



-
在临床麻醉中,镇静安定药、麻醉性镇痛药和静脉全麻药联合用于全麻诱导是目前最常见诱导用药组合,采用多种药物联合的目的在于充分发挥每个药的药理特性,从而减少麻醉药的用量,减少或降低麻醉药的不良反应。小剂量苯二氮卓类药、丙泊酚(Pro)与小剂量麻醉性镇痛药一起使用时,不仅可以彼此增强催眠作用,而且可以利用麻醉性镇痛药能缓解或阻断伤害性刺激反应的特性,达到满意的诱导、插管和切皮等麻醉的要求。药物联合应用所涉及的问题很多,比如咪达唑仑(Mid)、芬太尼(Fen)、Pro之间是否存在相互作用?其性质是什么?它们的最佳配伍剂量是多少?等等。对于多比例多剂量水平的组方优选,目前常用的方法有正交设计法、配方均匀设计法、直接寻优法等,这些方法要求的组数多,实验误差大。权重配方法是研究利用优化(或超级)拉丁方设计和均匀设计原理,并根据复方药物量效关系特点,规范实验设计建立的新的数据分析法[1],为药物配方实验提供了一种科学、高效和简便的手段。本研究运用权重配方法,探讨Mid、Fen和Pro联合诱导时,各药在维持血流动力学稳定上作用的大小,以及各药之间相互作用的性质。
HTML
-
60例择期行腹腔镜手术的病人,年龄18~60岁,ASA分级Ⅰ~Ⅱ级。
-
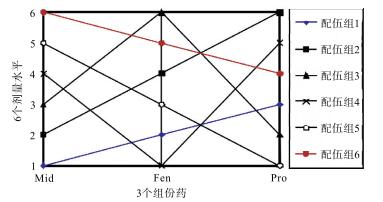
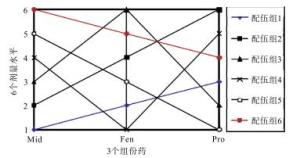
根据临床上的使用情况,将Mid、Pro、Fen的足量和弱效量分别确定为:Mid 0.02~0.06 mg/kg,Fen 2~6 μg/kg,Pro 0.5~1.5 mg/kg。用0.8的等比例,在足量至低效量范围内,将各组份药分为大小不同的6个剂量,构建出权重配方设计表(见图 1),60例病人随机分配至6个配伍组(见表 1)。
配伍组 Mid Fen Pro 组1 0.02 0.0025 0.8 组2 0.025 0.004 1.5 组3 0.03 0.006 0.6 组4 0.04 0.002 1.2 组5 0.05 0.003 0.5 组6 0.06 0.005 1.0 Dmax 0.06 0.006 1.5 Dmin 0.02 0.002 0.5 -
所有病人术前30 min肌内注射东莨菪碱0.3 mg。入室后GE-B40i型监护仪监测心率、无创动脉血压和脉搏血氧饱和度。右肘正中静脉穿刺置管滴注乳酸林格液。待监护仪上各项数据稳定3 min后,依次注入Mid(15 s)、Fen(15 s)、Pro(30 s)和罗库溴铵0.6 mg/kg。Pro注入后3 min采用双盲法行气管插管。
-
记录诱导前、Pro注入后1 min(T1)、2 min(T2)、插管即刻(T3)、插管后1(T4)、3(T5)、5(T6)、7 min(T7)的平均动脉压(MAP)和心率(HR)数值。
-
采用方差分析。
1.1. 病例选择
1.2. 分组设计
1.3. 麻醉过程
1.4. 数据采集
1.5. 统计学方法
-
诱导后各时点的MAP与术前基础值的差值,配伍组6的血压波动在插管前后(T3)低于配伍组1(P<0.05)(见表 2)。将各时点的血压波动值换算成效应值输入DAS ver1.0,结果显示3药在组方中的重要程度为:Pro>Mid>Fen(P<0.05)。其理论优化组方为Mid 0.06 mg/kg,Fen 0.005 mg/kg,Pro 1.5 mg/kg。理论优化比例为Mid:Fen:Pro=1.00:0.083 33:25。Pro与Mid之间为协同作用(P < 0.05),Pro与Fen之间为相加作用(P<0.05)(见表 3)。
分组 T1 T2 T3 T4 T5 T6 T7 组1 16.1±10.9 16.9±13.0 33.7±16.3 16.5±14.0 11.4±8.6 17.7±8.0 21.0±13.5 组2 19.4±10.0 23.6±10.8 20.4±14.9 17.3±9.3 10.1±8.2 12.7±8.9 13.6±7.0 组3 17.8±13.0 25.1±14.9 23.3±13.6 18.0±12.2 15.3±10.1 18.7±10.6 19.2±12.1 组4 24.1±17.0 19.1±16.0 27.1±16.5 21.6±15.9 12.3±8.9 13.9±8.9 17.8±8.5 组5 10.6±7.8 28.5±13.2 24.5±19.0 11.6±13.7 11.6±8.6 13.2±6.7 21.5±19.6 组6 16.7±7.4 22.7±13.4 7.6±3.9* 11.3±6.8 15.7±14.0 19.8±17.0 16.1±7.5 F 1.48 0.93 3.43 1.03 0.52 0.86 0.61 P >0.05 >0.05 < 0.01 >0.05 >0.05 >0.05 >0.05 MS组内 132.068 186.242 220.187 153.012 98.730 111.445 148.387 q检验:同时间点与组1比较*P<0.05 组分 标化剂量 b(di) b(didj) P 优化剂量 优化剂量注释和相互作用定性结果 Mid d1 0.458 — >0.05 0.060 为Mid DEmax Fen d2 0.288 — >0.05 5.000 为Fen DEmax Pro d3 0.537 — < 0.05 1.500 为Pro Dmax 交互项 d3d1 — 0.524 < 0.05 0.060 为Mid剂量(Dmax), 两组分呈协同性 交互项 d3d2 — 0.353 >0.05 5.000 为Fen剂量, 两组分间呈相加性 -
插管后各组的HR变化差异无统计学意义(P>0.05)(见表 4)。将各时点的HR变化值输入DAS ver1.0,结果显示3药在组方中的重要程度为Fen>Pro>Mid(P<0.05)。其理论优化组方为Mid 0.06mg/kg,Fen 0.005 mg/kg,Pro 1.25 mg/kg。理论优化比例为Mid:Fen:Pro=1.00:0.083 33:20.83,Fen与Pro和Mid之间均为协同作用(P<0.05和P<0.01)(见表 5)。
分组 T1 T2 T3 T4 T5 T6 T7 组1 8.8±6.8 8.2±10.2 24.5±19.1 23.2±10.8 17.1±10.4 14.4±13.8 13.7±15.0 组2 6.9±5.2 10.1±7.8 13.5±10.8 15.0±14.6 11.8±15.6 11.8±14.2 11.5±9.2 组3 7.4±3.7 6.3±2.3 13.3±7.2 13.3±17.9 18.5±13.0 13.7±12.0 13.5±10.7 组4 10.4±7.9 17.2±10.6 13.8±21.1 24.7±18.6 17.0±11.3 16.5±10.0 18.3±13.6 组5 7.2±8.6 8.1±9.8 15.7±9.6 17.6±12.4 14.4±13.6 8.6±6.8 8.8±7.7 组6 18.2±13.9 16.3±11.9 8.2±3.8 13.0±8.1 7.6±9.5 8.3±11.4 9.4±10.8 F 2.67 2.44 1.40 1.27 1.09 0.80 0.92 P >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 MS组内 69.425 86.697 180.850 202.141 153.903 135.380 130.837 组分 标化剂量 b(di) b(didj) P 优化剂量 优化剂量注释和相互作用定性结果 Mid d1 0.256 — >0.0.5 0.060 为Mid DEmax Fen d2 0.390 — >0.05 5.000 为Fen DEmax Pro d3 0.277 — >0.05 1.000 为Pro DEmax 交互项 d2d1 — 0.511 < 0.05 0.060 为Mid剂量(Dmax), 两组分呈协同性 交互项 d2d3 — 0.717 < 0.01 1.500 为Pro剂量(Dmax), 两组分呈协同性
2.1. Mid、Fen和Pro联用对血压的影响
2.2. Mid、Fen和Pro联用对HR的影响
-
权重配方法主要有以下特点:(1)是一种高效的方法,组方优选一般仅需6组,就可初步得出结果。如条件许可,尽量另设2~3组进行确定性试验。(2)在限定的多药物多剂量水平范围内,寻找最佳配伍,且结果符合专业要求。(3)能做药物相互作用的定性分析。(4)可确定各药组方中的重要程度。(5)由于确定性试验存在,使得本法的结果可靠[2]。
MAP是反映病人术中血流动力学变化的指标,也是判断病人术中麻醉深度的一个重要指标。理想麻醉诱导药应该是既能维持病人血流动力学稳定,又能保证足够的麻醉深度。本实验中,Mid、Fen、Pro的权重指数分别为0.458、0.288和0.537,说明这3种药对病人的血流动力学均有影响,但Pro在保持病人麻醉诱导期间血流动力学稳定上起主要作用,Pro在组方中的理想剂量应为1.0~1.5 mg/kg,与符定家等[3]的研究相似。
麻醉诱导时影响HR的因素很多,心脏交感神经和迷走神经的紧张性、插管的伤害性刺激、血流动力学的变化等均可对HR产生影响。方育等[4]认为Fen可以有效减弱置喉镜与插管刺激引起血流动力学改变,使诱导过程中病人的血流动力学更稳定。另有学者[5-6]认为有效控制该刺激引起的血液动力学变化,Fen的剂量应>4 μg/kg,就稳定病人诱导和插管期间HR而言,Fen在本诱导组方中起主要作用,组方中理想的Fen的剂量应不低于4 μg/kg。
在药物的相互作用上,Fen和Pro在保持诱导期心率稳定上起协同作用,而在对血压的影响上两者仅为相加作用。WICZLING等[7]认为0.001 mg/kg Fen与Pro合用时对血压和HR的影响呈协同作用,和本研究的结果有所不同。本研究中,以血压为参照指标时,Pro在组方中为主药;而在以HR为参照指标时,Fen为主药。对于Fen和Pro对血压和HR的影响上所表现出的不同的相互作用,和两药在体内不同的分布时间有关,在以与Fen相关性较好的HR作为参照指标观察时,由于Pro分布时间短,在体内很快达到血-效应点平衡浓度,所以二者表现出协同作用。而在以与Pro相关性较好的血压作为参照指标观察时,由于在诱导期Fen的血-效应点浓度未达到平衡,所以未表现出协同作用。
Mid在本组方中的作用相对较弱,但它在预防插管期间血流动力学变化上,和Pro、Fen均有协同作用,值得关注。我们推荐的Mid用量为0.06 mg/kg。本文采用Mid、Fen、Pro序贯诱导的方法,是否发挥Mid的药理特性,有待进一步研究。
综上,在本麻醉诱导组方中Pro和Fen在维持血流动力学稳定上起主要作用,Mid、Pro和Fen之间有协同作用,理想的诱导剂量为Mid 0.06 mg/kg,Fen 0.005 mg/kg,Pro 1.25 mg/kg。
 DownLoad:
DownLoad: