

-
敌草快(diquat,DQ)是一种非选择性、触杀性除草剂,与百草枯(paraquat,PQ) 化学结构相似,均为联吡啶化学分类。由于PQ的人体毒性较大,且无特效解毒药[1],导致的临床病死率较高,已逐渐被毒性较低的DQ取代。尽管DQ毒性较PQ低,但中毒后若不能及时有效干预,仍可造成病人出现多器官功能衰竭甚至死亡。
有研究[2]指出,不同类型的农药尽管在毒性表现上存在着差异,但毒性机制却存在相似之处。其中DQ的致病机制与PQ类似,均为促进线粒体氧化还原循环过程,产生的大量超氧阴离子自由基通过氧化应激和脂质过氧化导致机体细胞和组织损伤[3]。对DQ中毒病人血液、尿液毒物浓度的测定以及中毒剂量的评估可用于指导临床分析中毒病人的预后。而目前毒物浓度的测定多基于高效液相色谱法,因其检测方法较为复杂,临床上很难实现普及。此外,实际临床工作中发现对包括中毒剂量在内的病史信息进行及时准确的采集也存在一定困难。因此寻找可替代的临床或实验室指标对DQ中毒病人的诊疗和预后具有十分重要的意义。对PQ中毒的相关研究发现,外周血白细胞(WBC)增多是氧化应激反应的一部分,急性PQ中毒病人炎症反应早期即可表现出WBC增多、中性粒细胞增多和淋巴细胞减少,且非幸存者的WBC和中性粒细胞计数明显高于幸存者[4]。也有研究[5]指出全身炎症反应综合征(systemic inflammatory response syndrome,SIRS)评分可用于评估DQ中毒病人的预后[5]。而作为临床上最常见的可反映机体应激和炎症反应的WBC、中性粒细胞计数等炎症细胞参数,目前尚无确切证据表明其与DQ中毒病人的生存状况存在显著关联。
本研究通过评估WBC、中性粒细胞计数等参数与DQ中毒病人出院生存状况的关联,为临床早期识别DQ中毒危重症病人以及改善病人的预后提供依据。现作报道。
-
2019-2021年我院急诊科共接诊DQ中毒病人41例。纳入标准:急性DQ中毒病人,诊断标准参见《急性敌草快中毒诊断与治疗专家共识》[6]。排除标准:有其他毒物混合者;非口服中毒途径者;慢性疾病终末期病人;合并有急性或慢性炎症、严重感染或血液病的病人。
-
41例病人中,30例治愈出院者纳入存活组,院内死亡4例和放弃治疗出院后随访期间(3个月)死亡者7例纳入死亡组。
-
全血样本使用EDTA-K2抗凝管采集2 mL静脉血,血清样本使用分离胶促凝管,血浆样本使用肝素抗凝管采集4 mL静脉血,血清或血浆样本3 000 r/min离心5 min后分离血清或血浆,所有样本均要求采集后立即检测。
-
采用希森美康公司的XN 9000型血液分析仪检测全血WBC、中性粒细胞计数等血细胞参数。采用贝克曼库尔特公司的AU 5800型生化分析仪检测肝功能、肾功能等生化指标。采用罗氏公司的Cobas E601型电化学发光仪检测肌钙蛋白T(cTNT)和脑利钠肽前体(NT-proBNP)。
-
收集41例DQ病人的一般资料和住院期间的相关实验室指标,包括性别、年龄、体质量指数(BMI)、中毒剂量(指DQ摄入的毫升数,目前市场上DQ溶液的常见浓度为20%,即100 mL溶液实际等同于20 g溶质)、中毒开始至洗胃时间(指病人从摄入毒物开始到洗胃结束中间所经历的时间差),是否接受血液灌流、连续性肾脏替代治疗(CRRT)、机械通气等治疗。
关于洗胃、血液灌流、CRRT、机械通气等治疗手段的开展,本研究采纳《急性敌草快中毒诊断与治疗专家共识》为依据,该共识指出对DQ中毒病人应实现尽早洗胃,常规给予血液灌流,出现急性肾损伤时给予CRRT[7],此外仅当出现低氧血症时方考虑使用机械通气治疗。作为糖皮质激素的甲泼尼龙和免疫抑制剂环磷酰胺,虽有文献报道其单一或联合使用用于治疗急性DQ中毒,但尚无明确证据表明其治疗有效性。
中毒后24 h监测肝功能、肾功能、心脏指标、C反应蛋白以及血细胞参数,其中肝功能包括丙氨酸氨基转移酶(ALT)、天冬氨酸氨基转移酶(AST)、总胆红素(TBIL)、白蛋白(ALB)、球蛋白(GLB)、ALB/GLB比值(A/G),肾功能包括尿素氮(UREA)、肌酐(CREA)、心脏指标包括肌钙蛋白T(cTNT)、脑利钠肽前体(NT-proBNP),血细胞参数包括WBC、中性粒细胞计数、红细胞计数(RBC)、血红蛋白(HGB)、红细胞压积(HCT)、红细胞分布宽度(RDW)、血小板计数(PLT)、平均血小板体积(MPV),中毒后72 h监测C反应蛋白和血细胞参数。
-
采用t检验、χ2检验、logistic回归分析。对有独立预测能力的指标采用受试者操作特征(ROC) 曲线及曲线下面积(AUC) 描述,分析最佳截断值及指标的预测效能。
-
41例DQ中毒病人中,男20例(48.78%),女21例(51.22%),年龄13~55岁,平均(31.00±10.64)岁,BMI (21.30±3.71)kg/m2。中毒剂量(115.17±179.11)mL,中毒开始至洗胃时间(1.95±2.38)h,洗胃量(18 280.00±16 989.02)mL,住院时间(13.37±11.65)d。接受洗胃者37例(90.24%), 接受血液灌流者35例(85.37%), 接受CRRT者21例(51.22%),接受机械通气者6例(14.63%)。关于甲泼尼龙和环磷酰胺,41例中接受单一甲泼尼龙治疗者15例,接受甲泼尼龙联合环磷酰胺治疗者12例,未接受以上任一药物治疗者14例。
-
结果显示,死亡组的年龄、BMI及接受机械通气、接受CRRT的病人比例显著高于存活组,住院时间显著低于存活组(P < 0.01),接受血液灌流、洗胃的病人比例,中毒开始至洗胃时间以及洗胃量等因素在2组间的差异均无统计学意义(P>0.05)(见表 1)。DQ中毒病人接受甲泼尼龙、环磷酰胺单一或联合两者治疗情况比较,发现2种药物的不同治疗方案与DQ中毒病人的存活情况无显著关联(见表 2)。中毒后24 h的WBC、中性粒细胞计数、RBC、NT-proBNP、ALT、A/G表现为死亡组病人显著高于存活组(P < 0.05),而TBIL死亡组病人显著低于存活组(P < 0.01)(见表 3)。
分组 n 男 年龄/岁 BMI/(kg/m2) 中毒剂量/mL 住院时间/d 死亡组 11 7 38.27±9.71 24.42±4.37 170.91±144.88 5.82±4.14 存活组 30 13 28.33±9.80 20.38±3.05 94.73±188.14 16.13±12.32 t — 1.33# 2.88* 3.34 1.21 4.01* P — > 0.05 < 0.01 < 0.01 > 0.05 < 0.01 分组 n 接受血液灌流 接受CRRT 接受机械通气 接受洗胃 中毒开始至洗胃时间/h 洗胃量/mL 死亡组 11 9 9 5 11 2.45±2.28 17 428.57±12 434.59 存活组 30 26 12 1 26 1.74±2.43 18 611.11±18 774.63 t — 0.34# 5.63# 8.31# 0.46# 0.83* 0.19* P — > 0.05 < 0.05 < 0.01 > 0.05 > 0.05 > 0.05 *示t′值;#示χ2值;中毒剂量按20%DQ溶液100 mL等同于20 g的标准 表 1 死亡组和存活组一般资料比较(x±s)
分组 n 未使用甲泼尼龙或环磷酰胺 单一使用甲泼尼龙 联合使用甲泼尼龙和环磷酰胺 χ2 P 死亡组 11 2(14.29) 6(40.00) 3(25.00) 存活组 30 12(85.71) 9(60.00) 9(75.00) 2.46 > 0.05 合计 41 14(34.15) 15(36.59) 12(29.27) 表 2 死亡组和存活组甲泼尼龙、环磷酰胺的使用情况比较[n; 百分率(%)]
分组 n cTnT/(ng/L) NT-proBNP/(pg/mL) ALT/(U/L) AST/(U/L) TBIL/(mol/L) A/G 尿素氮/(mmol/L) 肌酐/(mol/L) CRP/(mg/L) 死亡组 11 228.38±466.07 5 397.40±6149.28 490.91±575.92 561.19±778.37 7.95±4.35 19.15±2.45 7.32±3.58 150.23±103.45 36.75±37.47 存活组 30 7.28±8.15 82.05±64.05 53.03±88.26 59.26±70.83 16.49±7.13 13.08±13.07 5.53±2.68 103.70±74.23 21.98±22.35 t — 1.57* 2.87* 2.51* 2.14* 3.71 2.43* 1.73 1.60 1.23 P — > 0.05 < 0.05 < 0.05 > 0.05 < 0.01 < 0.05 > 0.05 > 0.05 > 0.05 分组 n WBC/(×109/L) 中性粒细胞计数/(×109/L) RBC/(×1012/L) HGB/(g/L) RDW PLT/(×109/L) MPV/fL 死亡组 11 24.08±10.31 22.47±9.80 4.92±0.62 148.33±18.04 13.16±1.21 193.11±74.20 10.42±0.81 存活组 30 13.68±4.88 11.76±4.84 4.44±0.51 136.52±18.35 12.62±0.78 194.78±68.22 10.19±1.01 t — 4.40 3.47 2.52 1.83 1.68 0.07 0.68 P — < 0.01 < 0.01 < 0.05 > 0.05 > 0.05 > 0.05 > 0.05 *示t′值 表 3 死亡组和存活组中毒后24 h的实验室指标比较(x±s)
-
logistic回归分析结果显示,一般资料中年龄、BMI、是否接受机械通气、是否接受CRRT、住院时间,以及中毒后24 h的主要检验指标中WBC、中性粒细胞计数、RBC的回归意义显著(P < 0.05)(见表 4)。考虑到年龄、性别因素可能对相关研究指标回归分析的影响,在加入年龄、性别作为调整变量后再次行logistic回归,结果显示仅住院时间、是否进行机械通气、中毒后24 h的WBC和中性粒细胞计数回归意义显著(P < 0.05)(见表 5)。
变量 B SE Wald χ2 P OR 95% CI 年龄/岁 -0.097 0.040 6.02 < 0.05 0.907 0.840~0.981 BMI -0.297 0.151 3.89 < 0.05 0.743 0.553~0.998 中毒剂量/mL -0.002 0.002 1.24 > 0.05 0.998 0.994~1.002 是否接受CRRT -1.910 0.866 4.86 < 0.05 0.148 0.027~0.809 是否接受机械通气 -3.185 1.184 7.24 < 0.01 0.041 0.004~0.421 住院时间/d 0.289 0.109 6.98 < 0.01 1.335 1.077~1.653 中毒后24 h的WBC/(×109/L) -0.176 0.072 5.95 < 0.05 0.839 0.728~0.966 中毒后24 h的中性粒细胞计数/(×109/L) -0.203 0.084 5.81 < 0.05 0.816 0.692~0.963 中毒后24 h的RBC/(×1012/L) -1.538 0.782 3.87 < 0.05 0.215 0.046~0.995 表 4 DQ中毒病人的出院存活情况与临床和检验指标的logistic回归分析
变量 B SE Wald χ2 P OR 95% CI BMI -0.218 0.202 1.17 > 0.05 0.804 0.542~1.194 中毒剂量/mL 0.001 0.002 0.05 > 0.05 1.000 0.995~1.004 是否接受CRRT -1.313 0.952 1.90 > 0.05 0.269 0.042~1.739 是否接受机械通气 -2.940 1.316 5.00 < 0.05 0.053 0.004~0.696 住院时间/d 0.413 0.171 5.82 < 0.05 1.511 1.080~2.112 中毒后24 h的WBC/(×109/L) -0.171 0.082 4.50 < 0.05 0.840 0.715~0.987 中毒后24 h的中性粒细胞计数/(×109/L) -0.193 0.092 4.43 < 0.05 0.824 0.688~0.987 中毒后24 h的RBC/(×1012/L) -2.014 1.091 3.40 > 0.05 0.133 0.016~1.134 表 5 DQ中毒病人的出院存活情况与临床和检验指标的logistic回归分析(加入调整变量)
-
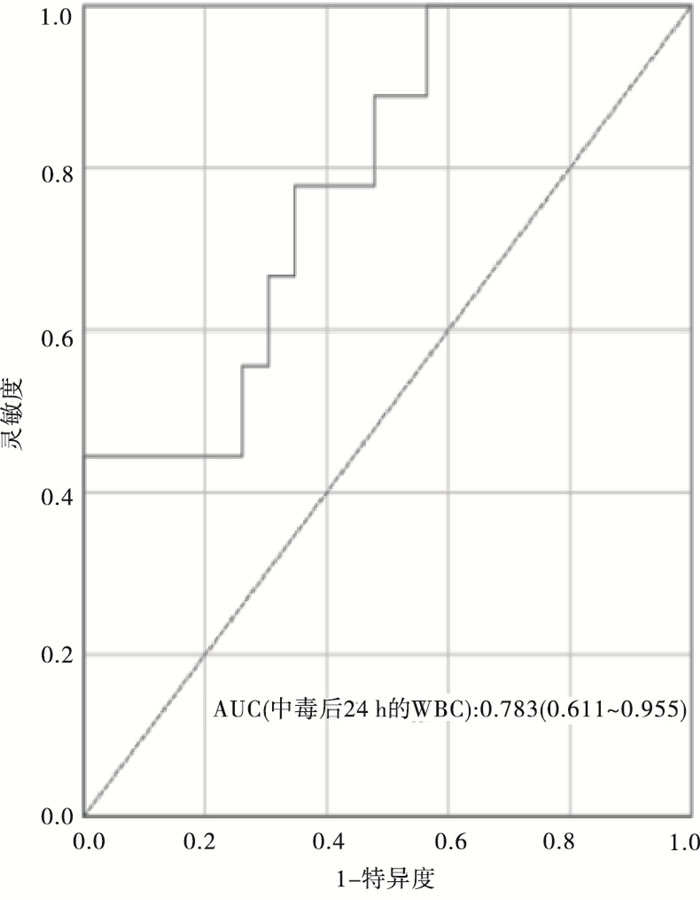
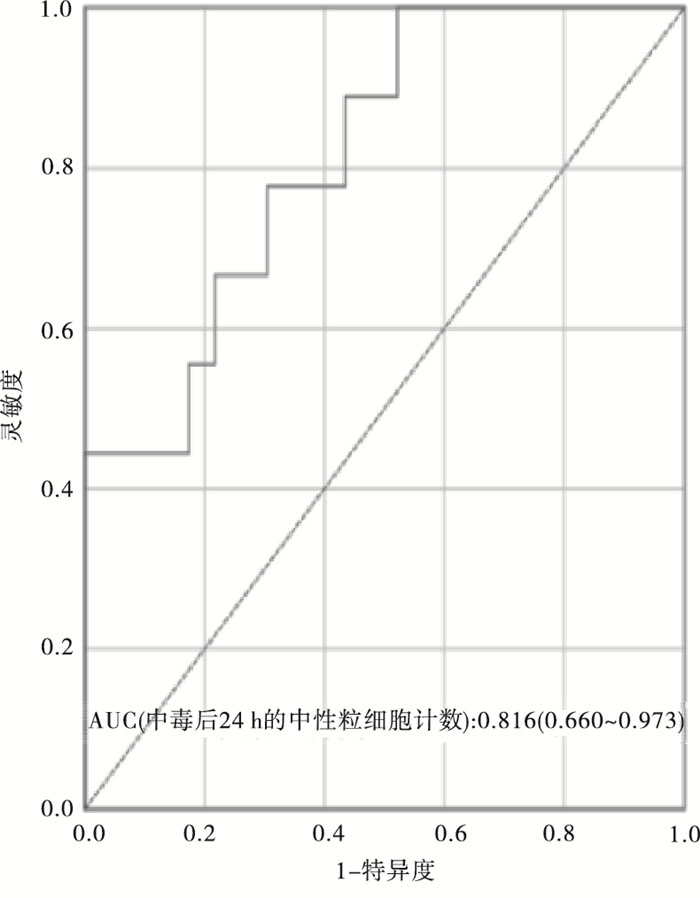
结果显示,当中毒后24 h的WBC和中性粒细胞计数分别以29.345×109/L、11.765×109/L作为截断值,其预测DQ中毒病人出院生存状况可获得最大AUC(AUC: 0.783±0.088, 95%CI: 0.611~0.955, P < 0.05和AUC: 0.816±0.080, 95%CI: 0.660~0.973, P < 0.01),且两者获得的AUC显著大于中毒剂量(AUC: 0.771±0.082, 95%CI: 0.611~0.931, P < 0.01)(见图 1~3和表 6)。

图 1 DQ中毒病人中毒剂量与出院生存状况的ROC曲线分析

图 2 DQ中毒病人中毒后24 h的WBC与出院生存状况的ROC曲线分析

图 3 DQ中毒病人中毒后24h的中性粒细胞计数与出院生存状况的ROC曲线分析
特征 n AUC 灵敏度 特异度 约登指数 最佳阈值 中毒后24 h的WBC/(×109/L) 32 0.783 0.444 1.000 0.444 29.345 中毒后24 h的中性粒细胞计数/(×109/L) 32 0.816 1.000 0.478 0.478 11.765 中毒剂量/mL 41 0.771 0.727 0.800 0.527 90.000 注:约登指数=灵敏度+特异性-1 表 6 中毒后24 h的WBC、中性粒细胞计数、中毒剂量与DQ病人出院生存状况的ROC曲线分析表
-
结果显示,存活组病人中毒后72 h的WBC、中性粒细胞计数水平较中毒后24 h显著减低(P < 0.05),而死亡组病人中毒后72 h的两指标平均水平虽也表现出低于24 h, 但差异无统计学意义(P>0.05)(见表 7)。
出院生存状况 n WBC/(×109/L) t P 中性粒细胞计数/(×109/L) t P 中毒后24 h 中毒后72 h 中毒后24~72 h差值 中毒后24 h 中毒后72 h 中毒后24~72 h差值 存活组 30 13.68±4.99 11.28±4.38 2.40±5.40 2.13 < 0.05 11.76±4.95 9.15±4.07 2.62±5.10 2.46 < 0.05 死亡组 11 22.53±12.17 19.17±7.51 3.37±5.86 1.41 > 0.05 21.17±11.87 17.62±7.99 3.55±5.61 1.55 > 0.05 表 7 不同生存状况组病人WBC、中性粒细胞计数随时间变化的比较分析(x±s)
-
目前关于DQ中毒病人死亡的相关危险因素的研究结果多表明中毒剂量和毒物浓度测定可作为预测病人生存结局的有效手段。血液、尿液中毒物的浓度测定虽然可以精准计算实际中毒剂量,但因其检测方法复杂,较难在临床上普及,此外实际临床工作中准确地对中毒剂量的病史采集存在一定难度。基于氧化应激反应的中毒机制,目前有研究[5]在对DQ中毒病人进行SIRS评分时发现,生存组与死亡组病人的SIRS评分有显著差异,提示炎症反应较重的病人预后较差,该研究结果表明炎症反应与DQ病人的预后存在一定关联。WBC是机体防御系统的主要组成部分,同时也是反映机体应激及炎性反应的重要指标,作为目前临床上最常见的具有炎症指征意义的参数,已被广泛应用于各类疾病的诊断和预后评估。
本研究首先对41例DQ中毒病人的一般资料和主要实验室指标按出院生存状况进行分组比较,结果显示死亡组病人其中毒发生后24 h的WBC以及中性粒细胞计数水平均显著高于存活组病人。此外,年龄、BMI、中毒剂量、中毒后24 h的RBC、接受CRRT、机械通气的病人比例及NT-proBNP、ALT、TBIL、A/G等指标也表现出明显的组间差异。logistic回归分析结果显示,除中毒剂量外,中毒后24 h的WBC、中性粒细胞计数等参数均表现出与DQ中毒病人出院生存状况存在显著关联。而在加入年龄、性别作为调整变量后,仅中毒后24 h的WBC、中性粒细胞计数、是否接受机械通气以及住院时间仍与出院生存状况关联显著。以上结果表明中毒后24 h的WBC和中性粒细胞计数可用于预测DQ中毒病人的出院生存状况。ROC曲线分析结果显示,中毒后24 h的WBC和中性粒细胞计数判断DQ中毒病人出院生存状况的最佳截断值分别为29.345×109/L和11.765×109/L,即当中毒后24 h的WBC>29.345×109/L、中毒后24 h的中性粒细胞计数>11.765×109/L时,DQ中毒病人的死亡风险显著增加。此外基于ROC分析AUC的比较,中毒后24 h的WBC和中性粒细胞计数对DQ中毒病人的预后价值更优于使用传统的中毒剂量的手段。对存活组和死亡组病人的WBC和中性粒细胞计数比较其中毒后24 h、72 h的时间动态变化,结果显示,存活组病人中毒后72 h的WBC、中性粒细胞计数水平较中毒后24 h显著减低,而死亡组病人中毒后72 h的两指标平均水平虽也表现出低于24 h, 但前后差异并不显著。
已有研究[8]指出DQ中毒病人入院后的初次WBC计数显著升高可提示病人的不良预后,本研究进一步证实了中毒后24 h的WBC水平对DQ中毒病人出院生存状况的预测价值。有研究[9]结果表明,PQ中毒的氧化应激机制可导致机体内的系统炎症反应,高水平的中性粒细胞和低水平的淋巴细胞常常预示着PQ中毒病人的不良结局, 但目前鲜见文献报道关于WBC分类计数与DQ中毒病人预后的关系,基于此本研究探讨了中毒后24 h的中性粒细胞计数对DQ中毒病人出院生存状况的预测价值。此外,本研究还对病人中毒后24 h、72 h的WBC以及中性粒细胞计数进行了比较分析,发现存活组和死亡组DQ中毒病人其WBC、中性粒细胞计数存在随时间差异性的动态变化表现,这凸显了DQ中毒病人WBC以及中性粒细胞计数水平的动态监测对指导预后的重要价值。现有对DQ中毒的研究结果多指出中毒剂量可作为预测病人死亡的独立危险因素[10],本研究仅发现中毒剂量在存活组和死亡组的分组比较中存在显著差异,进一步的logistic回归分析并未表明其与病人的出院生存状况有显著关联。此外对中毒剂量的ROC曲线分析结果显示其AUC值低于中毒后24 h的WBC和中性粒细胞计数。究其原因,可能为病人中毒后毒物实际摄入量受诸多因素的影响,如是否呕吐以及呕吐量、是否洗胃及洗胃量、血液灌流等,这可能导致了回归分析中的中毒剂量无法单独预测病人死亡的情况。此外,本研究在分组比较以及回归分析时还发现,是否接受机械通气与DQ中毒病人的出院生存状况存在一定关联,这可能与接受机械通气的DQ病人往往因存在肺损伤[11]以及吸入性肺炎有关从而指向了不良预后,由于本研究主要关注炎症反应机制下WBC的预后价值,而并未对DQ中毒病人治疗措施的独立预测能力进一步分析。关于甲泼尼龙和环磷酰胺,已有相关文献报道其单一或联合使用用于治疗急性PQ和缺乏特异性毒检依据的DQ中毒病人,但针对性的研究结果并未明确表明其可显著降低中毒病人的死亡率,以及是否会增加病人的感染风险[12]。本研究在对以上2种药物的使用和DQ中毒病人的存活情况进行分析中发现两者之间并无显著关联,表明甲泼尼龙和环磷酰胺的使用并未显著改善DQ中毒病人的生存状况。
本研究为单中心回顾性研究,符合研究标准的样本量较少,部分研究对象资料缺失,也造成了有效样本量较少,因此相关结论的应用需进一步多中心扩大样本人群加以证实。
综上,本研究提示DQ中毒病人中毒后24 h的WBC和中性粒细胞计数水平可以作为预测其出院生存状况的有效因子,WBC、中性粒细胞计数水平的动态监测对判断预后也具有重要意义。
白细胞和中性粒细胞计数对敌草快中毒病人出院生存状况的预测价值
Predictive value of white blood cell and neutrophil count on the survival status of patients with diquat poisoning after discharge
-
摘要:
目的探讨敌草快(DQ)中毒病人临床特点及预后的影响因素,评估白细胞(WBC)、中性粒细胞计数对DQ中毒病人出院生存状况的预测价值。 方法收集DQ中毒病人41例,按出院生存状况分为存活组30例和死亡组11例,分析2组病人的临床和实验室指标,采用logistic回归分析病人预后的影响因素,利用ROC曲线评价中毒后24 h的WBC以及中性粒细胞计数水平对DQ中毒病人出院生存状况的预测价值。此外,分析2组病人中毒后24 h、72 h的WBC和中性粒细胞计数水平,以评估WBC、中性粒细胞计数的动态变化与DQ中毒病人出院生存状况可能存在的关联。 结果死亡组病人的年龄、体质量指数(BMI)、中毒剂量以及接受机械通气的比例显著高于存活组,而接受连续性肾脏替代治疗(CRRT)的比例、住院时间均显著低于存活组(P < 0.01)。死亡组中毒后24 h的WBC、中性粒细胞计数显著高于存活组(P < 0.05)。logistic回归分析显示,除中毒剂量外,分组比较存在显著差异的各变量回归意义明显(P < 0.05)。在加入性别、年龄作为调整变量后再行回归分析,结果显示仅住院时间、是否进行机械通气、中毒后24 h的WBC和中性粒细胞计数有统计学意义(P < 0.05)。ROC曲线分析显示,当中毒后24 h的中性粒细胞计数、WBC分别以11.765×109/L和29.345×109/L作为cut-off值,可获得最大曲线下面积(AUC:0.816±0.080,95%CI:0.660~0.973,P < 0.01和AUC:0.783±0.088,95%CI:0.611~0.955,P < 0.05)。存活组病人中毒后72 h的WBC、中性粒细胞计数均显著低于中毒后24 h(P < 0.05),而死亡组病人中毒后72 h的WBC、中性粒细胞计数虽然平均水平也低于中毒后24 h,但差异无统计学意义(P>0.05)。 结论DQ中毒病人中毒后24 h的WBC和中性粒细胞计数水平可以作为预测其出院生存状况的有效因子,对WBC、中性粒细胞计数水平的动态监测有助于判定DQ中毒病人的不良预后。 Abstract:ObjectiveTo explore the clinical characteristics and prognostic factors of diquat (DQ) poisoning patients, and evaluate the predictive value of white blood cell (WBC) and neutrophil count on the survival status of DQ poisoning patients after discharge. MethodsAccording to the survival status after discharge, 41 patients with DQ poisoning were divided into survival group (n=30) and death group (n=11).The clinical and laboratory index of the two groups were analyzed.The influencing factors of patients' prognosis were analyzed by logistic regression.ROC curve was used to evaluate the predictive value of WBC and neutrophil count 24 h after poisoning on the survival status of patients with DQ poisoning.In addition, the levels of WBC and neutrophil count at 24 h and 72 h after poisoning in the two groups were analyzed to evaluate the possible correlation between the dynamic changes of WBC and neutrophil count and the discharge survival status of DQ poisoning patients. ResultsThe age, body mass index, toxic dose and the proportion of mechanical ventilation in the death group were significantly higher than those in the survival group, while the proportion of CRRT and the length of hospital stay were significantly lower than those in the survival group (P < 0.01).The levels of WBC and neutrophil count 24 h after poisoning in the death group were significantly higher than the survival group (P < 0.01).Logistic regression analysis showed that except for the poisoning dose, the value of variables with significant differences in group comparison was obvious (P < 0.05).After adding gender and age as adjustment variables, the results of logistic regression analysis showed that only the length of hospital stay, mechanical ventilation or not, WBC and neutrophil count 24 h after poisoning were significant (P < 0.05).The ROC curve analysis showed that when 11.765×109/L and 29.345×109/L were used as cutoff values of the neutrophil count and WBC 24 h after poisoning respectively, the maximum area under the curve can be obtained (AUC: 0.816±0.080, 95%CI: 0.660-0.973, P < 0.01 and AUC: 0.783±0.088, 95%CI: 0.611-0.955, P < 0.05).The levels of WBC and neutrophil counts in the survival group at 72 hours after poisoning were significantly lower than those at 24 h after poisoning (P < 0.05).By contrast, the average levels of WBC and neutrophil count in the death group at 72 hours after poisoning were also lower than that at 24 h after poisoning, but the difference was not significant. ConclusionsWBC and neutrophil count in patients with DQ poisoning 24 hours after poisoning can be used as effective factors to predict their survival after discharge, and the dynamic monitoring of WBC and neutrophil count is helpful to determine the adverse prognosis of patients with DQ poisoning. -
Key words:
- diquat poisoning /
- white blood cell count /
- neutrophil count /
- survival status /
- prediction
-
表 1 死亡组和存活组一般资料比较(x±s)
分组 n 男 年龄/岁 BMI/(kg/m2) 中毒剂量/mL 住院时间/d 死亡组 11 7 38.27±9.71 24.42±4.37 170.91±144.88 5.82±4.14 存活组 30 13 28.33±9.80 20.38±3.05 94.73±188.14 16.13±12.32 t — 1.33# 2.88* 3.34 1.21 4.01* P — > 0.05 < 0.01 < 0.01 > 0.05 < 0.01 分组 n 接受血液灌流 接受CRRT 接受机械通气 接受洗胃 中毒开始至洗胃时间/h 洗胃量/mL 死亡组 11 9 9 5 11 2.45±2.28 17 428.57±12 434.59 存活组 30 26 12 1 26 1.74±2.43 18 611.11±18 774.63 t — 0.34# 5.63# 8.31# 0.46# 0.83* 0.19* P — > 0.05 < 0.05 < 0.01 > 0.05 > 0.05 > 0.05 *示t′值;#示χ2值;中毒剂量按20%DQ溶液100 mL等同于20 g的标准  下载: 导出CSV
下载: 导出CSV
表 2 死亡组和存活组甲泼尼龙、环磷酰胺的使用情况比较[n; 百分率(%)]
分组 n 未使用甲泼尼龙或环磷酰胺 单一使用甲泼尼龙 联合使用甲泼尼龙和环磷酰胺 χ2 P 死亡组 11 2(14.29) 6(40.00) 3(25.00) 存活组 30 12(85.71) 9(60.00) 9(75.00) 2.46 > 0.05 合计 41 14(34.15) 15(36.59) 12(29.27)
下载: 导出CSV
表 3 死亡组和存活组中毒后24 h的实验室指标比较(x±s)
分组 n cTnT/(ng/L) NT-proBNP/(pg/mL) ALT/(U/L) AST/(U/L) TBIL/(mol/L) A/G 尿素氮/(mmol/L) 肌酐/(mol/L) CRP/(mg/L) 死亡组 11 228.38±466.07 5 397.40±6149.28 490.91±575.92 561.19±778.37 7.95±4.35 19.15±2.45 7.32±3.58 150.23±103.45 36.75±37.47 存活组 30 7.28±8.15 82.05±64.05 53.03±88.26 59.26±70.83 16.49±7.13 13.08±13.07 5.53±2.68 103.70±74.23 21.98±22.35 t — 1.57* 2.87* 2.51* 2.14* 3.71 2.43* 1.73 1.60 1.23 P — > 0.05 < 0.05 < 0.05 > 0.05 < 0.01 < 0.05 > 0.05 > 0.05 > 0.05 分组 n WBC/(×109/L) 中性粒细胞计数/(×109/L) RBC/(×1012/L) HGB/(g/L) RDW PLT/(×109/L) MPV/fL 死亡组 11 24.08±10.31 22.47±9.80 4.92±0.62 148.33±18.04 13.16±1.21 193.11±74.20 10.42±0.81 存活组 30 13.68±4.88 11.76±4.84 4.44±0.51 136.52±18.35 12.62±0.78 194.78±68.22 10.19±1.01 t — 4.40 3.47 2.52 1.83 1.68 0.07 0.68 P — < 0.01 < 0.01 < 0.05 > 0.05 > 0.05 > 0.05 > 0.05 *示t′值
下载: 导出CSV
表 4 DQ中毒病人的出院存活情况与临床和检验指标的logistic回归分析
变量 B SE Wald χ2 P OR 95% CI 年龄/岁 -0.097 0.040 6.02 < 0.05 0.907 0.840~0.981 BMI -0.297 0.151 3.89 < 0.05 0.743 0.553~0.998 中毒剂量/mL -0.002 0.002 1.24 > 0.05 0.998 0.994~1.002 是否接受CRRT -1.910 0.866 4.86 < 0.05 0.148 0.027~0.809 是否接受机械通气 -3.185 1.184 7.24 < 0.01 0.041 0.004~0.421 住院时间/d 0.289 0.109 6.98 < 0.01 1.335 1.077~1.653 中毒后24 h的WBC/(×109/L) -0.176 0.072 5.95 < 0.05 0.839 0.728~0.966 中毒后24 h的中性粒细胞计数/(×109/L) -0.203 0.084 5.81 < 0.05 0.816 0.692~0.963 中毒后24 h的RBC/(×1012/L) -1.538 0.782 3.87 < 0.05 0.215 0.046~0.995
下载: 导出CSV
表 5 DQ中毒病人的出院存活情况与临床和检验指标的logistic回归分析(加入调整变量)
变量 B SE Wald χ2 P OR 95% CI BMI -0.218 0.202 1.17 > 0.05 0.804 0.542~1.194 中毒剂量/mL 0.001 0.002 0.05 > 0.05 1.000 0.995~1.004 是否接受CRRT -1.313 0.952 1.90 > 0.05 0.269 0.042~1.739 是否接受机械通气 -2.940 1.316 5.00 < 0.05 0.053 0.004~0.696 住院时间/d 0.413 0.171 5.82 < 0.05 1.511 1.080~2.112 中毒后24 h的WBC/(×109/L) -0.171 0.082 4.50 < 0.05 0.840 0.715~0.987 中毒后24 h的中性粒细胞计数/(×109/L) -0.193 0.092 4.43 < 0.05 0.824 0.688~0.987 中毒后24 h的RBC/(×1012/L) -2.014 1.091 3.40 > 0.05 0.133 0.016~1.134
下载: 导出CSV
表 6 中毒后24 h的WBC、中性粒细胞计数、中毒剂量与DQ病人出院生存状况的ROC曲线分析表
特征 n AUC 灵敏度 特异度 约登指数 最佳阈值 中毒后24 h的WBC/(×109/L) 32 0.783 0.444 1.000 0.444 29.345 中毒后24 h的中性粒细胞计数/(×109/L) 32 0.816 1.000 0.478 0.478 11.765 中毒剂量/mL 41 0.771 0.727 0.800 0.527 90.000 注:约登指数=灵敏度+特异性-1
下载: 导出CSV
表 7 不同生存状况组病人WBC、中性粒细胞计数随时间变化的比较分析(x±s)
出院生存状况 n WBC/(×109/L) t P 中性粒细胞计数/(×109/L) t P 中毒后24 h 中毒后72 h 中毒后24~72 h差值 中毒后24 h 中毒后72 h 中毒后24~72 h差值 存活组 30 13.68±4.99 11.28±4.38 2.40±5.40 2.13 < 0.05 11.76±4.95 9.15±4.07 2.62±5.10 2.46 < 0.05 死亡组 11 22.53±12.17 19.17±7.51 3.37±5.86 1.41 > 0.05 21.17±11.87 17.62±7.99 3.55±5.61 1.55 > 0.05
下载: 导出CSV
-
[1] 王冉, 吴晓飞, 陆国玉, 等. 急性百草枯中毒病人预后的影响因素分析[J]. 蚌埠医学院学报, 2018, 43(2): 164. [2] SULE RO, CONDON L, GOMES AV. A common feature of pesticides: oxidative stress-the role of oxidative stress in pesticide-induced toxicity[J]. Oxid Med Cell Longev, 2022, 2022: 5563759. [3] MAGALHÃES N, CARVALHO F, DINIS-OLIVEIRA RJ. Human and experimental toxicology of diquat poisoning: toxicokinetics, mechanisms of toxicity, clinical features, and treatment[J]. Hum Exp Toxicol, 2018, 37(11): 1131. doi: 10.1177/0960327118765330 [4] ZHOU DC, ZHANG H, LUO ZM, et al. Prognostic value of hematological parameters in patients with paraquat poisoning[J]. Sci Rep, 2016, 6: 36235. doi: 10.1038/srep36235 [5] 王韫文, 赵敏. 71例急性敌草快中毒患者死亡危险因素分析[J/OL]. 中国医科大学学报, 2022, 51(3): 203. [6] 急性敌草快中毒诊断与治疗专家共识组. 急性敌草快中毒诊断与治疗专家共识[J]. 中华急诊医学杂志, 2020, 29(10): 1282. doi: 10.3760/cma.j.issn.1671-0282.2020.10.002 [7] 胡德亮, 张劲松, 陈旭锋, 等. 连续性肾替代治疗在体外膜氧合病人中的应用[J]. 蚌埠医学院学报, 2022, 47(10): 1360. [8] 梁晓丽, 虎晓岷, 龚阳, 等. 2016-2018年间40例敌草快中毒患者的死亡危险因素分析[J]. 临床急诊杂志, 2019, 20(5): 366. [9] WANG J, JIANG X, LU G, et al. Identify the early predictor of mortality in patients with acute paraquat poisoning[J]. Biomed Res Int, 2020, 2020: 8894180. [10] 王鸾, 王洋, 赵敏. 急性敌草快中毒患者死亡危险因素分析[J]. 中国实用内科杂志, 2020, 40(2): 158. [11] 刘雪萍, 蒋文中, 杨志前, 等. 口服敌草快中毒主要靶器官的新认识[J]. 岭南急诊医学杂志, 2021, 26(2): 180. [12] LI LR, CHAUDHARY B, YOU C, et al. Glucocorticoid with cyclophosphamide for oral paraquat poisoning[J]. Cochrane Database Syst Rev, 2021, 6(6): CD008084. -

 点击查看大图
点击查看大图

图(3)表(7)
计量
- 文章访问数: 1644
- HTML全文浏览量: 766
- PDF下载量: 7
- 被引次数: 0
