




-
近年来,肺癌已成为全球发病率及死亡率最高的恶性肿瘤,严重影响人类的健康[1-3],外科手术治疗依然是肺癌治疗的最重要手段,微创胸腔镜肺切除手术的发展也极大地推动了肺外科治疗技术进步。三维重建技术目前在肺段切除的术前规划和术中导航中应用越来越多[4-5],我们在肺段切除手术中应用经验积累的基础上,进一步在中央型肺癌和淋巴结明显肿大的肺叶根治性切除手术中应用三维重建技术,取得较好的临床效果,现作报道。
HTML
-
回顾性分析2018年11月至2019年12月,蚌埠医学院第一附属医院胸外科收治的非小细胞肺癌行胸腔镜肺叶切除和肺结节行肺段切除术50例病人的临床资料。其中男18例,女32例;年龄(56.60±10.16)岁;体检发现肺部病变37例,痰中带血4例,胸闷4例,刺激性干咳5例;术前均行胸部薄层CT扫描,肺功能、心电图、肺癌相关及常规检查等均无手术禁忌证。胸腔镜肺叶根治性切除术25例,包括右上肺癌8例,右中肺癌2例,右下肺癌9例,左上肺癌3例,左下肺癌3例;胸腔镜肺结节行肺段切除术25例,切除肺部病灶57个。肺癌肺叶切除术病人均满足根治性手术适应证;肺段切除手术符合以下要求:(1)病变直径≤2 cm且满足以下条件之一:磨玻璃成分≥50%、快速病理提示原位癌或微浸润癌、倍增时间≥400 d;(2)单肺或双肺多发结节、需保留更多肺功能等妥协性手术;(3)因位置、大小等原因无法楔形切除的良性病变等。此技术的开展通过蚌埠医学院第一附属医院伦理审查及院高新技术支持。
-
收集胸部薄层CT扫描数据,数据最佳要求:(1)64排CT机以上设备,采集层厚<1 mm的胸部薄层CT;(2)深吸气,保持屏气状态下扫描;(3)增强CT需控制对比剂药量及时间,采用团注试验法获得“时间-密度曲线”,通过分析后设置对比剂的注射剂量和延迟扫描时间,肺动脉与肺静脉的CT差值在150~350 Hu之间,肺动脉CT值高于周围胸腔组织100 Hu以上;(4)避免和头、颈及腹部联合扫描,避免反复多次扫描,去除扫描区域异物。将CT图像信息以DICOM格式保存应用。应用沈阳东软医疗系统有限公司授权的DeepInsight三维重建软件,重建方法如下:(1)将胸部CT二维图像信息以DICOM格式导人DeepInsight系统中;(2)通过图像加载处理、气管阈值的计算、分别进行气管、血管、淋巴结、肺结节及肺肿物的提取、血管染色等步骤,重建支气管、动静脉血管及淋巴结等模型;(3)进行淋巴结、肺肿物或小结节与支气管及肺动静脉血管分割,评估支气管、肺动脉、肺静脉等解剖结构的分支、直径、走形及变异情况,评估淋巴结、肺结节及肺肿物与支气管、肺动脉、肺静脉等结构的三维空间毗邻关系及侵犯程度,同时准确定位肺结节所处肺段的空间位置,进行精准的术前规划。
-
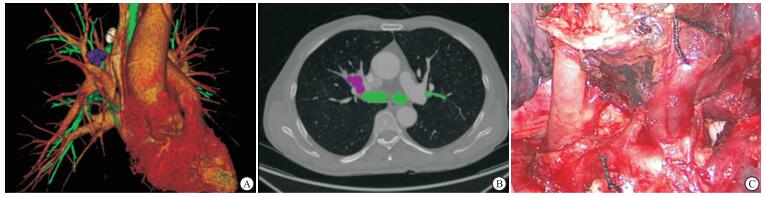
全部采用静吸复合麻醉,双腔气管插管或者封堵管单肺通气状态下手术,侧卧位单孔或单操作孔,操作孔根据病人病变部位及身高等情况选择腋中线附近第4或第5肋间。根据肺裂发育情况及肺血管有无外侵,选择手术顺序为单向式或传统顺序,根据术前重建的三维图像,精准解剖并处理支气管、不全肺裂、肺动静脉及段间平面,避免损伤、误断支气管及肺动静脉。肺癌根治术同时行系统性淋巴结清扫,肺段手术同时行淋巴结采样。手术完成后嘱麻醉师膨肺,检查漏气情况及是否需要加固缝合。在手术同时使用图像融合法与手术同步进行,由助手台下将模型通过旋转、透明化等操作,同步使三维重建图像与术中手术解剖结构一致;在结节定位、肺动静脉及支气管处理等操作时,实时进行验证导航,确保操作精准。全部病人手术均顺利完成,无中转开胸病例(见图 1、2)。
-
术后记录三维重建术前规划及术中导航使用情况, 手术方式, 手术时间、术中出血量、术后拔除胸腔闭式引流管时间及总引流量、术后住院时间等,并观察记录术后并发症,如肺部感染、呼吸衰竭、支气管胸膜瘘、出血、严重液气胸等的发生情况。
1.1. 一般资料
1.2. 方法
1.2.1. 精准术前规划
1.2.2. 手术方法

1.2.3. 临床观察资料
-
全部病人均能够精准地完成术前规划,清晰重建支气管及肺血管解剖结构及变异情况,对中央型肿瘤及肿大淋巴结与血管的关系重建满意,能准确地明确肺结节在肺段中的位置关系及进行精准的术前规划。全部病人均进行术中实时导航,按照术前规划实施手术,手术均顺利完成。
-
全部病人均在单孔或单操作孔胸腔镜下完成手术,其中胸腔镜肺叶根治性切除同时行系统性淋巴结清扫术25例,包括右上肺叶切除8例,右中肺叶切除2例,右下肺叶切除9例,左上肺叶切除3例,左下肺叶切除3例;胸腔镜肺段切除同时行淋巴结采样术25例,其中单肺段13例,联合肺段或肺亚段6例,肺段联合楔形6例;共切除肺部病灶57个。
-
手术时间(147.60±37.77)min,术中出血量(33.82±22.17)mL,术后住院时间(7.02±1.78)d,引流管拔除时间(4.68±1.60)d,术后总引流量(221.00±135.03)mL;围术期无严重并发症及死亡病例。少数病人术后轻度漏气,经引流后均愈合。
2.1. 三维重建术前规划及术中导航使用情况
2.2. 三维重建技术指导下的手术方式
2.3. 围术期观察指标及并发症
-
20世纪,国外率先报道胸腔镜肺叶切除手术[6],近年来科技的进步、设备硬件的研发、微创理念的深入、信息化的发展,微创胸腔镜肺外科快速发展,目前已有单孔、单操作孔、三孔、四孔、剑突下等不同入路胸腔镜手术[7-10];也出现了自主呼吸麻醉下肺癌根治术[11-12];手术适应证及手术技术难度也在发生变化,尤其对T4期局部晚期肺癌根治术,淋巴结粘连或转移、中央型肺癌等手术困难病例或者肺部结节需行肺段、亚段、联合亚段等手术,由于肺部结构的变异造成的困难增加。既往此类病人均通过术前胸部CT进行评估或进行手术规划,具有较大的局限性。CT平扫或增强不论在横断面、矢状面或冠状面均只能表现为二维图像,其对于肿瘤、淋巴结及正常组织结构的空间结构、具体形态及变异情况等信息的传递容易出现误差。同时每个医生所掌握的解剖、影像知识等经验和个体化的空间理解力,很难在不同的医生间沟通、传递在大脑中呈现出的主观性的三维实际图像,且难以进行表述。在单孔或单操作孔胸腔镜下完成肺叶根治性切除同时行系统性淋巴结清扫术和肺段切除同时行淋巴结采样手术中,临床上仍然存在诸多难题,对术前精准手术规划及术中实时导航技术的临床应用要求十分迫切。
近年来计算机及信息技术的发展,出现多种三维重建软件,可以将CT数据通过软件重建出三维图像,其中包括DeepInsight、Mimics、英库等软件[13-15]。重建出的三维图像数据信息能直观地表现出肿瘤、淋巴结与肺部结构的立体关系以及肺结节的空间位置关系和肺部结构的变异情况。三维重建技术在术前可以使医生更准确地进行交流、会诊及手术规划,同时通过软件的操作进行术前虚拟手术,术中将软件重建信息同步与手术所见结构进行验证指导,避免误损伤。因此三维重建技术在微创肺外科的应用对复杂肺切除手术、手术规划及精准定位、避免误损伤、降低手术中转率等都具有十分重要的作用[16-18]。我们在既往的工作中,使用了Mimics软件试用版等,功能强大,重建效果满意,但正版软件昂贵,未能进一步推广使用;一些商业公司软件,制作精美,省时省力,但存在可能出现少量错误及需病人自费等缺点,仅做尝试性使用;DeepInsight软件免费授权,操作简便,按照数据采集的最佳要求进行CT扫描可获得满意的重建效果。
本研究应用DeepInsight软件,通过下载的DICOM数据,进行三维重建、手术规划及虚拟手术用于指导微创胸腔镜肺切除手术。对于肺叶切除加淋巴结清扫术,术中根据肺裂发育情况及肺血管有无外侵,选择手术顺序为单向式或传统顺序,根据术前重建的三维图像,精准解剖并处理支气管、不全肺裂、肺动静脉及段间平面,避免损伤、误断支气管及肺动静脉,同时行淋巴结清扫。无中转开胸及术中意外出血情况,围术期无严重并发症及死亡病例。其解决手术难度主要是将肿瘤体积、解剖、毗邻结构以及生长类型等方面进行重建和虚拟手术。将肿瘤及肺结构立体化,对各种解剖结构与肿瘤、淋巴结空间位置关系进行直观观察,对术中风险进行准确预判,避免术中误损伤各种肺动脉、肺静脉、支气管等结构情况,避免可能出现的肺血管损伤导致的中转开胸甚至无法控制的大出血等情况发生,围术期无咯血、肺不张、严重漏气等严重并发症病例。对于肺结节的肺段切除手术,通过术前三维重建明确肺结节空间定位、肺静脉、肺动脉、支气管等结构的变异、走行及汇合情况,并充分认识支气管、肺动静脉等解剖结构的毗邻关系,术前精准规划最佳手术入路,根据每个病人的不同情况规划个体化肺段切除术。术中按照术前规划,对照三维图像进行操作,均顺利完成手术。所有病人术后均未发生如出血、严重漏气、咯血、肺不张等严重并发症。通过应用三维重建技术及虚拟手术规划制定的微创胸腔镜肺切除手术治疗总体安全可靠。
综上所述,通过术前、术中的三维重建技术,术前对中央型肺癌、肿大淋巴结与肺解剖结构的空间关系进行准确评估,对于肺结节精准定位,同时明确各种解剖异常,进行术前精准手术规划及术中实时导航技术的临床应用,能够精准、高效、安全方便地实施胸腔镜肺叶和肺段切除手术。
 DownLoad:
DownLoad: