cirrhosis[J]. Medicine, 2016, 95(23): e3853. doi: 10.1097/MD.0000000000003853 [17] 韩晶, 毛锦娟, 吴时胜, 等. 肝硬化上消化道出血患者并发门静脉血栓形成的危险因素[J]. 中华实用诊断与治疗杂志, 2018, 32(6): 571. [18] 曾钗明, 郭太林, 陈建康, 等. 肝硬化联合门静脉血栓形成的危险因素及预后效果[J]. 血管与腔内血管外科杂志, 2019, 5(5): 407. doi: 10.19418/j.cnki.issn2096-0646.2019.05.004 [19] MALAGUARNERE M, LATTERI S, BERTINO G, et al. D-dimer plasmatic levels as a marker for diagnosis and prognosis of hepatocellular carcinoma patients with portal vein thrombosis[J]. Clin Exp Gastroenterol, 2018, 11(3): 373. [20] RIVA N, VELLA K, HICKEY K, et al. Biomarkers for the diagnosis of venous thromboembolism: D-dimer, thrombin generation, procoagulant phospholipid and soluble P-selectin[J]. J Clin Pathol, 2018, 71(11): 1015. doi: 10.1136/jclinpath-2018-205293 [21] 梅勇, 周志林, 杨旭辉, 等. P-选择素和D-二聚体对肝硬化门静脉血栓形成的早期预测作用研究[J]. 现代消化及介入诊疗, 2020, 25(9): 1231. doi: 10.3969/j.issn.1672-2159.2020.09.023 [22] JUN J, XING G, WANG H, et al. Association between metabolic abnormalities and HBV related hepatocelluar carcinoma in Chinese: a cross-sectional study[J]. Nutr J, 2011, 10(1): 49. [23] 李巍, 王莉莉, 李海燕, 等. 急性缺血性卒中患者无症状深静脉血栓形成危险因素分析[J]. 中国现代神经疾病杂志, 2021, 21(7): 592. doi: 10.3969/j.issn.1672-6731.2021.07.011 [24] OKANO K, SHITAMOTO K, ARAKI M, et al. Influencing factors in quantitative measurement using activated platelet levels and platelet-activating capacity for the assessment of thrombosis in pre-metabolic syndrome and type 2 diabetes mellitus[J]. Nurs Health Sci, 2018, 20(1): 69. doi: 10.1111/nhs.12389 -

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 2567
- HTML全文浏览量: 1097
- PDF下载量: 8
- 被引次数: 0
