

-
急性胰腺炎为临床较为常见的消化系统疾病之一[1],该病具有起病急、发展迅速、并发症较多、病死率较高等特点[2]。多项回顾性研究[3-5]结果表明,未发生感染的重症急性胰腺炎病人相比伴有继发感染的病人临床病死率有着明显差别,由此可以看出,感染对于重症急性胰腺炎病人的预后有着极大的影响。目前临床上常用的急性胰腺炎诊治指标有中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)、白细胞(WBC)、血淀粉酶(AMS)、尿淀粉酶(UAMY)、肝素结合蛋白(HBP)及降钙素原(PCT)等[4, 6-7],而上述指标对重症急性胰腺炎合并感染病情早期预测的研究较少,故本研究旨在探讨上述指标对重症急性胰腺炎病人合并感染早期预测的临床应用价值。
-
回顾性分析2020年7月至2021年1月我院急诊外科收治的重症急性胰腺炎病人64例,纳入标准:(1)所有病人均符合中国急性胰腺炎诊治指南(2019年,沈阳)的诊断标准[8];(2)发病至入院时间在24 h以内;(3)经腹部CT检查;(4)病例资料完整;(5)所有入组者均自愿参与该研究并签署了知情同意书。排除标准:(1)有自身免疫系统疾病;(2)合并心、肺、肾等系统疾病;(3)未完成整个诊疗过程。感染的评价标准为血培养、腹腔引流液、胰腺坏死组织或胰周液体等细菌培养阳性或CT检查提示胰腺、胰周或肺部等组织器官继发感染性病变。根据是否合并继发性感染,将64例病人分为感染组34例及非感染组30例。
-
于病人入院时采集静脉血及尿液,用血液细胞分析仪检测WBC、中性粒细胞、血小板和淋巴细胞计数,并计算NLR及PLR;采用全自动生化分析仪和对应试剂盒,检测AMS、UAMY水平; HBP采用Jet-iStar干式荧光免疫分析仪检测; PCT采用瑞恒科技RH-100免疫层析定量读数仪进行检测。
-
采用t检验和受试者工作特征曲线(ROC)分析。
-
感染组病人NLR、PLR、WBC、HBP、PCT水平均高于非感染组(P < 0.01),而2组AMS和UAMY水平差异无统计学意义(P>0.05)(见表 1)。
分组 n WBC/(×109/L) AMS/(U/L) UAMY/(U/L) NLR PLR HBP/(ng/mL) PCT/(ng/mL) 非感染组 30 10.93±2.82 425.86±519.09 1 389.60±2 229.78 6.59±2.99 115.17±55.02 50.72±19.26 1.56±0.29 感染组 34 13.67±2.25 519.06±406.17 2 153.67±3 008.96 10.78±4.39 178.53±51.27 82.87±20.58 2.08±0.70 t — 4.32 0.80 1.14 4.50* 4.77 6.43 3.96* P — < 0.01 >0.05 >0.05 < 0.01 < 0.01 < 0.01 < 0.01 *示t′值 表 1 2组病人血、尿相关指标的比较(x±s)
-
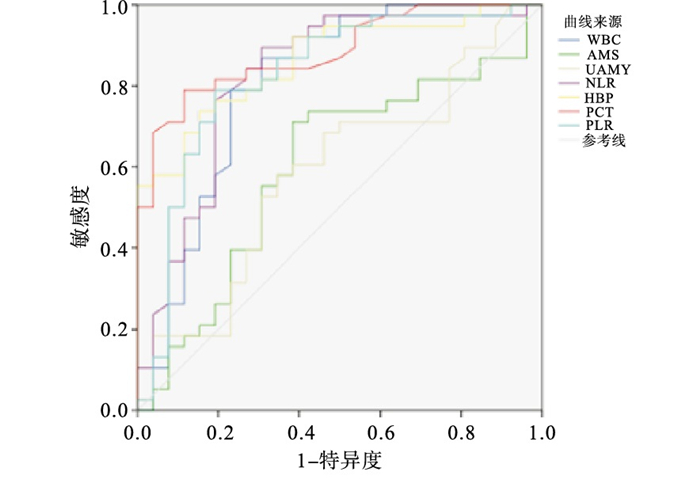
AMS和UAMY对诊断急性胰腺炎合并感染无统计学意义(P>0.05);WBC、NLR、PLR、HBP和PCT对重症急性胰腺炎病人合并感染的早期预测均有一定价值,而它们的敏感度、特异度及ROC曲线下面积(AUC)则有一定差异(P < 0.05),其中敏感度由大到小为:PLR>PCT>NLR>HBP>WBC,特异度由大到小为:PCT>NLR>PLR>HBP>WBC,AUC由大到小为:PCT>HBP>PLR>NLR>WBC(见表 2、图 1)。
指标 AUC P 截断值 敏感度/% 特异度/% WBC 0.803 < 0.05 11.78 78.90 76.90 AMS 0.599 >0.05 250.00 71.10 61.50 UAMY 0.587 >0.05 875.87 57.90 65.40 NLR 0.824 < 0.05 10.44 84.20 88.50 PLR 0.831 < 0.05 142.06 85.60 84.60 HBP 0.862 < 0.05 72.55 83.70 84.30 PCT 0.883 < 0.05 1.53 84.30 96.20 表 2 血、尿相关指标诊断急性胰腺炎合并感染的价值分析

图 1 血、尿相关指标诊断预测急性胰腺炎合并感染的ROC曲线
-
近年来,急性胰腺炎的发病率保持升高趋势,胆石症、高脂血症、暴饮暴食及酗酒等是引起急性胰腺炎的最常见诱因[9],合并感染则有较高的病死率。通过病人临床表现、影像学检查、血培养、引流液细菌培养等手段评估继发性感染耗时较多,风险较大,成本也较高,一旦延误诊断及治疗,可能会导致病人病情进一步恶化,死亡风险增大。急性胰腺炎易引发胰腺外器官的损伤,大量的胰酶和有害物质经血液释放可导致心、脑、肺、肝、肾等重要脏器损害,引发全身炎症反应综合征,甚至导致多器官功能障碍或衰竭,演变为重症急性胰腺炎。感染是急性胰腺炎常见的并发症,包括胰腺、胰周组织及肺部、泌尿系统等感染及菌血症等,对病人的预后产生非常严重的不良影响,其发生感染的概率大于50%,病死率较高[10-12]。因此对重症胰腺炎合并感染的情况做出早期预测,有利于感染的防治[13-14]。
本文主要探究了NLR、PLR、WBC、AMS、UAMY、HBP及PCT对重症急性胰腺炎病人合并感染病情的预测价值分析,以期探究特异度及敏感度均较好的感染标志物。NLR是反映高中性粒细胞数量(代表急性炎症反应)和低淋巴细胞数量(代表整体健康状况和生理压力均下降)的负面影响的参数。明显增高的NLR与良性和恶性临床状况的不良预后有关[15-17]。目前有报道认为NLR单个参数也能够预测急性胰腺炎的感染并发症[18]。本研究表明,NLR的监测对重症急性胰腺炎合并感染的早期预测具有重要的临床价值,AUC为0.824,敏感度为84.20%,特异度为88.50%。既往研究[19]表明PLR为癌症和炎症性疾病的预后标志物,可用于预测急性胆源型胰腺炎的严重程度,而该指标对重症急性胰腺炎合并感染的预测作用尚无明确结论;本研究表明,监测PLR对重症急性胰腺炎合并感染的早期预测AUC为0.831,敏感度为85.60%,特异度为84.60%。WBC作为传统炎症指标,在临床上广泛运用于对疾病炎症及感染程度的判断,本研究表明,WBC的监测对重症急性胰腺炎合并感染的早期预测亦具有一定的临床价值,但其AUC、敏感度及特异度较其他指标均较低,临床预测价值相对较小。HBP是一种丝氨酸蛋白酶,具有嗜蓝颗粒,由中性粒细胞分泌囊泡释放。研究[20]表明,HBP参与了多种炎症条件和感染的发展。在炎症过程的早期阶段,嗜酸性颗粒和分泌囊泡分泌HBP, HBP通过激活各种类型的细胞,包括单核细胞,导致血管渗漏和水肿形成。有研究[21]表明,在多形核细胞渗出后,HBP也会分泌,并促进炎症反应。本研究表明,HBP的监测对重症急性胰腺炎合并感染的早期预测AUC为0.862,敏感度为83.70%,特异度为84.30%。相关研究[22-23]表明,PCT是用于感染的诊断预测和指导抗生素治疗有效的、特异性的标志物,同时它是预测术后感染并发症的有用指标。本研究表明,PCT的监测对重症急性胰腺炎合并感染的早期预测具有明显的临床价值,AUC为0.883,敏感度为84.30%,特异度为96.20%。AMS、UAMY本身即是急性胰腺炎的诊断标准之一,淀粉酶数值与胰腺炎病情严重程度并不相关,但对于重症急性胰腺炎合并感染是否有预测价值,目前尚不明了。本研究表明,AMS及UAMY对于重症急性胰腺炎合并感染的早期预测无明显临床价值。
不同指标对重症急性胰腺炎病人合并感染的早期预测价值分析
Predictive analysis of different biochemical indicators in the assessment of severe acute pancreatitis complicated with infection
-
摘要:
目的探讨中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)、白细胞(WBC)、血淀粉酶(AMS)、尿淀粉酶(UAMY)、肝素结合蛋白(HBP)及降钙素原(PCT)对重症急性胰腺炎病人合并感染病情预测的临床应用价值,以及特异度及敏感度均较好的感染早期预测指标。 方法回顾性分析重症急性胰腺炎病人64例的临床资料,根据是否合并感染,将64例病人分为感染组34例及非感染组30例。于入院时采集静脉血检测NLR、PLR、WBC、AMS及PCT,采集病人尿液检测UAMY,并对检测数据进行对比分析。 结果非感染组和感染组中WBC、NLR、PLR、HBP、PCT水平差异均有统计学意义(P < 0.01);2组AMS、UAMY水平差异均无统计学意义(P>0.05)。AMS和UAMY对诊断急性胰腺炎合并感染无统计学意义(P>0.05);WBC、NLR、PLR、HBP和PCT指标在采用敏感度、特异度及ROC曲线下面积(AUC)诊断均有统计学意义(P < 0.05),其中敏感度由大到小为:PLR>PCT>NLR>HBP>WBC,特异度由大到小为:PCT>NLR>PLR>HBP>WBC,AUC由大到小为:PCT>HBP>PLR>NLR>WBC。 结论NLR、WBC、PLR、HBP及PCT的监测对重症急性胰腺炎合并感染的早期预测具有一定的临床价值,有助于对病情的判断及对后续治疗的指导。 -
关键词:
- 胰腺炎 /
- 感染 /
- 中性粒细胞与淋巴细胞比值 /
- 血小板与淋巴细胞比值 /
- 肝素结合蛋白 /
- 降钙素原
Abstract:ObjectiveTo explore the clinical application value of neutrophil-lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), white blood cell (WBC), blood amylase (AMS), urinary amylase (UAMY), heparin binding protein(HBP) and procalcitonin(PCT) in the evaluation of infection and severity of disease in patients with severe acute pancreatitis, and explore the infection markers with good specificity and sensitivity. MethodsThe clinical data of 64 patients with severe acute pancreatitis were retrospectively analyzed. According to the incidence of co-infection, the 64 patients were divided into the infection group (34 cases) and the non-infection group (30 cases). On admission, venous blood was collected to detect NLR, PLR, WBC, AMS, HBP and PCT. Urine samples were collected to detect UAMY, and the data were analyzed. ResultsThere were significant differences in the levels of WBC, NLR, PLR, HBP and PCT between the non-infection group and the infection group (P < 0.01). There was no significant difference in AMS and UAMY levels between the two groups (P>0.05). AMS and UAMY had no statistical significance in the diagnosis of acute pancreatitis complicated with infection (P>0.05). WBC, NLR, PLR, HBP and PCT had the statistical significance in the diagnosis of severe acute pancreatitis with sensitivity(PLR>PCT>NLR>HBP>WBC), specificity(PCT>NLR>PLR>HBP>WBC) and area under ROC curve (AUC)(PCT>HBP>PLR>NLR>WBC) (P < 0.05). ConclusionsThe monitoring of NLR, PLR, WBC, HBP and PCT has the important clinical value for the early prediction of severe acute pancreatitis complicated with infection, which is helpful to judge the condition and guide the follow-up treatment. -
表 1 2组病人血、尿相关指标的比较(x±s)
分组 n WBC/(×109/L) AMS/(U/L) UAMY/(U/L) NLR PLR HBP/(ng/mL) PCT/(ng/mL) 非感染组 30 10.93±2.82 425.86±519.09 1 389.60±2 229.78 6.59±2.99 115.17±55.02 50.72±19.26 1.56±0.29 感染组 34 13.67±2.25 519.06±406.17 2 153.67±3 008.96 10.78±4.39 178.53±51.27 82.87±20.58 2.08±0.70 t — 4.32 0.80 1.14 4.50* 4.77 6.43 3.96* P — < 0.01 >0.05 >0.05 < 0.01 < 0.01 < 0.01 < 0.01 *示t′值  下载: 导出CSV
下载: 导出CSV
表 2 血、尿相关指标诊断急性胰腺炎合并感染的价值分析
指标 AUC P 截断值 敏感度/% 特异度/% WBC 0.803 < 0.05 11.78 78.90 76.90 AMS 0.599 >0.05 250.00 71.10 61.50 UAMY 0.587 >0.05 875.87 57.90 65.40 NLR 0.824 < 0.05 10.44 84.20 88.50 PLR 0.831 < 0.05 142.06 85.60 84.60 HBP 0.862 < 0.05 72.55 83.70 84.30 PCT 0.883 < 0.05 1.53 84.30 96.20
下载: 导出CSV
-
[1] BANG JY, WILCOX CM, ARNOLETTI JP, et al. Superiority of endoscopic interventions over minimally invasive surgery for infected necrotizing pancreatitis: meta-analysis of randomized trials[J]. Dig Endosc, 2020, 32(3): 298. doi: 10.1111/den.13470 [2] 张映媛, 黄华, 路明亮, 等. 不同评分系统对判断急性胰腺炎病情及预后的比较研究[J]. 胃肠病学和肝病学杂志, 2018, 27(1): 25. doi: 10.3969/j.issn.1006-5709.2018.01.005 [3] ARVANITAKIS M, DUMONCEAU JM, ALBERT J, et al. Endoscopic management of acute necrotizing pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) evidence-based multidisciplinary guidelines[J]. Endoscopy, 2018, 50(5): 524. doi: 10.1055/a-0588-5365 [4] SCHEPERS NJ, BAKKER OJ, BESSELINK MG, et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis[J]. Gut, 2019, 68(6): 1044. doi: 10.1136/gutjnl-2017-314657 [5] ROBERTS SE, MORRISON-REES S, JOHN A, et al. The incidence and aetiology of acute pancreatitis across Europe[J]. Pancreatology, 2017, 17(2): 155. doi: 10.1016/j.pan.2017.01.005 [6] BUXBAUM JL, QUEZADA M, DA B, et al. Early aggressive hydration hastens clinical improvement in mild acute pancreatitis[J]. Am J Gastroenterol, 2017, 112(5): 797. doi: 10.1038/ajg.2017.40 [7] 程峰, 邱兆磊, 王振杰, 等. 超声引导下经皮经肝胆囊穿刺引流术在急性胆源性胰腺炎治疗中的应用[J]. 蚌埠医学院学报, 2020, 45(9): 1166. [8] 中华医学会消化病学分会胰腺疾病学组, 《中华胰腺病杂志》编委会, 《中华消化杂志》编委会. 中国急性胰腺炎诊治指南(2019年, 沈阳)[J]. 临床肝胆病杂志, 2019, 35(12): 2706. [9] ANNA W, BRIT L, ALEX K, et al. Acute pancreatitis: updates for emergency clinicians[J]. J Emerg Med, 2018, 55(6): 769. doi: 10.1016/j.jemermed.2018.08.009 [10] 李曼, 邢小康, 郭丰. 6种评分系统和4个实验室检查指标对重症急性胰腺炎预后的评估作用[J]. 中华消化杂志, 2018, 38(10): 673. doi: 10.3760/cma.j.issn.0254-1432.2018.10.005 [11] 覃敏珍, 姚敦卫, 唐国都. 血清C反应蛋白/白蛋白比值对重症急性胰腺炎的预测价值[J]. 广西医学, 2019, 18(20): 2576. [12] 肖辉. 急性胆源性胰腺炎患者的早期腺泡损伤与炎症因子反应的临床研究[J]. 临床消化病杂志, 2019, 31(2): 104. doi: 10.3870/lcxh.j.issn.1005-541X.2019.02.09 [13] 郑传明, 王振杰, 纪忠, 等. 彩超引导下经皮穿刺置管引流术在重症急性胰腺炎合并胰周积液患者中的应用价值[J]. 蚌埠医学院学报, 2016, 41(10) : 1275. [14] IQBAL U, ANWAR H, SCRIBANI M. RINGER's lactate versus normal saline in acute pancreatitis: a systematic review and meta-analysis[J]. J Dig Dis, 2018, 19(6): 335. doi: 10.1111/1751-2980.12606 [15] JABAUDON M, BELHADJ-TAHAR N, RIMMELÉ T, et al. Thoracic epidural analgesia and mortality in acute pancreatitis: a multicenter propensity analysis[J]. Crit Care Med, 2018, 46(3): e198. doi: 10.1097/CCM.0000000000002874 [16] LI W, LIU J, ZHAO S, et al. Safety and efficacy of total parenteral nutrition versus total enteral nutrition for patients with severe acute pancreatitis: a meta-analysis[J]. J Int Med Res, 2018, 46(9): 3948. doi: 10.1177/0300060518782070 [17] MOWBRAY NG, BEN-ISMAEIL B, HAMMODA M, et al. The microbiology of infected pancreatic necrosis[J]. Hepatobiliary Pancreat Dis Int, 2018, 17(5): 456. doi: 10.1016/j.hbpd.2018.08.007 [18] VEGE SS, DIMAGNO MJ, FORSMARK CE, et al. Initial medical treatment of acute pancreatitis: American gastroenterological association institute technical review[J]. Gastroenterology, 2018, 154(4): 1103. [19] CHO SK, JUNG S, LEE KJ, et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio can predict the severity of gallstone pancreatitis[J]. BMC Gastroenterol, 2018, 18(1): 18. [20] 王宁, 刘利胜. 降钙素原与中性粒细胞和淋巴细胞计数比值对肿瘤患者细菌感染预测价值[J]. 中华肿瘤防治杂志, 2018, 25(8): 595. [21] BANG JY, ARNOLETTI JY, HOLT JP, et al. An endoscopic transluminal approach, compared to minimally invasive surgery, reduces complications and costs for patients with necrotizing pancreatitis[J]. Gastroenterology, 2019, 156(4): 1027. [22] FISHER J, RUSSELL JA, BENTZER P, et al. Heparin-Binding Protein (HBP): acausative marker and potential target for heparin treatment of human sepsis-induced acute kidney injury[J]. Shock, 2017, 48(3): 313. [23] TVERRING J, NIELSEN N, DANKIEWICZ J, et al. Repeated measures of Heparin-binding protein (HBP) and procalcitonin during septic shock: biomarker kinetics and association with cardiovascular organ dysfunc-tion[J]. Intensive Care Med Exp, 2020, 8(1): 51. -

 点击查看大图
点击查看大图
图(1)表(2)
计量
- 文章访问数: 1909
- HTML全文浏览量: 931
- PDF下载量: 24
- 被引次数: 0
